
Abstract
Background:
Central airway obstruction (CAO) is a life-threatening situation. Stent insertion re-establishes patency of the central airways. Self-expanding metallic Y stents have been available since 2005, widening the spectrum of interventional bronchoscopic techniques.
Methods:
Retrospective analysis of all patients treated for CAO with a self-expanding metallic Y stent at the Thoraxklinik Heidelberg between May 2005 and January 2009.
Results:
A total of 43 patients aged 26–81 had a metallic Y stent inserted endoscopically for the treatment of CAO; 39 of these patients (90.7%) had CAO due to malignant disease, four patients (9.3%) due to benign disease. In all 43 patients, the Y stent was deployed without any complications. A longitudinal follow up was possible in 32 of the 43 patients. The stents remained in situ for an average of 107.1 days (range 1–640 days). In 29 patients with malignant CAO the stenosis was successfully overcome with a Y stent; 11 of these patients died within 6 weeks following stent insertion. On follow up the remaining 18 patients showed immediate improvement of dyspnoea. Eight out of the 18 patients (44.4%) tolerated the stent without problems, two (11.1%) required further stenting, six (33.3%) had complications such as increased secretions, cough, dyspnoea or granulation tissue formation. The stent was removed in one patient (5.6%) due to increased secretions, and in another (5.6%) as the stent was no longer required due to successful tumour-specific therapy.
Conclusion:
Placement of Y stents in symptomatic CAO allows for quick relief of symptoms. Severe complications are rare. Stent removal is possible after successful treatment of the primary tumour. However, the prognostic indicator for survival is the underlying malignancy.
Keywords
Introduction
Central airway obstruction (CAO) describes a reduced lumen at the level of the trachea, main carina and the main bronchi. This has many different causes, however in most cases it is due to malignancy. Most central airway stenosis is caused by lung cancer [Breitenbücher et al. 2008], but other malignancies such as lymphoma, oesophageal cancer and metastases of a distant primary can also be the cause. In 30% of all lung cancers a stenosis of the central airways can already be found at the time of diagnosis [Dutau et al. 2004].
Central airway stenosis can also be present in people with benign conditions such as scar tissue, chronic inflammatory diseases and benign tumours, and in rare cases, extraluminal haematoma. Diseases such as tracheobronchomalacia and excessive dynamic collapse of the airways can also be considered as an unfixed airway stenosis.
The main symptoms of central airway stenosis are dyspnoea and cough. These symptoms develop rapidly and with increasing airway obstruction represent an acute life-threatening state requiring urgent intervention.
Besides mechanical and thermal endoscopic procedures to alleviate the acute obstruction, stents have been available for over 20 years for the treatment of central airway stenosis. Metallic Y stents restore patency of the airways and relieve symptoms of CAO immediately. The first Y stent was developed in 1972 by Neville and colleagues and was a silastic stent [Neville et al. 1972]. In the following years airway stents were developed further and a tracheostomy was no longer necessary for their placement. Another aim in the development of stents was improved biocompatibility, which was associated with a lower risk and side effects profile. Nowadays different Y stents are available, which differ in material, rigidity and insertion technique.
To obtain the best possible results, different endoscopic techniques are combined [Cavaliere et al. 1996]. After mechanical debriding of the central airway stenosis, the insertion of a stent prolongs the interval to restenosis [Cavaliere et al. 1996].
Materials and methods
This retrospective analysis includes all patients with CAO treated with a self-expandable metallic Y stent at the Thoraxklinik Heidelberg between March 2005 and January 2009. The study protocol was presented to and approved by the ethics committee.
We evaluated patient characteristics, cause of obstruction, stent duration and stent complications with the help of patient charts and bronchoscopy records. All patients received a self-expanding Y stent (ECO-Y-Stent, Leufen MT, Germany) (Figure 1). These stents consist of a nitinol mesh and are covered by a thin polymer membrane excluding the distal 5 mm intended for the right main bronchus to prevent closure of the right upper lobe. This self-expandable metallic Y stent cannot be adjusted for length, but different sizes are available. The stent used in the patients included in this retrospective analysis had the following dimensions: the tracheal limb was 20 mm in diameter and 50 mm in length; the bronchial limb was 14 mm in diameter and 15 mm in length on the right side and 30 mm in length on the left side.

