
Abstract
Introduction
Asthma is a chronic inflammatory disease that is underdiagnosed and undertreated and presents frequent exacerbations. The prevalence of asthma in different countries ranges from 1% to 18% [Global Initiative for Asthma, 2007], being up to 3%, despite underdiagnosis, in Spain [Adams et al. 2000; Cimas et al. 1997].
The natural history of asthma involves the presentation of exacerbations, which frequently lead patients to seek care urgently, at either an emergency department or a primary care centre. The frequency varies from 0.3% to 4.9% depending on the series consulted [Otero et al. 2002], and the hospitalization rate in Spain ranges from 1.3% to 1.6%. These exacerbations can be caused by the nature of asthma itself, but overall they are due to exogenous triggers such as respiratory infections, pollution, undertreatment or poor treatment compliance [Guilbert et al. 2010; Johnston and Sears, 2006]. It has been estimated that up to 60–80% of exacerbations could be prevented by proper treatment of the underlying disease and early medical attention, saving resources by reducing the number of patients visiting the emergency department [Adams et al. 2000]. For example, inadequate use of inhaled corticosteroids [Rowe et al. 2007; Rabe et al. 2000], which are the basis of asthma maintenance treatment, could prevent patients from developing exacerbations.
Primary care assistance, as the portal to the healthcare system, provides a privileged setting for physicians to evaluate and resolve most asthma exacerbations and could prevent emergency department overcrowding due to patients with mild to moderate asthma exacerbations seeking urgent medical attention. Nonetheless, the mortality rate due to asthma cannot be overlooked; thus, asthma exacerbations must be carefully evaluated and treated [Lincourt et al. 2010; Álvarez et al. 2004; Barnes, 2004; Gibson et al. 2003; Tomas, 2001].
Written self-management plans and follow-up visits can have a positive effect on the morbimortality of asthma exacerbations [Gibson et al. 2003]. It is necessary to follow medical consensus and guidelines to improve medical care [Lincourt et al. 2010; Global Initiative for Asthma, 2007;British Thoracic Society and Scottish Intercollegiate Guidelines Network, 2003; Plaza et al. 2003; Sociedad Española de Neumologia y Cirugia Torácica y Sociedad Española de Medicina Familiar y Comunitaria, 1998; Neville et al. 1997]. Clinical assessments are not compliant with guidelines in a considerable number of cases [Lincourt et al. 2010; Barnes, 2004; Neville et al. 1997]. However, there are few studies evaluating the implementation of asthma guidelines in hospitals [Adams et al. 2000] or in primary care centres [Molina et al. 2005; Neville et al. 1997].
The main objective of this study was to describe the approach to asthma exacerbations in an urban primary care centre, the particular characteristics of patients with asthma exacerbations, the treatment and evaluation implemented, and the rate of resolution achieved by the medical team.
Methods
This was a descriptive, cross-sectional study performed in an urban primary care centre in Barcelona (Nou Barris, CAP Chafarinas) from November 2008 to May 2009. A total of 15,472 patients over the age of 14 years old, mainly with a low socioeconomic level, were assigned to the center. The primary care centre is equipped with eight basic assistance units, each comprising a physician and a nurse.
The inclusion criteria were as follows: age older than 14 years; asthma diagnosed according to the 2007 Global Initiative for Asthma (GINA) criteria; and consultation for an asthma exacerbation. The following data were collected when the patient visited the centre: sex; age; smoking habit; type of asthma; maintenance treatment; reason for consulting; time since the beginning of the symptoms; possible triggers; physical examination [including measurement of peak expiratory flow (PEF; Mini-Bell Peak Flow Meter; Trimedica, Barcelona)]; severity of the exacerbation; type of exacerbation; treatment received at the centre and after discharge; high risk criteria; hospital referral; regular physician referral; and time spent at the doctor’s office.
