
Abstract
Background:
Roflumilast, a phosphodiesterase 4 inhibitor, has been shown to improve lung function and reduce exacerbation rates, but is associated with adverse events (AEs). The purpose of this study was to systematically review the clinical effectiveness and safety of roflumilast.
Methods:
A systematic search was made of MEDLINE, Cochrane trials database, DARE and CINAHL. Randomized, controlled trials of more than 12 weeks’ duration comparing roflumilast with placebo were reviewed. Studies were pooled to yield relative risk (RR), incident rate difference or weighted mean differences with 95% confidence intervals (CIs).
Results:
Eight trials (8698 patients) met the inclusion criteria. Roflumilast significantly reduced moderate to severe exacerbations (RR 0.85; 95% CI 0.80−0.91) compared with placebo, but not severe exacerbations (RR 0.83; 95% CI 0.68–1.01) or mortality (RR 0.90; 95% CI 0.63–1.28). Roflumilast significantly improved lung function relative to placebo, but not quality of life measures. AEs (RR 1.11; 95% CI 1.03–1.19) and discontinuations of treatment due to AEs (RR 1.63; 95% CI 1.45–1.84) were significantly more frequent with roflumilast than placebo. In the chronic obstructive pulmonary disease (COPD) Safety Pool (12,054 patients), the overall incidence of serious AEs did not differ between groups. However, atrial fibrillation (0.4% versus 0.2%; p = 0.02) and suicidality (0.08% versus 0%) were more frequent with roflumilast than placebo.
Conclusions:
The efficacy of roflumilast appears modest compared with other available therapies for COPD. Further studies are needed to investigate the risk–benefit ratio and long-term safety of roflumilast before its wider use.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) continues to be a major cause of disability, mortality and healthcare costs worldwide. In 2005, 210 million people were diagnosed with COPD worldwide and 3 million died of the disease. In the USA, it is estimated that more than 12 million people are affected by the disease and COPD has become the third leading cause of death after cardiovascular disease and malignancy [Kochanek et al. 2011]. It is predicted that COPD will also become the third leading cause of death worldwide by 2030 [Halbert et al. 2006].
The clinical efficacy of currently available therapies is still suboptimal despite the advances in medical technology. Continuous oxygen therapy and smoking cessation are the only interventions shown to reduce mortality. There is a pressing need for additional intervention for patients with COPD, as no existing treatment has been shown to reduce disease progression [Barnes, 2008].
Roflumilast is a selective phosphodiesterase 4 (PDE4) inhibitor that leads to decreased recruitment and activation of proinflammatory cells and decreased production and release of proinflammatory cytokines in lung cells. Although the exact mechanism by which roflumilast exerts its therapeutic action is not completely understood, it is thought to be related to increased intracellular cyclic adenosine monophosphate production in the lung tissues and inflammatory cells. Clinical studies have shown that roflumilast improves lung function and reduces exacerbations [Kelly Freeman, 2012].
The US Food and Drug Administration (FDA) approved roflumilast in March 2011 for clinical use to reduce the risk of COPD exacerbations, although an advisory panel of outside experts had opposed it by a 5 to 10 vote. The advisory committee felt that a small improvement in lung function did not outweigh its significant side effects, which primarily consisted of gastrointestinal and psychiatric problems, including suicidal behavior, which led to increased withdrawal from clinical studies [FDA, 2010]. Roflumilast was finally approved by the FDA after its indication was made more restrictive and a warning about the psychiatric side effects was added to the drug label. The place and role of roflumilast in COPD management are currently unclear. The purpose of this study was to systematically review the clinical effectiveness and safety of roflumilast, the first-in-class orally active PDE4 inhibitor in the USA and a number of European countries.
Methods
Identification of trials
We identified all relevant clinical trials that studied clinical efficacies and safety of roflumilast. We independently searched the National Library of Medicine’s Medline database for studies in any language published from 1946 to 2 March 2012 using the Medical Subject Headings and keywords: Phosphodiesterase Inhibitors or roflumilast AND Pulmonary Disease, Chronic Obstructive or COPD. In addition, we searched the Cochrane Central Register of Controlled Trials, the Database of Abstracts of Reviews of Effects and the Cumulative Index to Nursing and Allied Health Literature (CINAHL). We also reviewed our personal files and searched the internet for relevant information. Bibliographies of all selected articles and review articles that included information on roflumilast in COPD were reviewed for other relevant articles.
