
Abstract
Despite the development of effective treatments, tuberculosis (TB) remains a major health problem. TB continues to infect new victims and kills nearly 2 million people annually. The problem is much greater in resource-limited countries but is present worldwide. Inadequate public health resources, cost, the obligatory long treatment period, and adverse drug effects contribute to treatment failures and relapses. Drug-resistant Mycobacterium tuberculosis (MTB) strains arise spontaneously and are propagated by inadequate treatment. According to World Health Organization global data, 17% of MTB strains in new, previously untreated cases are resistant to at least one drug. Approximately, 3.3% of new MTB cases are resistant to both isoniazid and rifampin, also called multidrug resistant (MDR), and rates of MDR-TB are greater than 60% in previously treated patients in some countries. Approximately 5% of cases of MDR-TB are also resistant to fluoroquinolones and to injectable drugs, and are called extensively drug resistant (XDR). Recently, XDR strains have been isolated that are also resistant to all standard second-line anti-TB medications. Successful drug treatment of TB with complex resistance profiles is virtually impossible with currently available drugs. There is a desperate need for new compounds that cure strains resistant to currently available drugs and for drugs that are better tolerated and will shorten treatment regimens. In the short term, new strategies for the management of drug-resistant TB with currently available drugs are being explored. These include the use of high-dose isoniazid, substitution of rifabutin in a small proportion of rifampin-resistant cases, linezolid, fluoroquinolones, and phenothiazines. A number of novel drugs are undergoing clinical testing and will hopefully be available in the near future. These include the newer oxazolidinones, diarylquinolines, nitroimidazopyrans, ethenylenediamines, pyrroles, and benzothiazinones.
Keywords
Introduction
Tuberculosis (TB) remains a leading cause of death globally. The World Health Organization (WHO) estimates that 2 billion people are infected with Mycobacterium tuberculosis (MTB) and that there are 9 million new active TB cases annually [Spigelman, 2007; World Health Organization, 2010a]. According to WHO estimates, nearly 2 million die annually with TB and a quarter of the deaths occur in individuals who are coinfected with human immunodeficiency virus (HIV) [Lawn and Zumla, 2011]. Most active cases and deaths occur in resource-limited countries where treatment and diagnostic facilities are lacking [Spigelman, 2007]. The development of drug resistance by MTB is a major concern. Drug-resistant MTB strains were first recognized soon after the introduction of streptomycin in 1944 and subsequently, resistance to other TB medications was demonstrated [Gillespie, 2002; Zhang and Yew, 2009]. Spontaneous mutations that impart drug resistance to MTB occur at predictable rates [Gillespie, 2002]. Resistant strains are perpetuated by inappropriate treatment – inadequate therapeutic regimen, poor patient compliance due to intolerable adverse drug effects, or treatment default because of inadequate support from local TB services [Chiang et al. 2010; Nuermberger et al. 2010; van der Werf et al. 2011]. Directly observed therapy short-term (DOTS) programs increase the likelihood of adherence and treatment completion and reduce the risk of the development of drug-resistant (DR)-MTB [Moonan et al. 2011]. Amongst newly diagnosed cases, approximately 17% of those previously untreated are resistant to at least one first-line drug, most commonly isoniazid (H) (10%), but resistance to any TB medication can occur and strains can become resistant to multiple drugs [World Health Organization, 2008a]. Drug resistance rates are higher in previously treated cases [World Health Organization, 2010]. Strains resistant to both H and rifampin (R), the two most effective currently available drugs, and possibly resistant to other drugs, are called multidrug resistant (MDR) [World Health Organization, 2008a]. Multidrug resistance was first reported in the early 1980s and cases are now found worldwide [World Health Organization, 2008a]. In 2009, WHO estimated that there were 440,000 new MDR-TB cases or 3.3% of new TB cases were MDR [World Health Organization, 2011b]. Annual mortality from MDR-TB was estimated to be 150,000 worldwide [World Health Organization, 2011b]. Inadequate treatment of MDR-TB leads to treatment failure, increased mortality, and the creation of MTB strains with an even more complex resistance profile. Dushanbe, the capital of Tajikistan, reported an MDR-TB rate of 16.5% in newly diagnosed patients with TB and a rate of 61.5% in previously treated cases in 2009, indicating how serious the problem of drug resistance can become [World Health Organization, 2010]. Extensively drug resistant (XDR) is the term used to describe MDR strains that are also resistant to both injectable antibiotics and to fluoroquinolones [Makarov et al. 2009]. Forty-six countries have maintained continuous surveillance of second-line drug resistance among their MDR-TB cases and 5.4% of MDR-TB strains are XDR-TB [World Health Organization, 2010]. In a recent report from Lithuania, median survival for patients with MDR- and XDR-TB was 4.1 and 