
Abstract
Objectives:
Screening for sleep disordered breathing (SDB) remains poor in the general population, despite evidence for association with adverse outcomes and improvement of certain outcomes with therapy. Data from the past decade have suggested an association between snoring and adverse pregnancy outcomes including gestational hypertensive disorders. However, it is unclear how often SDB is screened for in pregnancy. The objective of this study was to evaluate whether, and how, symptoms of SDB are assessed during prenatal care.
Methods:
This study was designed as a survey-based observational study. Within 48 hours of delivery, English-speaking patients were surveyed regarding prenatal conversations with obstetric providers about symptoms of SDB. During a similar time period, obstetric providers completed an anonymous questionnaire regarding how often they discussed the same symptoms during prenatal visits.
Results:
A total of 776 patients and 80 providers performing the majority of deliveries at the same hospital answered the survey. Nurse providers asked about sleep quality significantly more often than physician providers; however, responses to questions about snoring were similar in both groups. Resident physicians were the least likely to ask about sleep quality. Less than 3% of providers reported asking about snoring, closely matching patient responses. A total of 44% of patients surveyed were overweight and 21.7% were obese. Although 32% of patients snored, only 5% were asked about snoring during a prenatal visit. Obese women and women with a history of gestational hypertensive disorders were more likely to report being asked about snoring.
Conclusions:
Based on patient and obstetric provider recollections of discussions, the issue of SDB is poorly assessed during routine prenatal care, despite an increasing prevalence of overweight and obesity in the pregnant population.
Introduction
Sleep related breathing disorders include many syndromes such as obstructive sleep apnea (OSA), central sleep apnea and obesity hypoventilation. Loud snoring is the most common complaint in patients with OSA but may also indicate milder forms of sleep disordered breathing (SDB). Women are less likely to report snoring than men and may have an atypical presentation with presenting symptoms of insomnia, anxiety and depression. Despite an association with adverse cardiovascular outcomes such as hypertension, type II diabetes, cardiovascular and cerebrovascular disease, SDB remains an underdiagnosed disorder in the general population [Foster et al. 2009; O’Connor et al. 2009; Peppard et al. 2000; Punjabi, 2008].
Pregnancy is a unique period associated with physiologic changes that may predispose women to the development of SDB regardless of other comorbidities [Bourjeily, 2009]. Nasal congestion, a phenomenon that has been described in up to 30% of pregnant women, is a known risk factor for SDB. A smaller upper airway size has been described in pregnant women [Izci et al. 2003, 2006]. Diaphragmatic elevation with up to a 20% reduction in functional residual capacity (FRC) occurs in pregnancy with an additional drop in the supine position near term. Reduction in FRC has been known to predispose to airway collapsibility during sleep [White, 2005].
The prevalence of snoring is significantly increased among pregnant women, ranging from 10–45% [Bourjeily et al. 2010; Calaora-Tournadre et al. 2006; Franklin et al. 2000], and occurs more commonly than among nonpregnant women controls [Higgins et al. 2011]. Importantly, snoring, used as a surrogate for SDB in many studies, has been associated with adverse pregnancy outcomes including gestational hypertensive disorders: preeclampsia and gestational hypertension [Bourjeily et al. 2010; Franklin et al. 2000; Perez-Chada et al. 2007; Ursavas et al. 2008], as well as gestational diabetes [Bourjeily et al. 2010; Facco et al. 2010; Qiu et al. 2010]. Data on the association of SDB with adverse neonatal outcomes are less consistent [Bourjeily et al. 2010, 2011; Calaora-Tournadre et al. 2006; Franklin et al. 2000; Olivarez et al. 2010].
Providers from medical disciplines continue to poorly screen for SDB despite the fact that treatment of this disorder with continuous positive airway pressure (CPAP) improves daytime somnolence, quality of life [D’Ambrosio et al. 1999; Giles et al. 2006], and cardiovascular outcomes [Marin et al. 2005; Shah et al. 2010] and lessens healthcare costs [Bahammam et al. 1999; Kapur and Alfonso-Cristancho, 2009]. Given the available data on the high prevalence of snoring in pregnancy and its association with adverse outcomes, it is not clear how SDB is screened for in this population.