Study selection and data extraction
Both authors independently abstracted data from all studies using a standardized form. Data were abstracted on study design, study size, population, severity of illness and the impact of roflumilast on the endpoints of interest. Disagreements regarding values or analyses were resolved by discussion.
To be included in the analysis, a study had to be a randomized, controlled trial comparing the clinical effectiveness of roflumilast with that of placebo and had to have at least one of the following as a primary outcome variable: forced expiratory volume in 1 s (FEV1), COPD exacerbation, quality of life score or mortality rate. The quality of included studies was evaluated using the Consolidated Standards of Reporting Trials (CONSORT) criteria [Moher et al. 2010]. Each study was given a score out of 25, reflecting how many of the 25 CONSORT items were complied with (each item being given equal weighting). Our meta-analysis was conducted in accordance with the Quality of Reporting of Meta-analyses of Randomized Control Trials statement [Moher et al. 1999].
Data analysis
Mortality, adverse event (AE) and exacerbation rates were dichotomous variables. FEV1 and quality of life scores were continuous variables. The data analysis was performed using meta-analysis software (StatsDirect 2.7.8, StatsDirect Ltd, Cheshire, UK). The results were expressed as relative risk (RR) or incidence rate difference (IRD) for dichotomous outcomes and weighted mean difference (WMD) for continuous outcomes, along with their 95% confidence intervals (CIs). A Z-test was performed to examine the overall effect. We tested heterogeneity between trials with the I2 statistic. I2 indicates the proportion of between-study heterogeneity that is beyond chance and ranges between 0% and 100%; higher I2 values indicate higher amounts of heterogeneity. We used the DerSimonian and Laird random-effects model to pool rate differences across studies.
Sensitivity analyses
Sensitivity analyses were performed to assure the robustness of the results by excluding the clinical trials one by one from the pooled analyses and using odds ratio and risk difference. A multivariate regression meta-analysis was performed to identify a subgroup in which roflumilast could be more efficacious to reduce moderate to severe exacerbations. The variables included were mean age, baseline FEV1, duration of the clinical trials, concomitant use of tiotropium or salmeterol, and history of prior COPD exacerbations. Meta-regression analyses were performed using Stata 10 (StataCorp LP, College Station, TX, USA).
Results
Study selection
The electronic database searches identified 104 citations. Ninety-five studies were excluded on more detailed review. The remaining nine studies were reviewed for duplicate publications. Two studies were excluded for duplication [Bateman et al. 2011; Rutten-van Molken et al. 2007]. One study was excluded due to crossover design [Grootendorst et al. 2007]. We found that two studies included two separate trials. We included six publications reporting the total of eight clinical trials (Figure 1) [Calverley et al. 2007, 2009; Fabbri et al. 2009; Lee et al. 2011; Rabe et al. 2005; Rennard et al. 2011]. Detailed information on AEs which were not included in the original studies was found on the internet (COPD Safety Pool) [Forest Research Institute, 2010]. These safety data included the total of 12,054 patients (6972 receiving roflumilast) enrolled in 14 controlled parallel group studies including all eight studies used in our meta-analysis except for the study by Lee and colleagues [Lee et al. 2011]. This database was used in additional analyses for AEs and mortality.

Flow of Study Selection.
Study characteristics and patients
Characteristics of included studies are summarized in Table 1. The duration of studies ranged from 12 to 52 weeks. A total of 8698 patients with COPD were included in this analysis; 4459 were treated with roflumilast (500 μg a day) and 4239 received placebo. The mean age of included patients was 64.2 and 74% were men. The mean prebronchodilator FEV1 was 1.14 liters and 41% of predicted. Short-acting β agonists were allowed for rescue treatment in all studies. Concomitant use of inhaled corticosteroid (ICS; ≤2000 μg equivalent to beclomethasone) was allowed in two trials. The CONSORT score ranged from 20 to 24 and the mean score was 22. All studies were sponsored by the same pharmaceutical company and the sponsor was involved in the data interpretation and preparation of manuscripts.
Clinical trials.

Requiring over 16 h a day.