Self-expanding Y stent (ECO-Y-Stent, Leufen MT, Germany).
Stents were placed during a rigid bronchoscopy under general anaesthesia, with high-frequency jet ventilation and the aid of fluoroscopy. Guide wires were advanced into the right and left main bronchus via the flexible bronchoscope and the stent was then inserted into the correct position with an applicator using the Seldinger technique. First the limbs of the Y stent were deployed and then the tracheal part of the stent was released. The correct position of the stent could then be confirmed using the flexible bronchoscope (Figure 2).

Implanted Y stent.
Results
Patient characteristics
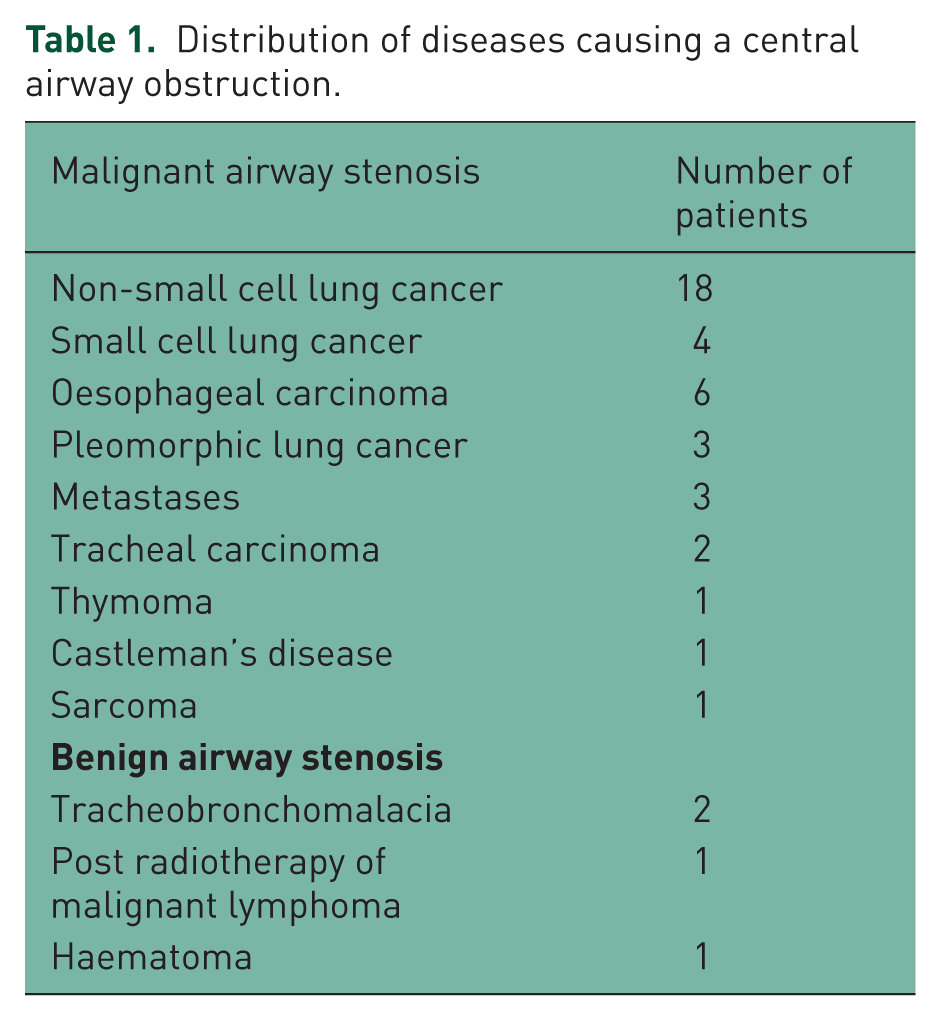
Between March 2005 and January 2009 we treated 43 patients with central airways obstruction using a self-expandable metallic Y stent at the Thoraxklinik Heidelberg. These patients were aged between 26 and 81 years, and the male:female ratio was 1.15:1. Thirty-nine patients had a malignant cause for their stenosis and four patients a benign cause. The most common cause for the CAO was non-small cell lung cancer. Table 1 shows the distribution of diseases.