We hypothesized that SDB is rarely screened for in pregnancy. Our objective was to evaluate how often the topic of SDB was discussed during the prenatal period. This was accomplished by assessing: (1) patient recollection of discussing sleep with their obstetric provider and (2) obstetric providers’ perceptions of their frequency of addressing SDB with patients.
Methods
Patients
English-speaking women 18 years or older who delivered at a large tertiary care women’s hospital between December 2006 and June of 2008 were eligible to be surveyed within 48 hours of delivery. The study was approved by the institutional review board. Patients were selected systematically from a daily list of deliveries. Women were asked whether they would participate; those who agreed signed a written informed consent and answered a questionnaire. Women were asked questions regarding conversations with their obstetric provider during the course of their prenatal care. The conversations presented included questions regarding symptoms of SDB, daytime hypersomnolence and referral for a sleep evaluation (Figure 1). Conversations about more common clinical questions asked during prenatal visits, such as fetal movement, were also included to act as ‘control’ questions. The patient could respond ‘yes’, ‘no’ or ‘unsure’.

Questions to patients about prenatal assessment of sleep disordered breathing.
In addition, women were asked about frequency of snoring, gasping, and apneas in the last 3 months of pregnancy.
Demographic information was also collected and included weight and height at the first prenatal visit. Data on medical history including current or prior history of gestational hypertensive disorders (preeclampsia or gestational hypertension) were also collected by survey and review of patients’ medical records.
Providers
All obstetric providers in the state were surveyed by mail with a similar questionnaire during the same time period, but only data from those who considered the tertiary care hospital as their primary hospital were analyzed. The survey included the same questions regarding SDB and the same ‘control’ questions; questions to providers are detailed in Figure 2. Responses to the questionnaire were anonymous but the survey asked for the provider’s title, physician provider (attending or resident) or nurse provider (certified nurse-midwife or registered nurse practitioner). A second request was sent by mail 2 months after the initial survey and providers were asked to fill out the questionnaire only once.