A participant who consumed more than one cigarette per day was classified as a smoker and a participant who had abstained from smoking for longer than 1 year was classified as an exsmoker. The 2007 GINA criteria were followed to define and classify the types of asthma. The severity of asthma exacerbations was classified according to the SEPAR: Sociedad Españ ola de Neumologia y Cirugí a Torá cica–SEMFyC: Sociedad Españ ola de Medicina Familiar y Comunitária criteria. The severity criteria of exacerbations were taken from a previous publication [Plaza et al. 2003].
Interventions were evaluated following the SEPAR–SEMFyC guidelines. Mild asthma exacerbations were considered to be well treated when short-acting β2-adrenergic agents (SABAs) were given on demand, undertreated when no treatment was given at all, and overtreated if there was any other intervention. Moderate exacerbations were considered well treated when SABAs were given on demand and oral corticosteroids were added; the administration of SABAs, oral corticosteroids or ipratropium bromide alone or no treatment was considered as undertreatment. Other possible interventions were considered as overtreatment. Severe asthma exacerbations were considered as well treated with SABAs on demand, ipratropium bromide, oral corticosteroids and oxygen and the patient was referred to hospital if necessary; the absence of any of these interventions was considered to be undertreatment.
The treatment given after discharge was also evaluated. For mild exacerbations, treatment with SABAs on demand and inhaled corticosteroids was considered correct; treatment with SABAs or inhaled corticosteroids alone was considered undertreatment; and treatment with oral corticosteroids, long-acting β2-agonists (LABAs) or leukotriene modifiers was considered overtreatment. For moderate exacerbations, SABAs on demand and inhaled corticosteroids/LABAs and oral corticosteroids were considered the correct treatment. Lack of any of these elements was considered as undertreatment.