2.9 years, respectively; considerably worse prognoses than for some cancers [Balabanova et al. 2011]. Even more ominous are reports of XDR-MTB strains that also demonstrate in vitro resistance to other second-line drugs, including aminoglycosides, cyclic polypeptides, fluoroquinolones, thioamides, serine analogues, and salicylic acid derivatives (Table 1) [Udwadia et al. 2012; Velayati et al. 2009]. Treatment of MDR strains requires more toxic second-line drugs and more expensive and longer treatment courses. A major limitation in choosing the best treatment strategies for MDR-TB is the dearth of controlled trials and most recommendations are based on retrospective chart reviews, case series, or expert opinion. Treatment recommendations for MDR-TB consist of an intensive 8-month phase that includes pyrazinamide (Z) and a minimum of four effective second-line drugs, including a fluoroquinolone, but not ciprofloxacin, an injectable antibiotic, one of kanamycin, amikacin, capreomycin, or viomycin, but not streptomycin which is considered a first-line drug, a thioamide, either ethionamide or prothionamide, and cycloserine or teridizone, a compound of two cycloserine molecules and terephtalaldehyde [Vora, 2010]. Treatment needs to be continued for a minimum of 20 months with four effective drugs, with the discontinuation of the injectable medication at the end of 8 months of therapy if there is a good clinical response to the intensive phase of treatment [Falzon et al. 2011]. If drug resistance or side effects preclude inclusion of one or more of these drugs, then, in descending order of preference, para-amino salicylate or group 5 antibiotics are recommended to provide a minimum of four effective drugs (see Table 1) [World Health Organization, 2008b]. The long treatment courses are expensive and difficult to tolerate. In a population of rural Bangladeshi HIV-negative patients with pulmonary MDR-TB, without extensive additional resistance and who were not previously treated with second-line drugs, a 9-month regimen that included gatifloxacin, Z, ethambutol (E), and clofazimine, and included an initial intensive 4-month phase that also included treatment with kanamycin, prothionamide, and high-dose H, resulted in a relapse-free cure rate of almost 88% with a reasonable rate of adverse effects [van Deun et al. 2010; Zhang and Yew, 2009]. Outcomes were not as good in patients treated with an ofloxacin-based regimen as in the gatifloxacin-treated group [van Deun et al. 2010; Zhang and Yew, 2009]. This study suggests that some patients with MDR-TB may be treated successfully with a shorter regimen than currently recommended by WHO [World Health Organization, 2011a].
Currently available antituberculosis drugs.

Considered a first-line drug.
Desirable attributes for a new drug
Attractive features for a new drug include a novel mode of action, good oral bioavailability, the ability to simplify or shorten treatment, a low incidence of adverse effects, activity against DR organisms, minimal interactions with TB and HIV drugs, that is, reduced interaction with hepatic CYP450 enzymes, and low cost [Koul et al. 2011; Ma et al. 2010]. Activity against both replicating and nonreplicating or dormant mycobacteria, also called latent TB infection (LTBI), would be desirable. Dormancy is defined as a state of low metabolic activity when the organisms fail to form colonies [Ma et al. 2010]. To sterilize and therefore cure TB, drugs must kill dormant MTB which otherwise can persist and begin replicating if conditions subsequently become favorable. Early bactericidal activity (EBA), the measured reduction in bacterial load within the first 2–5 days of treatment, is the usual method to assess the effectiveness of new drugs. The EBA is a good measure of the drug’s effect on active replicating MTB but does not measure its effect on the more slowly metabolizing dormant organisms and may not reflect its ability to eradicate all viable organisms. Although H has a greater EBA than R, it is not as effective against nonreplicating MTB, highlighting the importance of R in shortening treatment regimens [Ma et al. 2010; Mitchison, 2000]. TB drug development is not commercially appealing since the major burden of disease is in resource-limited countries unable to afford the high cost of new drugs [Ma et al. 2010]. TB drug discovery strategies largely rely on whole cell screening of thousands of compounds against Mycobacterium smegmatis, an organism that grows quickly and is safe for use in the laboratory [Mitchison, 2005]. This tactic has resulted in the discovery of a variety of compounds that are effective against MTB and other mycobacteria. After decades of stagnation, there is the promise of new treatment options, incorporating some of these new compounds (Table 2). No new first-line TB drugs have been approved since R was introduced in 1966 [Ma et al. 2010]. The increasing prevalence of DR-TB strains, including MDR-TB, XDR-TB, and XDR-TB strains that demonstrate resistance to second-line drugs, threatens a return to a state of affairs similar to the time before effective pharmacotherapy was available. Until new drugs are available, treatment outcomes in MDR- and XDR-TB will depend on the optimal use of existing first-, second-, and third-line options and developing new treatment strategies with existing drugs.