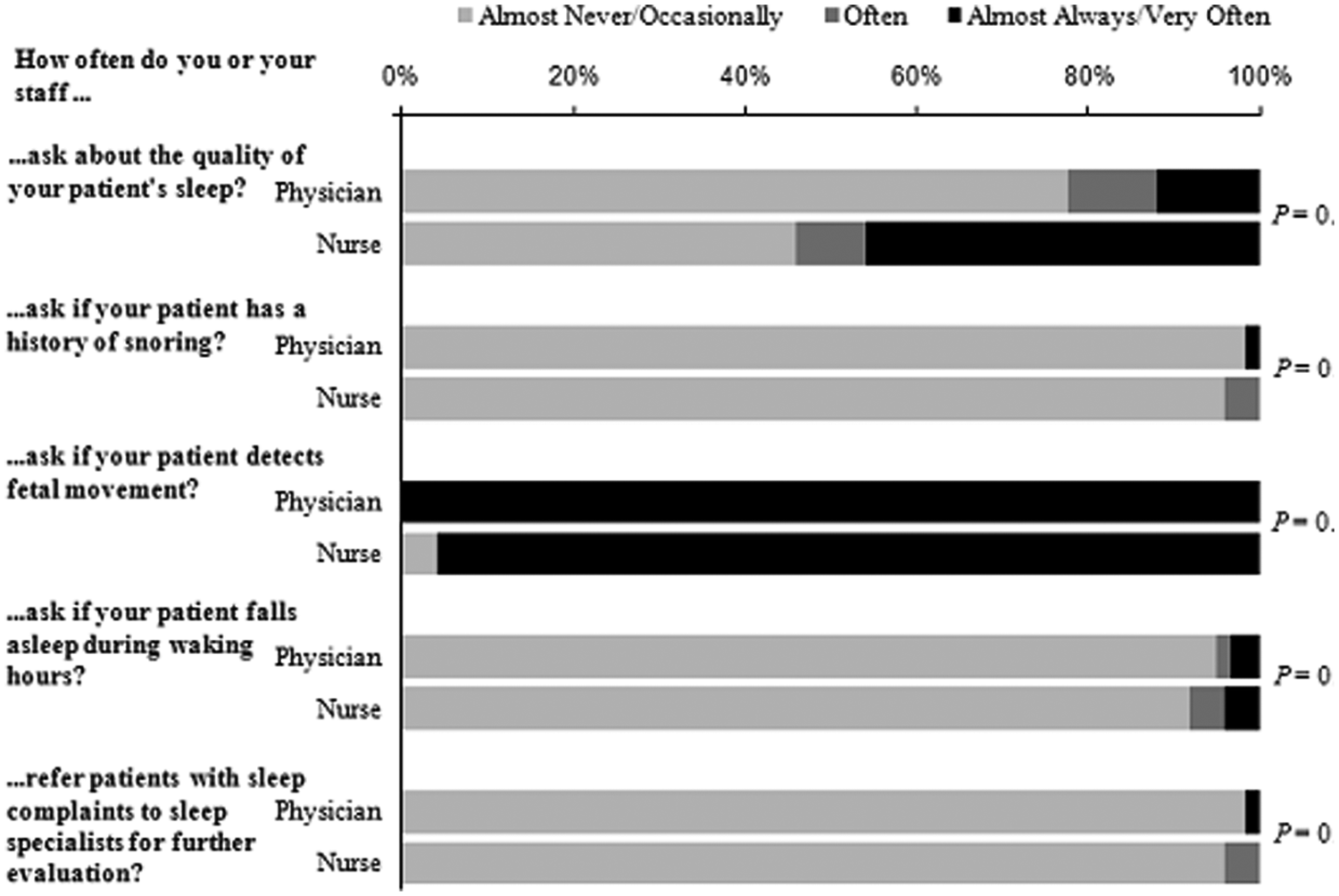
Provider questions to patients about sleep disordered breathing during pregnancy, by job title.
An example of a question asked was ‘In your pregnant population, how often do you or your staff ask a patient about snoring?’. Providers had the choice of the following answers: ‘never’, ‘rarely’, ‘often’, ‘very often’, or ‘almost always’.
Statistical analysis
All statistical analyses were conducted with the use of SAS software version 9.2 (SAS Institute, Cary, NC). Categorical variables were compared by chi-squared or Fisher’s exact test. Provider survey responses were categorized as never/rarely, often, very often/almost always. Unsure or missing responses were excluded from the analysis. Odds ratios (ORs) and 95% confidence intervals (CIs) for patient characteristics and provider questions (asked/not asked) were calculated by multivariate logistic regression. Patient age was categorized into quartiles for analysis. All p-values are two-tailed, with p < 0.05 considered statistically significant.
Results
Patient characteristics
A total of 776 women answered the survey (97% response rate). Their mean age was 29.1 years (range: 18–50); 25% of women met criteria for advanced maternal age. The majority of women were white (71.4%), 13.3% were Hispanic, 9.2% were Black, 3.4% were Asian and 2.7% were classified as ‘other’. A total of 44% of patients were overweight (body mass index [BMI] ≥25) and 21% were obese (BMI > 30), based on a prepregnancy BMI. Mean BMI at the time of delivery was 32 ± 6.2 (Table 1). A total of 2% of responders had a history of chronic hypertension, 12.1% had preeclampsia or gestational hypertension (current or prior history) and 16.1 % had a history of depression. SDB symptoms reported more than three times a week included: loud snoring in 32% of women, gasping in 10.1% and witnessed apneas in 4.4%.
Patient characteristics (n=776)

Patient responses
When asked whether a healthcare provider had addressed the patient during the course of the pregnancy about the quality of their sleep, 41.1 % of women answered ‘yes’ (Figure 1). A total of 5% of women were asked about snoring, 3.8% asked about gasping and 15.2 % asked about daytime hypersomnolence. Fourteen patients (1.8%) were referred for a sleep evaluation. Among women who were referred for further sleep evaluation, the majority (53.9%) were referred by an internist and four (28.5%) were referred by their obstetric provider.
