
Abstract
To develop an efficient therapy for chronic obstructive pulmonary disease (COPD), N-acetylcysteine (NAC) has been tested as a medication that can suppress various pathogenic processes in this disease. NAC is a thiol compound, which provides sulfhydryl groups. NAC can act as a precursor of reduced glutathione and as a direct reactive oxygen species scavenger, hence regulating the redox status in the cells. In this way NAC can interfere with several signaling pathways that play a role in regulating apoptosis, angiogenesis, cell growth and inflammatory response. Mucus hypersecretion has been reported in COPD and in other respiratory conditions. Two pathological processes have been described to play an important role in COPD, namely oxidative stress and inflammation. Both of these processes can induce mucin gene expression leading to mucin production. NAC, therefore, may influence mucin expression by acting on oxidative stress and inflammation, and play a role as a mucolytic agent. In this review we focus on the mucolysis of NAC in the management of COPD.
Sputum production in chronic obstructive pulmonary disease
Patients with chronic obstructive pulmonary disease (COPD) exhibit airway mucus hypersecretion, including sputum production, increased luminal mucus, goblet cell hyperplasia and submucosal gland hypertrophy [Rogers, 2001]. These processes have been shown to contribute significantly to morbidity and mortality in patients with COPD, especially in older patients and those who are prone to respiratory tract infection [Vestbo, 2002; Prescott et al. 1996; Rogers, 2001]. The effects of mucus hypersecretion in COPD are summarized in Figure 1.

Effects of mucus hypersecretion in chronic obstructive pulmonary disease. FEV1, forced expiratory volume in 1 s.
Cigarette smoke is a potent airway irritant and the strongest risk factor for COPD. Smokers with chronic bronchitis have an increased number of goblet cells compared with nonsmokers [Saetta et al. 2000] and an increased number of goblet cells correlates with epithelial mucin stores [Innes et al. 2006]. The mechanisms by which cigarette smoke exposure induces inflammation are not fully understood. However, an early alteration in the epithelial barrier function has been reported. Moreover, it has been described that cigarette smoke triggers oxidative stress-dependent processes such as neutral spinogomyelinase-mediated ceramide upregulation, p38 mitogen activated protein kinase (MAPK) and c-Jun N-terminal kinase (JNK) activation [Schweitzer et al. 2011].
The mucus hypersecretion can be initiated by an acute event that results in epithelial injury, neutrophil activation and release of chemokines. In case of prolonged/chronic exposure to toxic agent/irritant there is continuous neutrophil activation and permanent release of the inflammatory cytokines and proteases leading to permanent mucus hypersecretion [Erjefalt et al. 1995; Dignass and Podolsky, 1993]. Several mediators have been shown to stimulate mucus secretion (i.e. oxidants, cytokines, neuropeptides, adenosine triphosphate and uridine triphosphate, bacterial products, neutrophil elastase and inhaled pollutants) [Martin et al. 1997].
It is important to mention that there are two structurally and functionally distinct classes of mucins: membrane-bound and secreted mucins. Membrane-bound mucins participate in functions such as cellular adhesion, pathogen binding and signal transduction. The most studied secreted mucins that are responsible for the biophysical properties of the mucus are the gel-forming mucins: MUC5B (constitutively expressed) and MUC5AC (inducible) [Perez-Vilar et al. 2006]. MUC5AC transcription is mediated through c-Src and MAPK [Gray et al. 2004] and it is also activated by protein kinase C mediated events and the janus kinase-signal transducer and activator of transcription (JAK-STAT) signaling pathway [Fischer et al. 1999; Longphre et al. 1999; Basbaum et al. 1999].