Distribution of diseases causing a central airway obstruction.
Follow up after stent placement
Stent insertion in all 43 patients was performed without complications. We were only able to retrospectively evaluate all the data in 32 of these 43 patients, including duration the stent remained in situ, stent complications and the individual course of the disease. Follow-up data are based on clinical symptoms and radiological results. Bronchoscopic controls were performed in the case of pathological findings. The remaining 11 patients had incomplete data because they had not attended further follow up, they had changed to an unknown physician or were being treated in a different country after the procedure. One of these patients had received stent placement for the treatment of tracheomalacia; the other 10 patients had malignant airway stenosis and two of these also had a tracheo-oesophageal fistula.
Malignant airway stenosis
In the 32 patients studied, malignancy was the cause of airway stenosis in 90.6% (29 patients), lung cancer being the most common malignancy (72.4%). In all patients the stent was deployed during rigid bronchoscopy without complications and this led to immediate relief of symptoms of the central airway stenosis. Figures 3(a)–(d) show computed tomography scans of a patient with severe malignant central airways stenosis prior to and following Y stent implantation, demonstrating the re-establishment of the airway patency. The average duration the stent remained in situ was 107.1 days, ranging from 1 to 640 days. 11 out of the 29 patients died within 6 weeks, so that long-term outcome could be evaluated in 18 patients. Placement of the Y stent achieved patency of the central airways, but two of the 18 patients (11.1%) required further stenting of a main bronchus after 1–2 months due to progressive endobronchial tumour growth. Eight of the 18 patients (44.4%) tolerated the stent without complications. Six patients (33.3%) had minor complications, such as granulation tissue formation at the stent site (Figure 4), cough, increased secretions (Figure 5) or dyspnoea. Within the first 6 weeks, one patient (5.6%) had his stent removed due to significantly increased secretions and retention of secretions. Another patient (5.6%) had his stent removed after successful tumour-specific therapy which reduced the amount of stenosis and rendered the stent unnecessary. All 29 patients with malignant airway obstruction died within 1 day to 22 months after stent insertion; 11 of the 29 patients (37.9%) within 6 weeks. One patient died 1 day following stent insertion. This patient had non-small cell lung cancer with severe central airway stenosis but also multiple pulmonary metastases. After admission to hospital, the patient had to be resuscitated due to hypoxic cardiovascular failure. After successful resuscitation, she underwent Y stent implantation. Afterwards she was extubated and experienced an immediate relief of dyspnoea. However, the following day, the general condition of this patient got worse and she died. Death in this case was attributed to the advanced underlying malignant disease and not to the stent insertion itself. Overall, the mean survival time following stent insertion, excluding two patients in whom the stent was explanted again, was 122 days. Diagram 1 summarizes follow up of the 29 patients following stent implantation.