New drug classes.
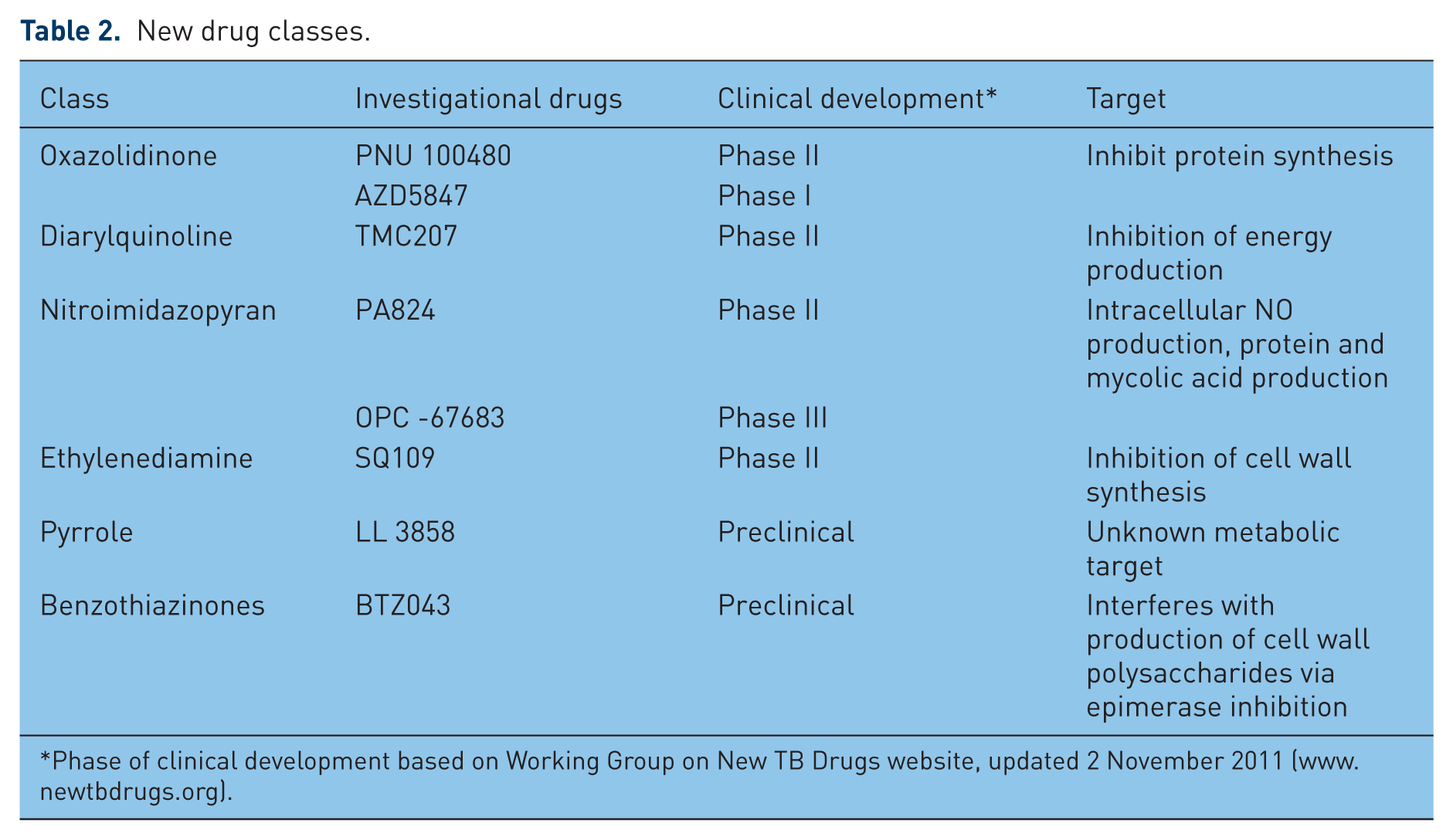
Phase of clinical development based on Working Group on New TB Drugs website, updated 2 November 2011 (www.newtbdrugs.org).