The inflammatory process in COPD involves neutrophils, cytotoxic CD8+ cells and macrophages [Jeffery, 2004] but the key inflammatory cell in COPD is the neutrophil. The neutrophil releases a variety of enzymes and one of its most important products is neutrophil elastase. Its secretion is carefully regulated under normal conditions [Nadel, 2000]. The local release of neutrophil elastase requires close contact between the neutrophil and another cell, mediated by surface adhesion molecules, thus limiting proteolysis to the immediate pericellular environment [Pettersen and Adler, 2002]. In the airway lumen, neutrophils undergo apoptosis and are cleared by macrophages without releasing their intracellular contents. In contrast, neutrophils that die by necrosis release proteases and reactive oxygen species (ROS) into the lumen. Release of inflammatory mediators, such as neutrophil elastase, triggers mucus hypersecretion via activation of various signaling pathways [Rogers, 2007].
Neutrophils that are recruited to the airways (and their secreted products) have been reported to play several key roles in epidermal growth factor receptor (EGFR)-dependent mucus hypersecretion [Shao and Nadel, 2005]. The possible pathways are presented in Figure 2. Namely, by releasing neutrophil elastase and tumor necrosis factor α, neutrophils influence EGFR expression in airway epithelium, increasing the mucin production. Moreover, neutrophil elastase causes goblet cell degranulation and this can affect mucus production. Another possible pathway is through ROS which, in turn, influence EGFR expression [Kim and Nadel, 2004].
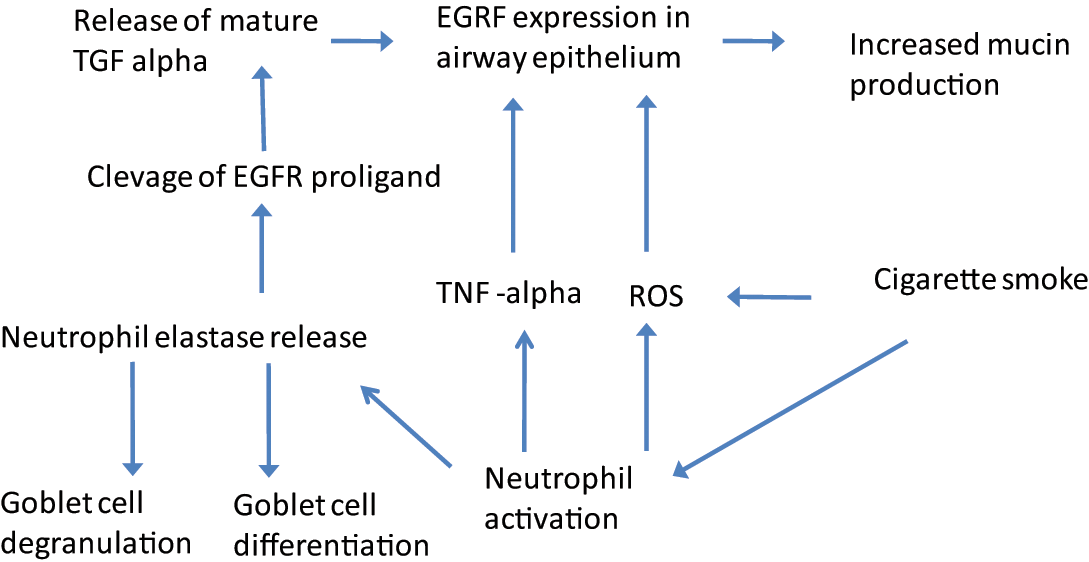
Epidermal growth factor receptor (EGFR) activation pathways (for references see text). ROS, reactive oxygen species; TNF, tumor necrosis factor.