Therapeutic success was assessed according to the frequency of recovery after treatment and/or the need to refer the patient to the hospital to achieve control [Sociedad Española de Neumologia y Cirugia Torácica y Sociedad Española de Medicina Familiar y Comunitaria, 1998]. The criteria for recovery were as follows: normalization of pulmonary auscultation and breath frequency (<20/min); normalization of heart beat frequency (<100/min); PEF >80% of predicted value; and subjective improvement reported by the patient after treatment.
For statistical analysis, quantitative variables were expressed as means and standard deviation (SD) and qualitative variables were expressed as percentages. Association among qualitative variables was assessed with the Chi-square test. Mean values were compared using Student’s t-test and analysis of variance. The SPSS 10.0 software package was used to perform the statistical analyses. p < 0.05 was considered statistically significant.
Results
Characteristics of exacerbations
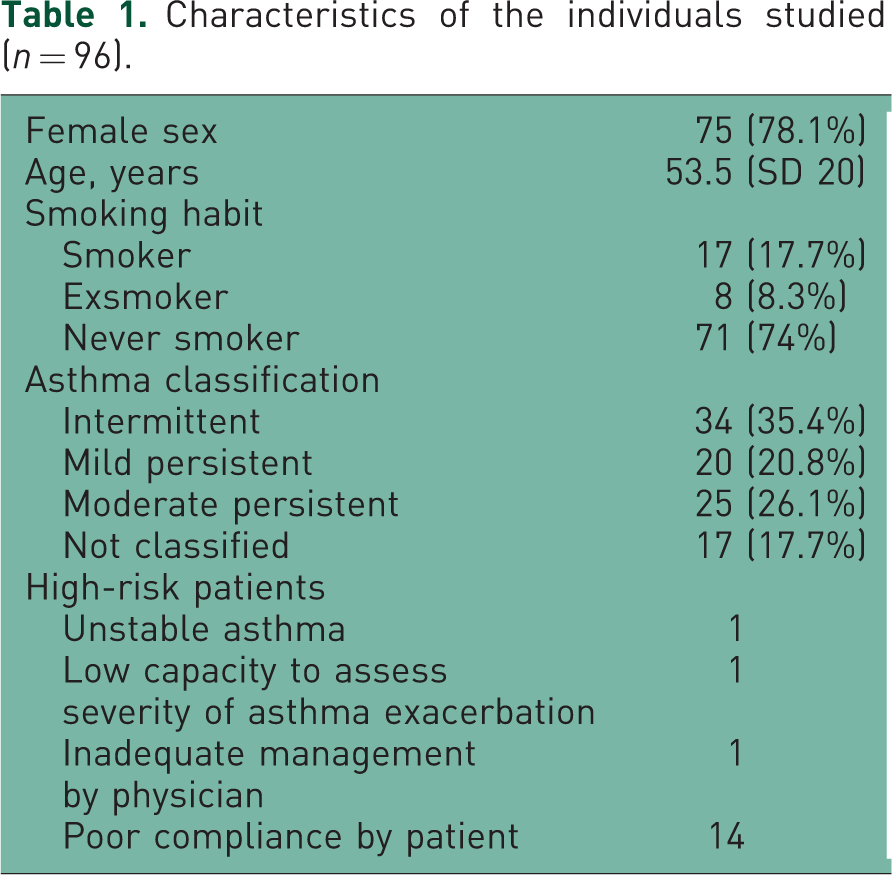
A total of 123 exacerbations were seen during the study period, corresponding to 96 patients, who had a mean age of 53.5 years (SD 20 years); 78.1% were females. Seventy-three patients attended the centre only once, 19 attended twice and the remaining patients attended three times. The characteristics of the individuals studied are shown in Table 1. Of the exacerbations seen, 74% were classified as mild, 24.4% as moderate and 1.6% as severe.
Characteristics of the individuals studied (n = 96).
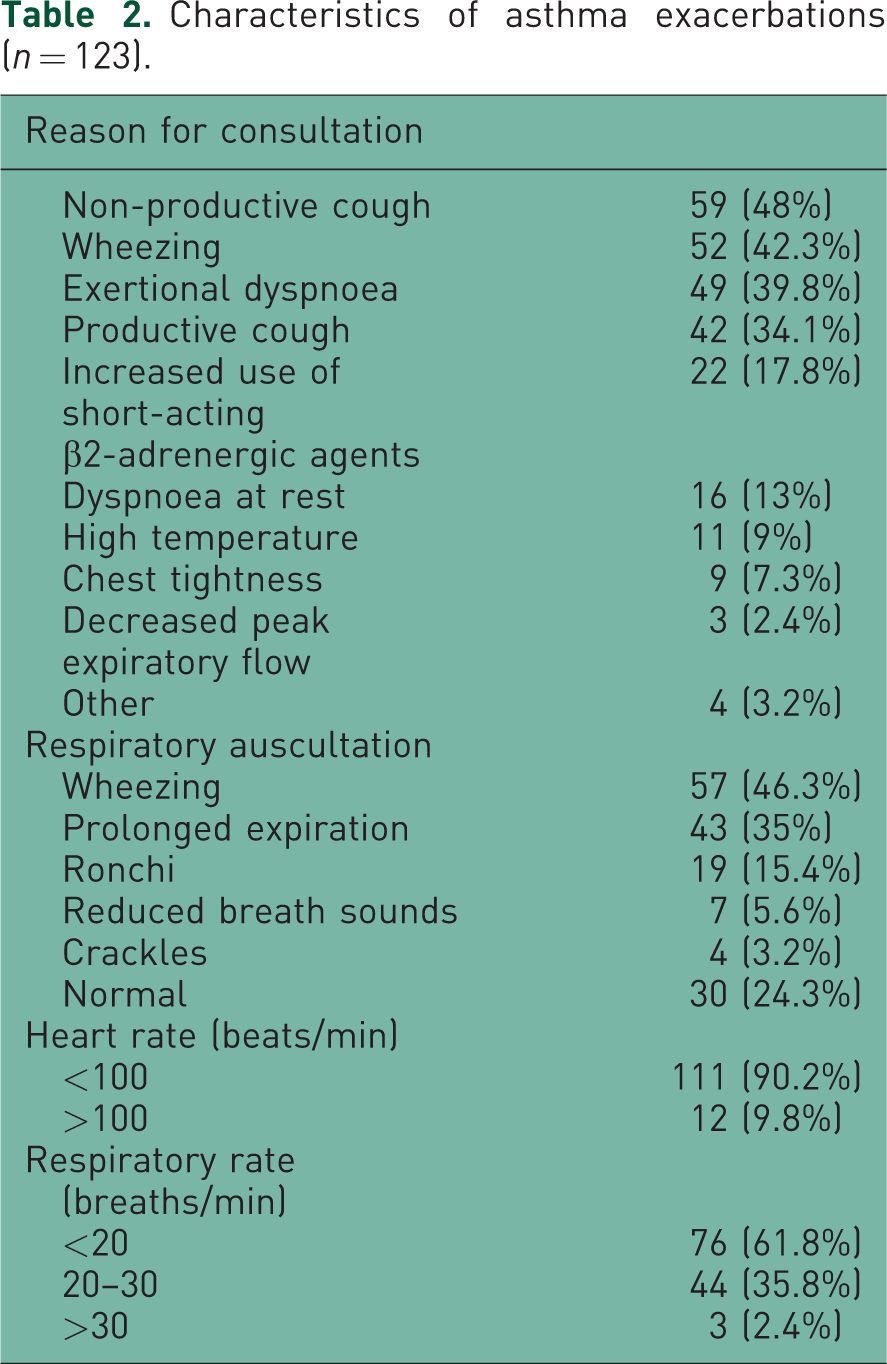
The most frequent reasons for consultation were as follows: non-productive cough (48%), wheezing (42.3%) and effort dyspnoea (39.8%) (Table 2). Common triggers were respiratory infections (78% of cases) and allergen exposure (13%). Data on the physical examination are shown in Table 2.
Characteristics of asthma exacerbations (n = 123).
PEF was measured in all patients, but the technique was only acceptable in 54.4% of patients, who had an average age of 43.2 years. The severity of exacerbation was not related to the process of taking the measurement (p > 0.05). The interval from symptom onset to seeking medical care was 5.8 days (95% confidence interval 4.7–6.9) and did not differ significantly according to exacerbation severity (Table 3).
Relation between type of exacerbation and duration of clinical course (days), average number of follow-up visits (expressed by median and standard deviation) and peak expiratory flow measurement (expressed by percentage).