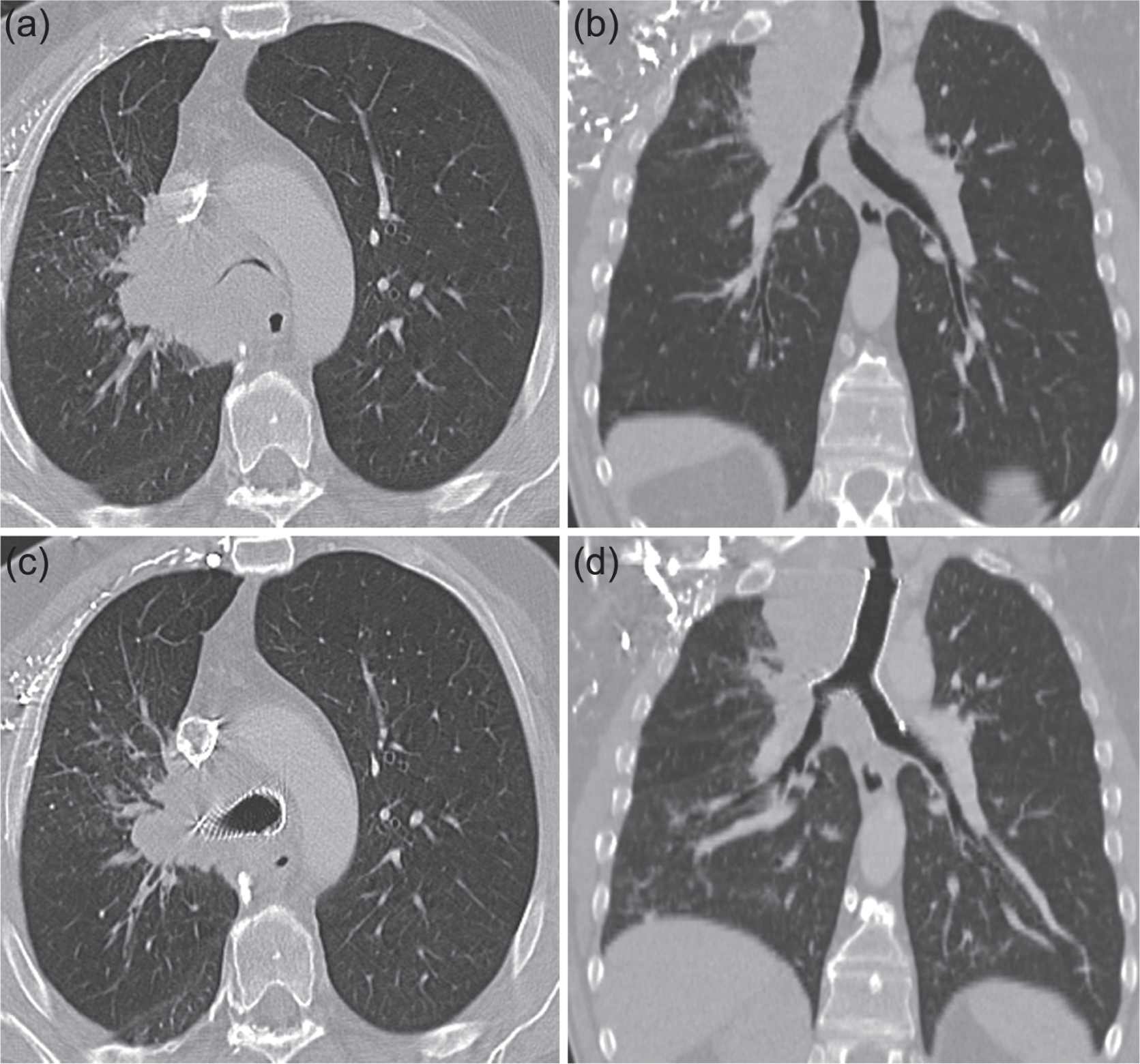
Computed tomography scans of a patient with severe malignant airway stenosis prior to Y-stent implantation (a, b) and after Y-stent implantation (c, d).

Granulation tissue formation.

Retention of secretion within the stent.

Follow up of 29 patients with stent implantation because CAO due to malignancy. 11 patients died within the first 6 weeks due to underlying malignancy. Long-term follow up and evaluation of stent-associated complications were collected in 18 patients.
Benign airway stenosis
One of the four benign stenoses (25%) had developed due to previous thoracic radiotherapy to treat non-Hodgkin lymphoma (scarring). In this patient, a larger stent was required within 2 months. Two patients with tracheomalacia received a Y stent to assess the potential benefit of airway stabilization. If there was clinical improvement a surgical tracheoplasty was then planned. A follow up was only available for one out of these patients in whom the stent was removed after 3 days due to a lack of clinical improvement. The second patient benefited from the stent in the first days following stent implantation, but further follow up is missing. One patient had tracheal stenosis due to extraluminal compression from a haematoma sustained during a ruptured thoracic aortic aneurysm.