Recently, a potential role of nuclear factor κB (NFκB) factor on mucin expression has been reported, namely, rhinovirus induction of MUC5AC in bronchial epithelial cells in vitro occurred via NFκB-dependent induction of matrix-metalloproteinase-mediated transforming growth factor α release, thereby activating an EGFR-dependent cascade [Hewson et al. 2010]. This finding is supported by another study using a flavonoid, naringenin, to inhibit the activation of EGFR. Naringenin also reduced the protein expressions of phosphorylated EGFR, phosphoinositide 3 kinase (PI3K), phosphorylated Akt, phosphorylated extracellular-signal-regulated kinase 1/2 (ERK1/2) and NFκB and significantly inhibited PI3K/Akt and ERK MAPK signaling with a concurrent reduction in production of ROS and NFκB activities. This suggests that naringenin may play a protective role by minimizing mucus production during airway inflammation by downregulating ROS production and inhibiting NFκB activity via the EGFR-PI3K-Akt/ERK MAPK signaling pathway [Yang et al. 2011].
In addition, mucus hypersecretion and gel thickness can be stimulated by macrophage derived and epithelium derived inflammatory mediators such as interleukin 4 (IL-4), IL-5, IL-9, prostaglandin E2, tumor necrosis factor α (TNFα) [Enss et al. 1997; Adler et al. 1994; Temann et al. 1997, 1998].
Therefore, several therapeutic targets for neutrophil-dependent mucus hypersecretion could be studied; that is, the inhibition of inflammatory cells, their degranulation and release of ROS, and inhibition of signaling pathways (e.g. EGFR, NFκB).
Consequently, future research should determine whether there really is an intrinsic abnormality specific to mucus in COPD. Based on this information, appropriate suppressors of mucus hypersecretion in COPD can be developed.
Role of medication in sputum expectoration
A few mucoactive medications are currently available, which may be beneficial in hypersecretory disorders of the airways.
Mucoactive agents are meant to either increase the ability to expectorate sputum (expectorants, mucolytics and mucokinetic drugs) or decrease sputum hypersecretion (mucoregulators).
Expectorants are meant to increase the volume of airway water or secretion to increase the effectiveness of coughing. They decrease the adhesion of secretions and they are meant to improve airway clearance. Importantly, they do not alter the ciliary beat frequency or mucociliary clearance. Although expectorants are sold over the counter, there is no evidence that they are effective for the therapy of any form of lung disease, and when administered in combination with a cough suppressant such as dextromethorphan there is a potential risk of increased airway obstruction.
Mucolytics [e.g. N-acetylcysteine (NAC)] depolymerize mucin. The classic mucolytics have free thiol groups to degrade mucin. It is possible due to free thiol groups, which dehydrolize disulfide bonds. NAC is able to decrease the mucus viscosity in vitro [Sheffner, 1963] but because of the rapid inactivation seems not to have this effect in vivo. Properties of NAC are described in more detail below.
DNA-active medications such as dornase α (Pulmozyme: Genetech Inc, San Francisco, CA, USA) and potentially actin-depolymerizing drugs such as thymosin-4 may be of value in helping to break down airway mucus.
Mucokinetic agents can increase the effectiveness of cough, either by increasing expiratory cough airflow or by increasing mucociliary efficiency. In this group we can find β-agonist bronchodilatators and methylxanthines.
Mucoregulatory agents reduce the volume of airway mucus secretion. Mucoregulatory agents include anti-inflammatory agents, anticholinergic agents, some macrolide antibiotics and presumably also NAC, which can act as an anti-inflammatory agent and antioxidant.
Novel compounds are undergoing preclinical research, for example, inhibitors of EGFR tyrosine kinase and antisense oligomers [Rubin, 2007].
N-Acetylcysteine: pharmacokinetics and mechanisms of action
NAC is a thiol and mucolytic agent, a precursor of L-cysteine and reduced glutathione. The mucolytic properties of NAC are the most common reason for its use. Although NAC has been used for many years to treat a number of respiratory conditions [Ziment, 1986], its efficacy is not very well documented despite being thoughtfully studied in vivo and in vitro. The possible lack of efficacy of NAC can be explained by its pharmacokinetics, which are highly dependent on the administration route.