CONSORT, Consolidated Standards of Reporting Trials; CPA, clinically significant cardiopulmonary abnormalities; ECG, clinically relevant electrocardiogram findings not related to chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 s; ICS, inhaled corticosteroid; LTOT, long-term oxygen therapy.
Exacerbations
The definitions of exacerbations varied among studies and are summarized in Table 2. We examined the event rates per patient year as well as the number of patients experiencing at least one exacerbation. The results are shown in Table 3. The rate of overall exacerbations (mild, moderate or severe) was significantly reduced with roflumilast compared with placebo (IRD −0.41 events/patient year; 95% CI −0.72 to −0.11). The rate of moderate or severe exacerbations was also lower with roflumilast than placebo (IRD −0.14 events/patient year; 95% CI −0.22 to −0.06) (Figure 2). However, this was primarily driven by moderate exacerbations as evidenced by no significant difference in the rate of severe exacerbations between groups (IRD −0.01; 95% CI −0.04 to 0.02; p = 0.49) (Table 3).
Definitions of exacerbations.

SABA, short-acting β agonist.
Exacerbation rates.
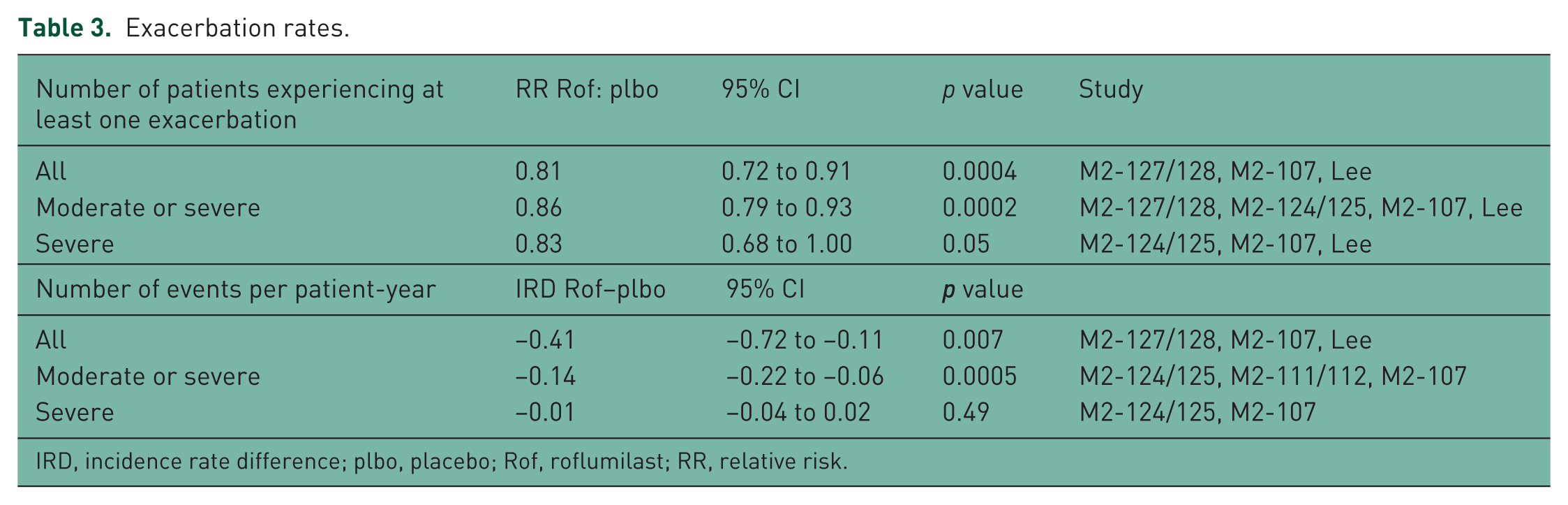
IRD, incidence rate difference; plbo, placebo; Rof, roflumilast; RR, relative risk.

Summary effects of roflumilast on relative risk (a) and incident rate difference (b) of moderate and severe exacerbations.