Rifamycins
The introduction of R allowed TB regimens to be reduced from 18 to 24 months to 9 months and subsequently, the addition of Z to H and R provided an effective 6-month treatment that did not promote drug resistance [Mitchison, 2005]. A 6-month treatment regimen is adequate unless the patient has cavitary disease or persistent culture positivity after 2 months of therapy [Nuermberger et al. 2010]. Rifamycins kill MTB in a concentration-dependent manner [van den Boogard, 2009]. Recommendations for R dosing have not changed since its introduction and were based on minimum inhibitory concentrations (MICs) and cost considerations [Lenaerts et al. 2005]. Subsequently, it was realized that standard dosing results in marginal R blood levels, at the low end of the concentration response curve [Jayaram et al. 2003; Mitchison and Fourie, 2010; van den Boogard, 2009]. Increasing the R dose improves its pharmacokinetic properties including peak concentration and area under the concentration–time curve (AUC) [Diacon et al. 2007]. Doubling the quotidian R dose from 600 to 1200 mg doubles its EBA and a dose of 1200 mg is generally tolerable [Diacon et al. 2007]. Increasing R dosing from 10 to 13 mg/kg increases the peak concentration by 49% and the AUC by 65% [Ruslami et al. 2006]. In a subsequent report from this group of investigators, 50 patients with newly diagnosed smear-positive pulmonary TB were randomized to treatment with either the standard or the higher R dose [Ruslami et al. 2007]. The higher dose was as well tolerated and resulted in an improved pharmacokinetic profile with higher peak drug concentrations and greater time–concentration profiles [Devasia et al. 2009]. The maximal effects of R on the hepatic cytochrome P450 oxidases (CYP450) occur at a daily dose of 300 mg, so higher than standard doses do not increase CYP450 activity further and do not have a greater effect on serum concentrations or the metabolism of other medications [Niemi et al. 2003]. R and other rifamycins inhibit bacterial DNA-dependent RNA polymerase [Uzun et al. 2002]. Approximately, 95% of the reported R resistance is due to mutation of the Rho B gene of the β subunit of RNA polymerase [Uzun et al. 2002]. Despite the presence of R resistance due to this mutation, 12–20% of R-resistant strains, including some MDR strains, remain susceptible to rifabutin [Cavusoglu et al. 2004; Uzun et al. 2002; Yoshida et al. 2010]. Rifabutin is the favored option for these MDR-TB cases [Yew and Leung, 2008]. It is also the favored rifamycin in patients with HIV taking protease inhibitors since it has the most modest effect on CYP450 enzyme induction, approximately 40% of that seen with R [Mitnick et al. 2009; Nuermberger et al. 2010]. There are other investigational rifamycins which may also be effective against R-resistant strains [Garcia et al. 2010]. Based on evidence in a murine model, daily or thrice weekly dosing of rifapentine, another rifamycin, in a regimen where H is replaced by moxifloxacin, may allow TB treatment to be shortened from 6 to 3 months [Rosenthal et al. 2007].
Fluoroquinolones
Fluoroquinolones inhibit gyrA and gyrB genes, interfering with bacterial chromosomal replication. They demonstrate concentration-dependent killing at lower MICs than other first-line drugs and they are mycobactericidal [Donald and Diacon, 2008]. They are active against both replicating extracellular and latent intracellular MTB [Cole and Riccardi, 2011]. With the exception of ciprofloxacin, they have an EBA similar to H [Garcia et al. 2010; Gillespie, 2002; Sirgel et al. 1997]. These drugs are generally well tolerated and have the convenience of once daily dosing. Fluoroquinolones have been examined both as potential first- and second-line agents for the treatment of TB [Yew and Leung, 2008]. The clinical trial results with fluoroquinolones have been variable and so far do not justify their substitution for the existing first-line drugs but they are approved as second-line agents [Burman, 2010; Moadebi et al. 2007; Takiff and Guerrero, 2011]. In areas of high TB prevalence, treating lower respiratory tract and other infections with fluoroquinolones may potentially mask and delay the diagnosis in patients with TB [Chang et al. 2010]. Fluoroquinolone resistance can develop during treatment and patients not previously treated for TB may acquire fluoroquinolone-resistant strains because of their widespread use to treat other infections [Devasia et al. 2009; Ginsburg et al. 2003; Liu et al. 2011]. Cross resistance can develop between the drugs in this class [Ginsburg et al. 2003]. Another concern is that coadministration of moxifloxacin with R reduces moxifloxacin AUC by 27% [Weiner et al. 2007]. In a murine model, moxifloxacin demonstrates more rapid EBA than H but it was similar to H in humans. In one study, the substitution of E by moxifloxacin did not increase the rate of negative sputum cultures at 2 months [Burman et al. 2006]. At standard therapeutic doses, the 8 methoxy-fluoroquinolones, moxifloxacin and gatifloxacin, have the lowest MICs among the available fluoroquinolones. Gatifloxacin use has been limited by the occurrence of dysglycemia in some patients [Yew et al. 2011]. Ofloxacin and its L isomer, levofloxacin, are also effective for TB treatment. Ciprofloxacin is not as effective as the other fluoroquinolones and should not be used to treat TB. Considering the cost and effectiveness of higher dosing, levofloxacin at a dose of 750 mg or greater is the fluoroquinolone recommended by WHO [Falzon et al. 2011]. At a daily dose of 1000 mg, levofloxacin is as effective as standard doses of moxifloxacin and gatifloxacin [Caminero et al. 2010; Johnson et al. 2006]. A retrospective review of Korean patients with MDR-TB found similar treatment success and adverse effect rates with levofloxacin and moxifloxacin [Lee et al. 2011]. Inclusion of levofloxacin in treatment regimens does not increase the rate of reported adverse effects [Marra et al. 2005]. In addition to their role in the treatment of MDR-TB, studies are underway to see if fluoroquinolones can reduce the treatment of drug-sensitive (DS)-TB from 6 to 4 or even to 3 months [Cole and Riccardi, 2011].