NAC is rapidly absorbed following an oral dose. Plasma concentrations after an oral administration of 600 mg peak after 60 min (4.6 μM), quickly decreasing to 2.5 μM after 90 min. Other groups have reported values of 16 and 35 μM after oral administration of 600 mg and 1200 mg/day respectively. The plasma half life is estimated to be about 2.5 h and no NAC is detectable 10–12 h after administration [De Caro et al. 1989]. Higher concentrations in plasma may be achieved after intravenous administration. For example, infusion of 150 mg/kg results in a peak of 554 mg/liter (3.4 mM) within 15 min with a half life of 5.7 h [Prescott et al. 1989]. The proportion of NAC bound to proteins is relatively low during steady-state infusion (30–40%) but increases rapidly after completion of infusion (60–70%) [Harada et al. 2002]. In contrast to the increased level found in plasma, neither oral nor intravenous administration of NAC was followed by a significant increase in its levels or its metabolites [Macnee et al. 1991] in lung tissues or bronchoalveolar fluid [Bridgeman et al. 1994].
After absorption, NAC is rapidly metabolized to cysteine, which is a direct precursor in the synthesis of intracellular glutathione. In this way it acts as an antioxidant by restoring the pool of intracellular reduced glutathione, which is often depleted as a consequence of increased status of oxidative stress and inflammation [Santangelo, 2003; Rahman and Macnee, 2000]. Its antioxidant and anti-inflammatory properties have recently been reviewed [Sadowska et al. 2007].
N-Acetylcysteine in chronic obstructive pulmonary disease
Oral NAC has been used for decades as a mucolytic agent in several lung disorders.
Oral NAC has also been tested as a medication that may influence oxidative stress and inflammation in COPD and thus led to an improvement in lung function and a reduction in the exacerbation and hospitalization rates. As already mentioned, reports on the dose effects of NAC are not conclusive and, as described below, this is especially the case in patients with COPD who may have a different pharmacokinetic profile as a consequence of increased consumption and turnover [Sadowska et al. 2007].
NAC may exert its mucolytic and mucoregulatory action via several mechanisms (Figure 3). First, it works through depolymerization of the mucin glycoprotein oligomers by hydrolyzing the disulfide bonds that link the mucin monomers. This is possible because of the presence of free thiols (sulfhydryl groups). Therefore, NAC decreases the sputum viscosity in vitro [Sheffner, 1963; Davis et al. 1975] and acts as a mucolytic. Second, it plays a mucoregulatory role as it can decrease sputum hypersecretion in experimental rat models [Rogers et al. 1989]. Moreover, it has been demonstrated to inhibit the mucus secretory cell hyperplasia and enhanced expression of the MUC5AC gene in bleomycin-induced lung fibrosis in rats [Mata et al. 2003].

Effects of N-acetylcysteine (NAC) on mucus hypersecretion in chronic obstructive pulmonary disease (for references see text). FEV1, forced expiratory volume in 1 s.
As mentioned above, NAC can influence sputum production by reducing the oxidative stress. Under conditions of oxidative stress increased mucus secretion has been reported [Jeffery and Zhu,. 2002]. NAC has been reported to abolish the morphological changes in the endothelial cell monolayers induced by cigarette smoke [Schweitzer et al. 2011] and it can improve the antioxidant status of cells by increasing intracellular glutathione. Plasma glutathione has been reported to increase in patients with COPD after 5 days of NAC treatment (600 mg three times a day) but no effects were observed at the lower doses that were effective in healthy volunteers (600 mg/day) [Macnee et al. 1991; Bridgeman et al. 1994]. In patients with moderate COPD without inhaled steroid treatment, H2O2 in exhaled breath condensate decreased after 15 days of NAC treatment with a further decrease after 30 and 60 days of treatment. Lung function was not affected. Kasielski and Nowak did not observe any reduction in exhaled H2O2 in patients with stable COPD treated with NAC 600 mg/day for 6 months compared with those receiving placebo [Kasielski and Nowak, 2001]. However, 9 and 12 months of treatment with this lower dose did achieve significant reductions in exhaled H2O2. These different outcomes illustrate the importance of dose and duration, and confirm the potential of NAC to enhance the antioxidant capacity of plasma and the airspaces of the lungs against oxidant-induced injury. It could be suggested that the influence of NAC on redox status of the cell may indirectly affect sputum production.