Provider responses
A total of 250 provider questionnaires were mailed out with a total of 102 responses (40.8%). All respondents answered all of the questions on the survey. The majority of providers (80.4%) considered the tertiary care institution their primary hospital and only these providers were included in the analysis. The characteristics and responses were similar for the included and excluded groups.
A total of 22.7% of providers answered that they ‘very often or always’ ask their patients about their sleep quality. However, 97.6% answered ‘almost never or occasionally’ to the questions on snoring, gasping and choking. A total of 93.9% answered ‘almost never or occasionally’ to the question asking about daytime hypersomnolence (Figure 2). When asked how often providers refer their patients to a sleep specialist for an evaluation of sleep complaints, 97.6% responded ‘almost never or occasionally’. When asked how often providers asked about fetal movement, 98.8% answered ‘almost always, very often’.
Providers were analyzed by their type of training, i.e. physician providers (including residents and attending physicians; 69.6%) versus nurse providers (which includes nurse–midwives and nurse practitioners; 30.4%). Nurse providers asked significantly more frequently about sleep quality than their physician counterparts (45.8% versus 12.1% respectively, p = 0.004). However, there were no significant differences in the responses to the questions regarding snoring (p = 0.5), gasping (p = 0.5), daytime hypersomnolence (p = 0.8), or referral to a sleep specialist (p = 0.5) among the nurse provider and the physician provider group.
When physician providers were analyzed by experience (resident physician versus attending physician), attending physicians were more likely to ask about sleep quality than resident physicians (16.6% versus 4.5%, p = 0.04). However, there were no significant differences in the responses to the questions regarding snoring (p = 0.4), gasping (p = 1.0), daytime hypersomnolence (p = 0.7), or referral to a sleep specialist (p = 1.0) among the two groups.