Oxazolidinones
Oxazolidinones are broad spectrum antibiotics that inhibit protein synthesis by interfering with messenger RNA binding to the ribosome at the initiation phase of translation [Shinabarger et al. 1997; Singh et al. 2008]. They are active against mycobacteria; both DS- and DR-TB strains, and against nontuberculous mycobacteria including the rapidly growing mycobacteria [Bressler et al. 2004; Singh et al. 2008]. Linezolid was the first drug in this class to be marketed. In pharmacokinetic studies in adults with pulmonary TB, twice daily dosing produces higher serum levels, greater AUC/MIC and increased time above MIC [McGee et al. 2009]. Its use in TB was based on early studies that demonstrated that it had modest EBA [Dietze et al. 2008]. A limiting factor is that long-term therapy at the recommended dosage of 600 mg, twice daily is associated with side effects including myelosuppression and peripheral neuropathy [Bressler et al. 2004; Green et al. 2001]. At a daily dose of 600 mg, linezolid remains active against TB and is better tolerated [Bressler et al. 2004; Nam et al. 2009; Park et al. 2006]. Although there are no available randomized clinical trials, several small series have demonstrated that regimens that integrate linezolid can successfully treat MDR-TB with manageable adverse effects [Condos et al. 2008; Koh et al. 2009; Tang et al. 2011; von der Lippe et al. 2006]. A retrospective review of the European experience with MDR- and XDR-TB found that outcomes in linezolid-treated patients were as good even though those treated with linezolid-containing regimens had more resistance to first- and second-line drugs and included more retreated patients [Koul et al. 2011]. The linezolid-treated patients, 75 with MDR-TB and 10 with XDR-TB, had a high rate of the expected side effects including anemia, thrombocytopenia, and peripheral neuropathy. The 28 patients treated with 600 mg daily had as good treatment outcomes with fewer side effects, 4 of 28 versus 31 of 57 patients, than those treated with twice daily dosing [Migliori et al. 2009]. A retrospective review of the New York City experience with MDR-TB, including XDR-TB, from 2000 to 2006 inclusively, identified 16 patients treated with a linezolid-containing regimen [Anger et al. 2010]. Side effects including myelosuppression, neurotoxicity, and gastrointestinal upset were common but were mostly manageable by temporarily stopping the medication or by reducing the dose. All of the patients were culture positive initially but converted to negative while on treatment with linezolid [Anger et al. 2010]. Eleven completed treatment with linezolid and another discontinued therapy prematurely but did not relapse [Anger et al. 2010]. Three patients died while on treatment and one relapsed 6 months after completing therapy and died 2 weeks after relapse [Anger et al. 2010]. In California, 30 patients with MDR-TB were treated with linezolid [Schecter et al. 2010]. Of these, five were still undergoing treatment when the report was prepared. Among the other 25 patients treated with linezolid, 22 were successfully treated, two defaulted, and only one failed treatment. Another oxazolidinone, PNU-100480, is currently undergoing investigation. Preliminary evidence suggests that it may be better tolerated and has greater bactericidal activity than linezolid with a MIC that is 3.2 times lower against known DR strains [Alffenaar et al. 2011]. In a murine model of TB, it was more effective than linezolid with an efficacy similar to H and R [Alffenaar et al. 2011]. It increased the bactericidal activity when added to standard therapy in a murine model, confirming its sterilizing activity [Williams et al. 2009a]. In combination with moxifloxacin and Z, it was more active than standard first-line therapy in a murine TB model, suggesting that it has the potential to reduce the required treatment period for both DS- and DR-TB [Williams et al. 2009b]. Very preliminary testing has also been started with another highly bactericidal oxazolidinone, AZD5847 [Cole and Riccardi, 2011].