Discussion
CAO or peripheral airway obstruction can be caused by malignant disease and less frequently by benign conditions. The most common cause of endoluminal narrowing or obstruction is lung cancer, which represents 25% of all cancers in Europe at an incidence of 52 per 100,000 per year [Midthun and Jett, 2008]. Lung cancer is the most common cause of death from cancer in men and the second most common in women. In 2013, The estimated age-standardized mortality rate is 37.1/100.000 for lung cancer in men and 13.9/100.000 in women [Malvezzi et al. 2013]. Airway stenosis is present in 30% of cases at the time of diagnosis [Dutau et al. 2004], manifesting itself as dyspnoea, apnoea in the case of complete airway obstruction, post-stenotic pneumonia or haemoptysis. CAO is a life-threatening complication. Compensation mechanisms can maintain a stable respiratory state, but if the maintained lumen of the central airways is less than 5 mm, respiratory decompensating results [Prakash, 1997; Becker et al. 2003]. Approximately 50% of patients with CAO have an endoscopic procedure as an emergency with acute respiratory compromise [Herth and Eberhardt, 2007].
Endoscopic techniques can be divided into rapidly active and long-acting treatments. Mechanical and thermal tumour debridement as well as the insertion of stents show an immediate effect while photodynamic therapy or endoluminal brachytherapy have a delayed effect. The different techniques should be combined to achieve the best results possible if endobronchial therapy is an option [Santos et al. 2004].
The primary aim of endoluminal stent insertion for tumour-associated stenosis is the immediate relief of symptoms associated with the stenosis. There are currently many different endobronchial stents available for the treatment of CAO and for covering fistulas [Freitag, 2000]. When the main carina is involved anatomically shaped Y stents can be used, for which different types are available. The first bifurcation stent was developed by Neville in 1972. In 1982, Westaby and colleagues developed a bifurcated rubber stent [Westaby et al. 1982]. This long and rigid stent often caused significant problems with cough and is hence only rarely used in extensive tracheal stenosis with involvement of the main carina. The Orlowski Y stent is used specifically to treat tracheal strictures but due to retention of secretions it requires frequent rebronchoscopy [Orlowski, 1987]. Another Y stent is the Hood Y stent, which is softer than the other available stents and has a certain amount of give on coughing. One of the most commonly used Y stents is the Dumon Y stent, which is made of silicone and has small studs on its exterior surface for better fixation and reduction in risk of migration [Dumon, 1990]. This stent is inserted via a Dumon–Efer bronchoscope with a specific introducer system. Once in the trachea it is positioned into its final position with the help of a rigid forceps. The Dynamic Stents are hybrid stents consisting of metal and silicone with a flexible membrane in the position of the posterior tracheal wall [Freitag et al. 1994]. The membrane gives under coughing, hence improving the action of coughing and reducing the amount of secretion retention. The Y stent is implanted using grasps under visual control with a laryngoscope.
All patients evaluated in this retrospective analysis had a self-expandable nitinol stent (ECO-Y-Stent, Leufen MT, Germany) inserted, which has been available since 2005 (nitinol consists of a metal ligation of nickel and titanium). These stents possess a so-called memory effect, meaning that the stent will return to its original shape after having been deployed. Self-expandable metallic stents (SEMS) are characterized by an optimal cross-sectional airway diameter. Furthermore these stents offer a precise adaptation to irregular airways. The metallic Y stents are implanted by using introducer systems that are advanced over two guide wires under fluoroscopic control. The advantage of this stent, compared with the previously mentioned stents, is the ease of insertion into the bronchial system. However, rigid bronchoscopy is recommended as it is easier to control any potential complications. In our retrospective study, all 43 patients with central airway stenosis had an immediate improvement in their respiratory symptoms following stent placement. This result complies with observations in previously published trials by Yang and colleagues in which five patients were treated by Y-shaped metallic stent insertion [Yang et al. 2007] and by Han and colleagues in which 35 patients received metallic Y stents [Han et al. 2008].