Regression analysis
Age did not appear to affect how often women were asked about snoring (Table 2). Interestingly, older women reported being asked less often about daytime hypersomnolence than their younger counterparts (p = 0.0009), even when adjusted to other variables (p = 0.0003) (Table 2). Obese women were more likely to be asked about snoring; and overweight (but not obese) women were more likely to be asked about daytime hypersomnolence than their normal weight counterparts.
Multivariable logistic regression analysis of patient characteristics and provider questions about snoring and excessive daytime sleepiness.
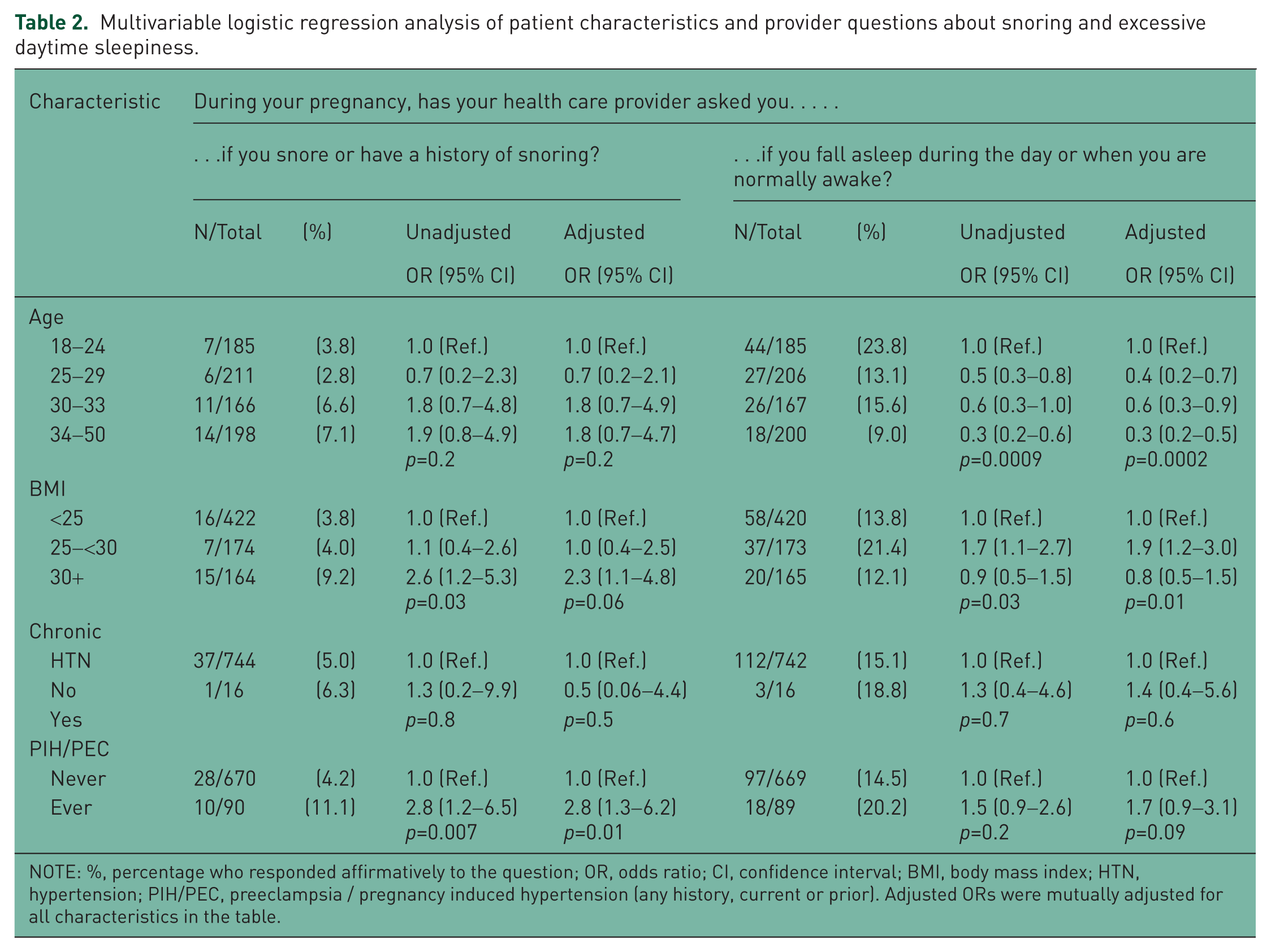
NOTE: %, percentage who responded affirmatively to the question; OR, odds ratio; CI, confidence interval; BMI, body mass index; HTN, hypertension; PIH/PEC, preeclampsia / pregnancy induced hypertension (any history, current or prior). Adjusted ORs were mutually adjusted for all characteristics in the table.
Patients with a history of chronic hypertension were not more likely to be asked about snoring, daytime hypersomnolence, or other symptoms of SDB. However, patients with a current history of gestational hypertensive disorder and those with any history (current or prior) of hypertension were more likely to be asked about snoring, even after adjusting for other variables (adjusted odds ratio [aOR] 2.7, 95% confidence interval [CI] 1.1–6.3, p = 0.02 and aOR 2.8, 95% CI 1.3–6.2, p = 0.01, respectively ), but not about daytime hypersomnolence. A prior history of depression was associated with a trend toward prompting providers to ask about quality of sleep (p = 0.07) but did not reach statistical significance in either the univariate or the multivariate regression analyses.
In addition, women were more likely to be referred to a sleep specialist if they had a BMI ≥30.0 (4.8% versus 1.0% for <25.0; p = 0.006) or a history of chronic hypertension (12.5% versus 1.5%; p = 0.03), but not if they currently snored (p = 0.5) or were older (p = 0.2).