High-dose isoniazid
H has been used as a first-line drug for the treatment of TB for nearly 60 years. It is a prodrug that is activated by the mycobacterial catalase-peroxidase enzyme, KatG, and acts by inhibiting cell wall synthesis by interfering with proteins involved in mycolic acid metabolism [Burman, 2010; Mitchison, 2005; Slayden and Barry, 2000]. Mutation of the katG gene, the most common cause of H resistance in MTB, conveys high-level resistance. The Inh A gene is part of the FAS-II fatty acid elongation system required for mycolic acid synthesis [Gagneux et al. 2006]. Mutations of the inh A promoter region are a less common cause of H resistance. It can be overcome with higher dosing of H, 10–15 mg/kg per day, and is important to recognize since strains with this mutation are also highly resistant to the thioamides [Caminero et al. 2010]. Increased efflux can also bestow drug resistance on MTB [Colangeli et al. 2005]. The iniA gene helps MTB eliminate both H and E from the bacterial cell [Colangeli et al. 2005].
Phenothiazines
Phenothiazines are active against MTB, both in vitro and in vivo, with an action independent of antibiotic susceptibility [Amaral and Kristiansen, 2000; Sharma and Singh, 2011]. Thioridazine has less central nervous system activity than other phenothiazines but is as active against MTB [Sharma and Singh, 2011]. Thioridazine interferes with several important metabolic pathways in MTB [Sharma and Singh, 2011]. It interferes with aerobic respiration in microaerobic conditions by inhibiting type II nicotinamide adenine dinucleotide dehydrogenase, an enzyme in the mycobacterial respiratory chain [Sharma and Singh, 2011]. It also inhibits calcium-calmodulin binding, contributing to the reversal of antibiotic resistance, making it synergistic with the antimycobacterial antibiotics [Sharma and Singh, 2011]. Thioridazine also interferes with bacterial efflux mechanisms, increasing the sensitivity of MTB to antimycobacterial agents [Amaral et al. 2008]. It is concentrated in macrophages which enhances its activity against intracellular MTB [Sharma and Singh, 2011]. It is effective against both DS- and DR-TB, and against some nontuberculous mycobacteria [Van Ingen et al. 2009]. Several small series have demonstrated that thioridazine can successfully treat patients infected with XDR-TB strains [Amaral et al. 2010]. Although less pronounced than that seen with other phenothiazines, it can cause extrapyramidal signs and QTc prolongation, potentially causing serious arrhythmias including torsade de pointe [Sharma and Singh, 2011].
Diarylquinolines
Diarylquinolines reduce adenosine triphosphate (ATP) levels by selectively inhibiting mycobacterial ATP synthase but have little effect on other bacteria and virtually none on the homologous enzyme in eukaryotes [Andries et al. 2005; Haagsma et al. 2009, 2011; Koul et al. 2007, Koul et al. 2008]. The most active diarylquinoline and the first to undergo clinical testing, TMC207, previously referred to as R207910, is active against both DS- and DR-TB, including strains that are resistant to streptomycin, Z, E, and moxifloxacin [Andries et al. 2005; Lienhardt et al. 2010; van den Boogard et al. 2009]. It has a MIC of 0.03–0.12 mg/liter against both DS- and DR-TB strains, comparing favorably to R which has a MIC of 0.15 mg/liter against DS-TB strains [Andries et al. 2005; Heifets et al. 1990; Mitchison, 2005]. It is active against MTB both in macrophages and extracellularly [Dhillon et al. 2010]. It is bactericidal against hypometabolic organisms resulting in sterilizing activity and permitting shorter and possibly once weekly treatment regimens [Ibrahim et al. 2009; Koul et al. 2007; Nuermberger and Mitchison, 2009; Rustomjee et al. 2008]. It also has good activity against the nontuberculous mycobacteria, including M. avium, M. kansasii, and rapidly growing mycobacteria, including M. abscessus [Koul et al. 2007]. TMC207 is bactericidal against both actively replicating and dormant MTB since even nonreplicating organisms require ATP synthesis to remain viable [Koul et al. 2007; Moonan et al. 2011; Rao et al. 2008]. The EBAs of three different doses of TMC207 were compared with H and R in 75 treatment-naïve patients with smear-positive pulmonary TB, including one-third who were HIV positive [Rustomjee et al. 2008]. TMC207 demonstrated good EBA at a dose of 400 mg but with a delayed onset, starting on the fourth treatment day [Rustomjee et al. 2008]. TMC207 is the first diarylquinoline to enter phase II human trials [Nuermberger et al. 2010]. The data are limited but the medication is well tolerated in humans [Andries et al. 2005]. It is administered orally and metabolized by the hepatic CYP450 enzymes, therefore coadministration with R reduces its serum concentrations [Burman, 2010; Lounis et al. 2008]. It will be most useful in regimens without R, that is, for the treatment