Health status
Three trials evaluated health-related quality of life using St George’s Respiratory Questionnaire (SGRQ) score (range 0–100, with lower scores indicating a better quality of life; a minimum clinically important difference in the total score being 4 points) [Calverley et al. 2007; Rabe et al. 2005; Rennard et al. 2011]. Improvement in SGRQ scores was greater with roflumilast compared with placebo. However, the difference was not statistically or clinically significant (pooled WMD −1.32; 95% CI −3.20 to 0.55; p = 0.07). M2-124 and M2-125 trials [Calverley et al. 2009] reported Euroquol 5-dimension scores and found no difference between roflumilast and placebo groups (pooled WMD 0.002; 95% CI −0.01 to 0.017; p = 0.76).
Lung function
Small improvement in mean prebronchodilator FEV1 was observed with roflumilast (range 9 to 65 ml) in all studies whereas it was decreased or relatively unchanged with placebo (range −42 to 8 ml). Compared with placebo, improvement in prebronchodilator FEV1 was significantly greater with roflumilast (pooled effect size WMD 55 ml; 95% CI 42–68; p < 0.0001) (Figure 3). A similar result was noted for other lung function parameters (Table 4).

Summary effects of roflumilast on prebronchodilator forced expiratory volume in 1 s.
Improvement in lung function with roflumilast compared with placebo.

FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; WMD, weighted mean difference.
Safety
All included studies reported AEs occurring in at least 2% of patients [Calverley et al. 2007, 2009; Fabbri et al. 2009; Lee et al. 2011; Rabe et al. 2005; Rennard et al. 2011]. A total of 8696 patients were included in the safety analysis. Among 4459 patients receiving roflumilast 500 μg, 1392 and 2864 were exposed for 6 months and 1 year, respectively. In the pooled analysis, 47% and 28% of patients in the roflumilast and placebo groups reported at least one AE (RR 1.11; 95% CI 1.03–1.19). Discontinuation of treatment due to AEs was significantly more frequent with roflumilast compared with placebo (15% versus 9.2 %; RR 1.62; 95% CI 1.44–1.83; p < 0.0001) (Table 5). Gastrointestinal (diarrhea, nausea and decreased appetite), nervous system (headache, dizziness and tremor), psychiatric (insomnia) and constitutional AEs (weight loss) were significantly more common with roflumilast compared with placebo (Table 5). Infectious AEs were more common with placebo compared with roflumilast but the difference was not statistically significant.
Adverse events that occurred in 2% or more of patients.

AE, adverse event; CI, confidence interval; NNH, number needed to harm; RR, relative risk.
The all-cause mortality rate was reported in four trials including 5014 patients [Calverley et al. 2007, 2009; Lee et al. 2011]. None of the studies were sufficiently powered to detect a difference in mortality. The mortality rate did not differ between the roflumilast and placebo groups (2.2% versus 2.5 %; RR 0.90; 95% CI 0.63–1.29; p = 0.56) (Figure 4). In the COPD safety pool, 84 deaths (1.5%) were reported in the 500 μg roflumilast group and 86 (1.6%) in the placebo group (p = 0.69) [Forest Research Institute, 2010]. COPD (25%) and pneumonia (11%) were the most common causes of death. None of the deaths were considered likely or definitely related to the study medication [Forest Research Institute, 2010].

Summary effects of roflumilast on mortality.
The incidence of serious AEs (SAEs) was reported in six trials comprising 7022 patients [Calverley et al. 2007, 2009; Lee et al. 2011; Rabe et al. 2005; Rennard et al. 2011]. In our pooled analysis, SAEs occurred in 17.5% and 18.4% with roflumilast and placebo. The difference between the groups was not statistically significant (RR 1.06; 95% CI 0.86–1.33; p = 0.57; I2 = 55%). In the COPD safety pool including the total of 11,257 patients (500 μg roflumilast = 5766; placebo = 5491), COPD-related SAEs were significantly less frequent with roflumilast (5.8% versus 7.1%; p = 0.008), but atrial fibrillation was more common with roflumilast compared with placebo (0.4% versus 0.2%; p = 0.02) [Forest Research Institute, 2010]. Respiratory failure, myocardial infarction and chest pain were reported more frequently with placebo but the differences were not statistically significant. Overall incidence of SAEs was also similar between the roflumilast and placebo groups (13.5% versus 14.2%; p = 0.3) (Figure 5). Rare but serious psychiatric SAEs were also reported in the COPD safety pool [Forest Research Institute, 2010]. There were three completed suicides (0.05%) (one while on the medication and two > 3 weeks after discontinuation) and two suicide attempts (0.03%) in 6563 patients treated with roflumilast (500 μg = 5766; 250 μg = 797) and no completed or attempted suicides in 5491 patients on placebo [Forest Research Institute, 2010].