Discussion
This study consists of a survey administered to providers, and to women in the immediate postpartum period regarding assessment of SDB symptoms during routine prenatal care. Both patient and provider surveys showed that assessment of SDB symptoms is rarely sought during the course of pregnancy. Nurse providers were more likely to ask about sleep quality than physician providers but the frequency of inquiring about SDB symptoms was similar among the two groups. Only 5% of women were asked about snoring despite a prevalence of 32% in this population. Only 1.8% of patients were referred for a sleep evaluation, and in the majority of cases, the referral was performed by internists. Obese women and women with a prior history of gestational hypertensive disorders were more likely to be asked about snoring but not about daytime hypersomnolence.
SDB is common in the nonpregnant population but may still be underdiagnosed. The incidence of the disorder in the general population depends on how the disease is defined. The incidence of OSA may vary from 2–9% when OSA is defined as AHI >5 with at least one symptom that is known to improve with therapy [Epstein et al. 2009; Jennum and Riha, 2009] to 20% when OSA is defined as an AHI >5 [Punjabi, 2008]. The incidence of OSA in pregnancy is not known, but the disorder is less likely to be suspected in young women, such as pregnant women. Our study has shown that patients were not appropriately asked about symptoms of OSA, despite the high prevalence of symptoms and risk factors and were only rarely (1.8%) referred for a sleep evaluation. These data suggest that the diagnosis of OSA is very likely to be missed during pregnancy since obstetric providers, who are the main providers for the duration of pregnancy in most cases, are rarely asking questions relating to the disorder, even in women at risk. Interestingly, providers asked about quality of sleep much more commonly (22.7%) than snoring. This may be due to either an attempt at educating patients about expected sleep disturbances due to pregnancy physiology or to the fact that providers may not have the appropriate training to discuss or potentially manage sleep-related disorders such as SDB. Despite the strong association between OSA and chronic hypertension, a history of chronic hypertension did not prompt providers to ask about symptoms of SDB more frequently [O’Connor et al. 2009; Peppard et al. 2000]. Although providers were more likely to ask about snoring and refer for a sleep evaluation in obese women, the referral still occurred very infrequently. A referral rate of 1.8% seems quite low given the high prevalence of obesity (22%) and snoring (32%) in our sample. Given the relatively short duration of pregnancy, timely diagnoses and interventions are needed. It is possible that delays in obtaining polysomnography and initiating interventions in this population may play a role in referral rates during pregnancy. Given the large number of women who become pregnant every year and the epidemic of obesity in many parts of the world, in-home testing may have to replace polysomnography in this population.
Recent data regarding screening for OSA in the nonpregnant population shows that primary care providers including family practitioners continue to poorly screen for OSA. In one study by Grover and colleagues, physicians documented only 24% of all sleep complaints experienced by 382 patients [Grover et al. 2011]. Another study that collected data from 44 randomly selected practices showed that very few primary care clinicians routinely screen for OSA [Mold et al. 2011]. Despite >90% of selected patients having sleep-related symptoms, less than a third had these symptoms documented in their medical records [Mold et al. 2011]. In a study published a decade ago, cardiologists underreported OSA compared with primary care providers [Namen et al. 2002]. Based on the current study and the available data, primary providers including obstetricians as well as specialists do not seem to screen appropriately for the disorder. Lack of questioning about symptoms of SDB in pregnancy may be related to causes similar to those identified among medical disciplines such as lack of confidence in identifying and managing the disease [Southwell et al. 2008]. The lack of screening among obstetric providers may also be related to the lack of conviction that such screening is necessary given that there are no available data showing that therapeutic interventions actually improve pregnancy outcomes. The authors would argue that making the diagnosis is important at any time because treatment with CPAP is associated with improved excessive daytime sleepiness and quality of life [D’Ambrosio et al. 1999; Giles et al. 2006], with data suggesting improved cardiovascular outcomes and blood pressure measurements [Marin et al. 2005; Shah et al. 2010] and these findings are likely as true for the pregnant population as they are outside of pregnancy. In addition, with frequent visits to a healthcare provider and the motivation to do ‘the right thing’ given concerns for the unborn child, pregnancy has the prospect of being a period where lifelong interventions may be more successfully instituted.