As far as the inflammatory process in COPD is concerned, data are limited that claim the effectiveness of NAC. Van Overveld and colleagues reported a decrease in neutrophil chemoattractant properties in the sputum of patient with COPD after 8 weeks of NAC treatment at 600 mg/day [Van Overveld et al. 2000]. Since the main chemoattractants for neutrophils in sputum are IL-8 and leukotriene B4, this suggests that NAC decreased the concentration of those chemoattractants in the sputum. With regard to the effects of NAC treatment on clinical parameters such as lung function, exacerbation rate and hospitalization, the reports are equivocal.
In a retrospective study, Gerrits and colleagues observed that NAC intake is related to a 30% decreased risk of hospital readmission for COPD and that this risk reduction is dose dependent [Gerrits et al. 2003]. The review by Grandjean and colleagues based on eight long-term trials (>3 months) with dosages of 400–1200 mg/day reports a 23% decrease in exacerbation rate in the NAC-treated groups compared with placebo [Grandjean et al. 2000]. Nevertheless, the latest large-scale, prospective 3-year study, the Bronchitis Randomized on NAC Cost-Utility Study (BRONCHUS) did not observe any significant differences in the change in forced expiratory volume in 1 s or in the exacerbation rate after 3 years of NAC treatment compared with placebo [Decramer et al. 2005].
As far as the molecular effects of NAC on mucins are concerned, it has been reported that NAC can influence MUC5AC expression via several pathways. Namely, it has been reported that MUC5AC expression is increased by acrolein, an aldehyde component of cigarette smoke. Moreover, acrolein increased MUC5AC mRNA levels by phosphorylating EGFR and MAPK 3/2 or MAPK 3/2(ERK1/2). Pretreating the cells with an EGFR-neutralizing antibody, or a metalloproteinase inhibitor, decreased the acrolein-induced MUC5AC mRNA increase [Deshmukh et al. 2005]. Furthermore, MUC5AC expression was enhanced in H292 cells exposed to H2O2 compared with that in control cells. Pretreatment with NAC suppressed MUC5AC production and p38 activation. Blockage of p38 MAPK led to suppression of MUC5AC mRNA expression [Jang et al. 2010]. NAC has also been reported to inhibit the expression of NFκB which in turn influences MUC5AC expression acting via the EGFR pathway [Lu et al. 2011]. Interestingly, neutralizing antibodies to EGFR ligands failed to inhibit mucus production via neutrophil-derived oxidative stress, whereas NAC did abolish MUC5AC expression [Takeyama et al. 2000]. This suggests alternative pathways to mucus production than via the EGFR pathway, which is influenced by NAC. The simplified summary of a possible molecular mechanism of NAC is presented in Figure 4.

Possible points of action of N-acetylcysteine (NAC). NAC inhibits oxidative stress by acting as a direct reactive oxygen species (ROS) scavenger and by changing the cellular redox status. This, in turn, may influence nuclear factor-κB (NFκB) activation and modulate the inflammatory response . This can directly and indirectly influence MUC5AC activation and therefore mucus hypersecretion (for references see text). EGFR, epithelial growth factor receptor; GSH, reduced glutathione; iNOS, inducible nitric oxide synthase; MUC5AC, mucin 5AC; NO, nitric oxide.
In conclusion, NAC should be considered an interesting medication influencing inflammation, oxidative stress and mucus clearance. Unfortunately, a sufficient blood concentration is very difficult to achieve because of the fast turnover. Future research should focus on the components possessing the properties of NAC with a better pharmacokinetic profile.
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
The authors declare no conflicts of interest in preparing this article.