It should be kept in mind that this stent is no physiological replacement for a stenosed airway [Herth and Eberhardt, 2007]. By changing the mechanics as well as the characteristics of the mucosal surface one has to expect stent-associated complications. One of the most common complications of all airway stents is migration of the stent. By attaching rings or studs to the outer surface of the stent, mucosal contact is improved and the risk of migration is reduced. Despite this, in cases of reduction of the tumour size under tumour-specific therapy, the diameter of the airway increases and the contact between the stent and mucosa decreases, leading to stent migration. However, the risk of migration is rarely seen in Y stents, since they imitate the bifurcation and attach to the main carina. Another complication, retention of secretions, is often seen with Y stents. Under normal physiology sputum is usually transported via the ciliae towards the mouth. When larger amounts of sputum are produced, for example during an infection or inflammation, the action of coughing also transports the sputum out of the lungs. Since the ciliae cannot function when a polymeric or covered metal stent is in place, the sputum cannot be readily transported outwards. Furthermore, with rigid stents the effectiveness of the cough is limited, leading to retention of sputum within the stent. This in turn can lead to bacterial ‘infestation’ of the mucous layer, causing infections. The most common bacteria colonizing the stent biofilm are Pseudomonas aeruginosa, Staphylococcus aureus, Streptococcus pneumoniae and Klebsiella spp. [Noppen et al. 1999]. Granulation tissue or tumour regrowth at the distal or proximal end of the stent, or within the stent in the case of uncovered metal stents, are further complications. The stent causes constant pressure on the mucosa, which leads to growth of the mucosa causing granulations. These in themselves can lead to reobstruction of the airway with dyspnoea. In these cases frequent bronchoscopies are performed to remove the granulation tissue preferentially with cryotherapy.
In our retrospective analysis we were able to show that in nine of the 18 cases who lived longer than 6 weeks (50%) complications such as granulation tissue, retention of sputum or restenosis proximal or distal to the stent lead to the need for repeated endoscopic interventions. Stent placement should be seen as a temporary palliative intervention, relieving symptoms of obstruction and improving quality of life and also to bridge the time required to start a tumour-specific therapy such as radio- or chemotherapy [Swartman, 2011; Kim et al. 2009]. In our retrospective study there was one patient with CAO due to small cell lung cancer who had not received any tumour-specific therapy prior to stent implantation. After successful therapy the stent could be removed. A study of 22 patients showed that endoscopic stent placement in central airway stenosis was used as a bridging method prior to adjuvant antineoplastic therapy [Witt et al. 1997]. In 50% of patients with airway stenosis due to lung cancer, lymphoma or metastases it was possible to remove the endobronchial stent after an average of 31.7 days. It is important to point out that in our analysis the amount of stenosis reduction after tumour-specific therapy was 5.6, far below the 50% published by Witt and colleagues. This is probably due to the fact that in our retrospective analysis we not only included patients with locally advanced cancer who had not received any treatment prior to stent placement, but we also included patients with advanced cancer who had received several tumour-specific therapies prior to stent implantation.
In a prospective study, Furukawa and colleagues showed that the average survival time of an untreated patient with stenosing lung cancer, who after stent implantation received adjuvant tumour-specific therapy, was 5.6 months [Furukawa et al. 2010]. In patients with a lower Eastern Cooperative Oncology Group score, however, in whom adjuvant therapy is not possible and stent placement represents a final palliative measure, the medium survival is only 1.6 months [Furukawa et al. 2010]. Therefore indications for stent placement need to be divided into a bridging method prior to commencing adjuvant therapy and final palliative therapy for relief of symptoms. For palliative therapy, stent placement needs to be discussed on an individual basis and with strict criteria due to the previously mentioned possible complications. In our study we were able to show that 37.9% of patients died within 6 weeks of stent placement due to their underlying malignancy and therefore in such patients the benefit is questionable. Despite this, stent insertion should be considered as a palliative intervention in patients with advanced lung cancer, as shown by one retrospective study of general practitioners (GPs) involved in the palliative care of patients at home [Vonk-Noordegraf et al. 2001]. These GPs considered stent placement for the immediate relief of symptoms as a useful palliative measure in 58% of patients with central airway stenosis.
In conclusion, insertion of a Y stent in central airway stenosis caused by underlying malignancy leads to immediate splinting of the central airways. The self-expanding Y stent made of nitinol is simple to place, leads to an improvement in quality of life and in some cases buys time until a tumour-specific therapy can be initiated. The defining prognostic factor for the further survival of the patient with malignant airway stenosis is the course of the underlying malignancy.