Nurse providers asked about sleep quality more commonly than physician providers. This may be due to the fact that nurse providers are usually allotted more time with patients than physician providers are but may also have to do with the training curriculum of nurse providers compared with that of physicians. In addition, resident physicians were the least likely to ask about sleep quality, raising the question of whether sleep education should be included in obstetric residency curricula, given the accumulating literature about sleep and SDB outcomes in pregnancy.
Snoring in pregnancy has been associated with key adverse pregnancy outcomes such as gestational hypertensive disorders [Bourjeily et al. 2010; Calaora-Tournadre et al. 2006; Franklin et al. 2000; Perez-Chada et al. 2007; Ursavas et al. 2008] (OR 1.8–2.3 in most studies) [Bourjeily et al. 2011] and gestational diabetes (aOR 2.1, 95% CI 1.3–3.4) [Bourjeily et al. 2011; Facco et al. 2010]. In addition, higher rates of unplanned Caesarean deliveries were found to be associated with both loud snoring [Bourjeily et al. 2011] and OSA [Louis et al. 2010]. Associations of snoring with critical fetal outcomes have also been shown including growth restriction in some studies [Franklin et al. 2000; Micheli et al. 2011 ] but not others [Bourjeily et al. 2010; Loube et al. 1996; Tauman et al. 2011b]; preterm birth [Bourjeily et al. 2010] and induced preterm birth [Louis et al. 2010] were found in snorers and patients with OSA, respectively. This outcome may have been mediated by preeclampsia. Fetal decelerations occurring at the time of apneic events have been studied. However, although fetal decelerations in response to apneic events have been suggested by small case series [Sahin et al. 2008] and case reports [Joel-Cohen and Schoenfeld, 1978], these studies lacked synchronization between fetal monitors and apnea monitors, did not adjust for confounders, or were based on clinical observations rather than polysomnographic documentation of apneas. A recent study evaluating in-hospital patients in the second half of their pregnancy showed a surprisingly high incidence of OSA but the selected apneic events shown did not show any significant effects of apneic events on fetal heart rate [Olivarez et al. 2010]. A recent report has shown preliminary evidence of elevated nucleated red blood cells, erythropoietin and interleukin-6 in newborns of snorers compared with newborns of nonsnorers, suggesting subtle alterations in markers of fetal wellbeing in pregnant snorers [Tauman et al. 2011a].
Although glucose abnormalities and fetal outcomes were collected on the surveyed patients in this study, those outcomes were not included in the multiregression analysis as these data are much more recent and were not published at the time of the provider survey. However, it is reassuring to know that providers are more likely to ask about snoring in patients with a history of ever having been diagnosed with a gestational hypertensive disorder.
The most important strength of the study is the number of women who were surveyed. In addition, although the response rate of obstetric providers was only 41%, the number of physicians reporting their practice styles is still large and practice styles similar. Supporting our hypothesis that SDB is rarely screened for in pregnancy, providers and patients alike reported a low rate of discussing sleep during the course of prenatal care.
However, there are several limitations to our study. The women completing the survey were from a primarily urban/suburban population and were cared for at a tertiary academic institution and may not represent the general pregnant population. The number of obstetric providers who responded to the survey was approximately 41% and may not truly represent the behaviors of all providers in the community. Our study is also limited by a potential for recall bias since women were interviewed at the end of their pregnancy.
In summary, despite an association of SDB symptoms with adverse pregnancy outcomes, obstetric providers do not screen appropriately for the disorder and, therefore, only rarely refer women for further evaluation.
Footnotes
Acknowledgements
We are grateful to Susan M. Martin, Cynthia Citino, and Kevin Connors for their help with patient recruitment and data collection, and Beth Hott and Lorraine Manchester for their help with manuscript preparation. These individuals were compensated for their contribution to the work. We are also grateful to the Perkins Charitable Foundation for their generous funding and support of the study, and George Oliva III and Charles McPhee for their help with obtaining funding.
Funding
This work was supported by the Perkins Charitable Foundation. The foundation did not have a role in the design, data analysis or manuscript preparation.
Conflict of interest statement
The authors declare that there are no conflicts of interest to declare.