of R-resistant strains including MDR-TB. It is as effective as the combination of first-line drugs and increases bacterial clearance when combined with them for treatment of murine TB [Burman, 2010]. It is particularly effective when used in Z-containing regimens, suggesting that synergism exists between these two drugs [Ibrahim et al. 2007; Nuermberger and Mitchison, 2009]. Even though coadministration with R reduces the AUC by one half, it still maintains significant bactericidal activity [Lounis et al. 2008]. Data from murine TB models suggest that the addition of TMC207 to MDR-TB regimens may allow the current 18–24-month regimens to be shortened to 12 months [Veziris et al. 2011]. The results of a phase IIb placebo-controlled trial of TMC207 in humans with MDR-TB have been published [Diacon et al. 2009]. Patients were treated with an appropriate regimen for MDR-TB that typically included ofloxacin, kanamycin, Z, E, and cycloserine or terizidone, and either TMC207, 400 mg daily for 2 weeks followed by 200 mg three times a week for a further 6 weeks, or placebo [Diacon et al. 2009]. Although nausea and a small degree of QT prolongation without any reported arrhythmias occurred in the TMC207-treated group, they experienced a shorter time to sputum culture conversion to negative than the group not receiving TMC207 [Diacon et al. 2009]. The conversion-to-negative rate was 48% in the TMC207-treated group compared with only 9% in the control group. Its activity is likely due to time- rather than concentration-dependent killing. Spontaneous TMC207-resistant mutations develop at similar rates to H- and R-resistant mutants [Huitric et al. 2010]. In vitro resistance develops via mutations of the atpE gene which encodes for subunit c of ATP synthase [Andries et al. 2005; Huitric et al. 2007; Petrella et al. 2006]. Other mutations can also confer resistance to TMC207 [Huitric et al. 2010].
Nitroimidazopyrans
The nitroimidazopyrans are structurally related to metronidazole. A number of compounds in this class have been studied but currently two, a nitroimidazoxazine, PA-824, and a nitroimidazoxazole, OPC-67683, are undergoing clinical development [Mukherjee and Boshoff, 2011; Papadopoulou et al. 2007]. PA-824 is a prodrug activated by mycobacterial glucose-6-phosphate dehydrogenase (G6PD). Mutations of the G6PD deazaflavin cofactor, coenzyme F420, required for activation of PA-824, impart mycobacterial resistance to the compound [Bashiri et al. 2008; Stover et al. 2000]. Microbiocidal molecules including nitric oxide and other reactive nitrogen intermediaries which damage cytochrome oxidases are produced by PA-824. It also inhibits protein and mycolic acid synthesis [Stover et al. 2000]. Mycolic acids are the very long chain fatty acids that impart a waxy-like consistency to mycobacterial cell walls. The resulting hydrophobicity interferes with drug penetration, making it difficult to kill mycobacteria and contributing to the need for protracted treatment regimens. PA-824 has a time-dependent killing profile with a satisfactory MIC, and is highly active against both DS- and DR-TB strains [Ahmad et al. 2011; Bashiri et al. 2008]. Testing against both DS- and DR-resistant strains demonstrated MICs ranging from 0.015 to 0.25 μg/ml [Stover et al. 2000]. It is effective against both actively replicating and dormant MTB [Nuermberger et al. 2006]. It has an EBA comparable to H, R, and moxifloxacin [Hu et al. 2008; Lenaerts et al. 2005; Tyagi et al. 2005]. PA-824 kills both actively replicating and nonreplicating MTB by intracellular NO release [Singh et al. 2008; Stover et al. 2000]. It is even active against dormant MTB in a hypoxic environment [Singh et al. 2008]. In a murine TB model, a combination of PA-824, Z and moxifloxacin was more effective than R, H, and Z combined [Nuermberger et al. 2008]. In another study, a combination of moxifloxacin and TMC207 was more effective than standard first-line therapy [Tasneen et al. 2011]. Studies in guinea pigs indicate that the activity of PA-824 was comparable to H [Stover et al. 2000]. In a 14-day study in man, PA-824 had a comparable EBA to the first-line drugs that was similar between doses of 200 and 1200 mg daily [Diacon et al. 2010]. It was safe, well tolerated, and demonstrated an EBA that extended over the whole study period [Diacon et al. 2010]. Despite PA-824 increasing the rates of culture conversion to negative, it did not improve relapse rates [Nuermberger et al. 2006]. It may also be effective as an aerosolized medication [Sung et al. 2009]. There were initial concerns about the effect of PA-824 on renal function in man. Although it reduces creatinine excretion in a reversible fashion, it does not reduce the glomerular filtration rate and it does not significantly affect any other aspect of renal physiology [Ginsburg et al. 2009]. Similar to PA-824, OPC-67683 is a prodrug and requires in vivo