Insertion of endobronchial stents is not only possible in patients with malignant stenosis but also in those with benign airway stenosis. However, in these patients surgery remains the ‘gold standard’ treatment to avoid the complications that are associated with stent implantation. If surgery is not possible, stent implantation presents an alternative therapeutic approach. In general, silicone stents are the preferred option in benign conditions because they can be removed very easily and are not associated with risk of stent fracture. However, one retrospective cohort analysis revealed safe removal of SEMS in patients with benign disorders [Noppen et al. 2005]. Therefore, SEMS can be used in patients in whom silicone stents are unsuitable and difficult to implant. Besides easier implantation, the advantages of SEMS compared with silicone stents are greater cross-sectional airway diameter and a better adaptation to irregular airways. However, it should be borne in mind that, particularly in patients with benign stenosis, stents are associated with a high rate of complications. In one 2011 published trial 77 patients with malignant stenosis and 72 patients with benign central airway stenosis underwent implantation of self-expandable metallic stents [Chung et al. 2011]. Although, patients with benign diseases experienced better clinical outcome following stent placement, the overall complication rate in patients with benign disorders was 42.2%, and thus significantly higher than in patients with malignancies (21.1%).
Tracheobronchomalacia and excessive dynamic collapse of the airway can also broadly be considered as a central airway stenosis though not fixed. Different therapy options are available, such as stent insertion and tracheoplasty with stenting of the posterior wall of the airway. In our retrospective analysis two patients with severe tracheomalacia had a self-expanding Y stent inserted, and one of the patients benefited from this. A prospective study by Ernst and colleagues showed that 77.6% of all patients with tracheobronchomalacia benefited from stent placement, but complications such as retention of secretions, infections and stent migration were seen in 84.5% of cases [Ernst et al. 2007]. Owing to the high frequency of stent complications, stent insertion should only be considered a temporary intervention. If the patient shows clinical benefit they should be referred for tracheoplasty, which leads to improvement in dyspnoea, exercise tolerance and hence quality of life [Majid et al. 2009].
A further cause for benign central airway stenoses are scar strictures, which occur mostly after intubation or tracheostomy [Kelsey et al. 2006]. Radiotherapy in the treatment of lung cancer can also lead to scar tissue, with resulting airway stenosis. In one study reported that, 3 months after percutaneous high-dose radiotherapy, a significant narrowing of the airways can be observed [Kelsey et al. 2006]. Insertion of endobronchial stents for scar stenoses maintains central airway patency, whilst accepting the known stent-induced complications [Martinez-Ballarin et al. 1996]. Stent insertion is an alternative to surgical intervention in benign scar strictures if the patient is not a suitable candidate due to high operative risk.
One patient in our study had an extraluminal obstruction secondary to a haematoma from a contained rupture of a thoracic aortic aneurysm. By inserting a stent, central airway patency could be maintained, but the 72-year-old patient died later as a result of the aneurysm. We were nevertheless able to show that the central airways can be splinted by insertion of a stent in the case of extraluminal compression by a haematoma. This was also demonstrated in a case report of a 27-year-old with CAO following operative repair of an aortic dissection who had a temporary stent successfully inserted [Elgandli et al. 2009].
In conclusion, insertion of self-expanding Y stents is an option in the treatment of benign airway stenosis. In view of frequent stent-associated complications, this procedure should only be used as a temporary solution and only as a more long-term alternative in the case of inoperability.
Summary
Insertion of self-expanding metal Y stents in central airway stenosis caused by underlying malignant disease leads to rapid improvement of symptoms by splinting of the central airways. This technique can be used as a bridging method prior to commencing tumour-specific therapy and also as a palliative intervention in advanced tumour stages. Stent-associated complications are retention of secretions, formation of granulation tissue, cough and dyspnoea. Y stents are also an option in benign bifurcation stenosis to maintain airway patency, but in view of the frequent stent-associated complications the criteria need to be strict.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.