Summary of serious adverse events from COPD Safety Pool. A-fib, atrial fibrillation; COPD, chronic obstructive pulmonary disease; MI, myocardial infarction; SAE, serious adverse event.
Sensitivity analyses
Sensitivity analyses using odds ratio and risk difference did not affect the results. Excluding the clinical trials one by one from the pooled analyses did not affect the results. Funnel plots as well as the Begg-Mazumdar (Kendall’s tau) and Egger tests showed no evidence of publication bias for the all efficacy and safety endpoints except for the pooled analysis for SAEs (Egger test, p = 0.004). The univariate and multivariate regression meta-analyses failed to identify any subgroup in which roflumilast would be more efficacious to reduce moderate to severe exacerbations. None of the variables, including mean age, FEV1, duration of the clinical trials, concomitant use of tiotropium bromide or salmeterol and history of prior exacerbations significantly affected the study results.
Discussion
Our meta-analysis and systematic review confirmed that roflumilast improved lung function compared with placebo. However, no significant difference was noted in the mortality rate and health-related quality of life between groups. The rate of moderate to severe exacerbations was significantly lower with roflumilast but the rate of severe exacerbations did not differ between groups. Discontinuation of treatment due to AEs was significantly more frequent with roflumilast and overall incidence of AEs was also significantly increased with roflumilast. The overall incidence of SAEs did not differ between groups in our pooled analysis as well as in the COPD safety pool. COPD-related SAEs were less frequent but the incidence of atrial fibrillation was significantly more common with roflumilast compared with placebo. In the COPD safety pool, suicidality was more common with roflumilast (0.08 versus 0%).
Considering all the clinically pertinent and statistically significant findings, if 1000 patients with moderate to severe COPD are treated with roflumilast for 1 year, 140 moderate to severe exacerbations (primarily moderate ones that would require a short course of therapy with antibiotics or prednisone) would be avoided, however 200 patients would experience at least one AE, of which 60 would discontinue the medication, 2.5 patients would develop atrial fibrillation and 0.8 patients would attempt suicide, of which 0.5 patients would succeed. Overall quality of life would not be affected with the additional cost of $207 a month [Anonymous, 2011].
Although roflumilast is approved for patients with COPD with severe and very severe airflow limitation and a history of exacerbations, its place in the current armamentarium of COPD treatments and the risk–benefit ratio are still at the center of debate [Puhan, 2011]. It is concerning that another PDE4 inhibitor, cilomilast, was rejected by the FDA advisory panel in September 2003, based on concerns over the efficacy of the agent, as well as gastrointestinal side effects. However, the FDA temporarily approved cilomilast in October 2003 but the final approval is contingent on the outcome of additional efficacy and safety studies [Giembycz, 2006], which are still ongoing. The risk–benefit ratio of the entire class of orally active PDE4 inhibitors appears to be in question.
Some patients continue to have symptoms or repeated exacerbations despite combination therapy with a long-acting β agonist (LABA) and ICS. Additional pharmacological treatment options in such a refractory disease may include a long-acting muscarinic antagonist (LAMA), such as tiotropium bromide, theophylline or roflumilast. Triple inhaled therapy (LAMA plus LABA plus ICS) has been shown to reduce COPD exacerbations as well as hospitalizations and improve lung function, respiratory symptoms and quality of life without much safety concern [Aaron et al. 2007; Welte et al. 2009]. A randomized, controlled trial of roflumilast with the background therapy of an ICS plus LABA combination is currently ongoing [Calverley et al. 2012].