metabolic activation [Mukherjee and Boshoff, 2011]. It also contributes to the production of reactive nitrogen intermediaries and inhibits protein and mycolic acid synthesis in a similar fashion to PA-824 but unlike H, only inhibits the production of methoxy- and ketomycolates [Mukherjee and Boshoff, 2011; Yew et al. 2011]. It is active against both DS- and DR-MTB strains with MICs ranging from 0.006 to 0.024 μg/ml [Matsumoto et al. 2006]. It is more active than H or R against intracellular MTB in human macrophages [Petrella et al. 2006]. It eradicated TB more quickly than standard first-line treatment and has the potential to shorten treatment regimens [Matsumoto et al. 2006]. Drug interactions with OPC-67683 should not be problematic since it has minimal effects on the hepatic CYP450 enzyme pathways [Matsumoto et al. 2006]. Resistance to OPC-67683 is conferred by mutations to the mycobacterial Rv3547 catalytic enzyme [Mukherjee and Boshoff, 2011]. There was concern about the potential for mutagenicity with some of the earlier studied nitroimidazopyrans. However, the two currently undergoing clinical development do not interfere with nucleic acid synthesis and mutagenicity should not be a concern [Singh et al. 2008; Stover et al. 2000]. The closely related nitrofuranylamides (NFAs), which are structurally similar to nitrofurantoin, also demonstrate activity against MTB, including DR strains, but do not have clinically significant activity against the nontuberculous mycobacterial species [Hurdle et al. 2008]. Resistant mutants can develop to NFA compounds and are cross resistant to the nitroimidazopyrans [Hurdle et al. 2008].
Ethylenediamines
The ethylenediamines are derivatives of E that are being investigated for their potential as antimycobacterial medications [Vergara et al. 2009]. One member of this class, SQ-109, is active against E-resistant MTB strains [Burman, 2010]. It demonstrated MICs ranging from 0.7 to 1.6 µM against DS- and DR-MTB strains [Protopopova et al. 2005]. It is active both in an in vitro model of murine macrophages and in vivo against murine TB [Jia et al. 2005]. Although less potent than H administered at a dose of 25mg/kg per day, its antimycobacterial activity was similar to E 100 mg/kg per day, and tissue drug levels were 10-fold greater than the MIC [Jia et al. 2005]. Its mechanism of action has not been discovered but it appears to interfere with cell wall synthesis and it has activity against both DS- and DR-TB, including MDR-MTB strains [Global Alliance for TB Drug Development, 2008; Nikonenko et al. 2007]. It has good activity against MTB with a MIC of 0.5 μg/ml and it has a synergistic effect with H, R, and with TMC207 [Chen et al. 2006; Reddy et al. 2010]. The synergistic effect with R was also present against R-resistant strains and the combination resulted in a reduction in the MIC of R in these strains [Chen et al. 2006]. It appears to act in an additive fashion with streptomycin but did not appear to have either an additive or synergistic effect when combined with Z or E [Chen et al. 2006]. Replacing E with SQ-109 improved the effectiveness of the standard first-line regimen, H and R, with and without Z, in a murine model of TB [Nikonenko et al. 2007]. Other diamines with antimycobacterial properties are also undergoing preliminary testing [Onajole et al. 2010, 2011].
Pyrroles
A pyrrole, LL3858, has antimycobacterial activity but its metabolic target is unknown. It has potent antimycobacterial activity with a MIC range of 0.06–0.5 μg/ml against DS- and DR-TB strains [Nuermberger et al. 2010; Shi and Sugawara, 2010; Yew et al. 2011]. It was active against MTB by itself and enhanced the effects of standard therapy with H, R, and Z [Shi and Sugawara, 2010].
Benzothiaziniones
Benzothiaziniones target the heterodimeric enzyme, decaprenylphosphoryl-β-D-ribose 2’-epimerase, essential in the production of arabinans [Makarov et al. 2009]. These mycobacterial cell wall polysaccharides are necessary to maintain cell wall integrity and their disruption results in cell lysis and bacterial death [Cole and Riccardi, 2011; Makarov et al. 2009]. A benzothiazinione, BTZ043, has MICs comparable to H, both in vitro and in murine models. It does not appear to be mutagenic [Makarov et al. 2009]. It was effective when tested against 240 DS- and MDR-TB strains isolated from cases in European hospitals [Cole and Riccardi, 2011; Makarov et al. 2009].
Summary
Although no new first line-drugs are commercially available yet, there are exciting new candidate compounds in several different drug classes. They hold the promise of shorter treatment regimens and offer the promise of cure for patients with MTB strains resistant to the currently available first-line drugs. A diarylquinoline, TMC207, will likely be the first of the new candidate medications to reach the market.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.