Theophylline, a nonselective phosphodiesterase inhibitor, could be compared with roflumilast. Although theophylline can be toxic and close monitoring of drug levels is necessary, it has been shown to improve respiratory symptoms, gas exchange, lung function and respiratory muscle function in patients with COPD [Murciano et al. 1989]. In a meta-analysis of 20 randomized, controlled trials, the mean improvement in FEV1 with theophylline was 100 ml compared with placebo [Ram et al. 2002], which is much greater than that of roflumilast (52 ml) noted in this meta-analysis. Although comparing the efficacy of medications across studies is hampered by biases as studies commonly use different selections criteria, the above comparison may still be valid given comparable baseline characteristics between the two meta-analyses. The mean age and baseline FEV1 ranged from 58 to 69 years and 0.96 to 1.15 liters in the theophylline meta-analysis [Ram et al. 2002], which are quite comparable to those of the current meta-analysis.
In regards to other clinical outcomes for theophylline, it did improve a quality life measure in one study [Guyatt et al. 1987], which has not been shown with roflumilast. The use of theophylline was also associated with a small reduction in COPD exacerbations in a large retrospective study [Cyr et al. 2008]. The incidence of gastrointestinal AEs was more frequent with theophylline than with placebo (RR 7.67; 95% CI 1.47–39.94) but the dropout rate did not differ between groups (RR 0.80; 95% CI 0.23–2.76; p = 0.72) in the meta-analysis [Ram et al. 2002], which suggests most of the AEs associated with theophylline might have been mild. Clinical studies directly comparing theophylline and roflumilast are warranted to determine which medication would be preferred in cases with a refractory disease.
The recommended dosage of roflumilast is 500 μg once daily and the cost of 30 days’ maintenance treatment according to the average wholesale price listings is $207 [Anonymous, 2011], which is comparable to those of maintenance inhaled therapies. It is very unlikely that roflumilast would be more cost effective than other maintenance inhaled therapies such as a LAMA or a LABA plus ICS combination because roflumilast has not been shown to reduce hospitalizations which are known to have the greatest impact on the cost effectiveness in COPD management besides the acquisition costs of medications [Hilleman et al. 2000]. Hertel and colleagues concluded that roflumilast would be cost effective in the UK [Hertel et al. 2012]. However, the cost effectiveness was probably overestimated since they did not incorporate the costs and loss of quality of life related to AEs associated with roflumilast into their study.
Our meta-analysis has limitations. First, a combination therapy of an ICS and a LABA was not allowed in any of the included trials, which is often used in patients with severe COPD with recurrent exacerbations. The risk–benefit ratio of roflumilast could change in relation to concomitant therapies. In fact, the benefit of roflumilast was limited to the subgroup of patients who were taking concomitant ICS [Rennard et al. 2011]. A further study would be needed involving the patients who are receiving LABA/ICS combination therapy.
Second, roflumilast will likely be used in patients with recurrent exacerbations despite other therapies. Such patients would likely have other cardiopulmonary abnormalities and may be on long-term oxygen therapy (LTOT). However, most of the included studies excluded patients with significant cardiopulmonary abnormalities except for COPD. In addition, patients on LTOT were excluded in half of the clinical studies, as shown in Table 1. Therefore, the results from this analysis may not be generalizable in real-world practice.
Third, rare SAEs, such as atrial fibrillation and suicidality, were significantly more common with roflumilast but such events may have happened just by accident. It is unknown if this is a chance observation or if roflumilast is arrhythmogenic or suicidogenic at this time. The risk–benefit ratio of roflumilast could change when it is widely used in a real-world practice since patients with significant cardiopulmonary abnormalities were excluded in most of the included studies (Table 1). A long-term safety profile of roflumilast needs to be established with postmarketing surveillance since such information is typically unknown for an entirely new class of medicines and their long-term side effects could be revealed only in a postmarketing study as happened with rofecoxib [Cahana and Mauron, 2006].
In summary, the efficacy of roflumilast appeared relatively modest compared with other pharmacologic therapies for COPD. AEs leading to discontinuation of therapy were not uncommon with roflumilast. SAEs were rare but the healthcare providers should be aware of the potential for suicidality and atrial fibrillation. Postmarketing safety surveillance, an efficacy trial with the background therapy of an ICS plus LABA combination, and a head-to-head trial with theophylline are warranted to further investigate the risk– benefit ratio and the place of roflumilast in the current armamentarium of COPD therapies.
Footnotes
Acknowledgements
The author would like to thank Drs Dennis Suich and John Onofrio for valuable comments on an earlier draft of this paper.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.