Treatment of asthma exacerbations
Up to 23.9% of patients developed more than one exacerbation during the 6-month study period. Patients who were undertreated for their baseline asthma according to the GINA consensus presented more severe asthma exacerbations (p = 0.05) (Table 1). Patients with more severe asthma had more severe exacerbations (p < 0.05) (Figure 1), but the severity of exacerbation was not a predictive factor for relapse.

Relationship between type of asthma and severity of asthma exacerbation. Only two patients with severe persistent asthma experienced moderate exacerbations and there were only two severe exacerbations, one in a patient with mild persistent asthma and another with moderate asthma. These are not represented in the figure. There were significant differences between the distribution of severity of exacerbations according to the type of baseline asthma (p = 0.032).
No drug was prescribed in 33.3% of cases; salbutamol was given with a large-volume spacer chamber in 66.6% of cases, with the addition of oral corticosteroids in 8.1%. One course of salbutamol was given in 90.3% of exacerbations, two courses were given in 8.5% and three courses in 1.2%. No episodes were treated with parenteral corticosteroids, oxygen or ipratropium bromide.
The percentage of asthma exacerbations adequately treated according to the guidelines was 60.2% for mild, 26.7% for moderate and 0% for severe episodes. Deviation from the guidelines was due to undertreatment in all stages.
The average time to resolution of the exacerbation was 30.2 min (SD 16.5). The average number of follow-up visits after discharge was 3.3 (range 1–6), which did no show statistically differences related to the type of asthma nor the severity of the exacerbation. Only 8.9% of patients required sick leave, the duration of which averaged 8.4 days (SD 5.9).
Treatment after discharge
The frequency of resolution was 98.4%, since only two patients were referred to the emergency department; 18.6% of patients with exacerbations were discharged with antibiotic prescription; 34% of patients with exacerbations were given oral corticosteroids after discharge, of these exacerbations 38% were mild and 61.9% were moderate.
The treatment prescribed after discharge followed the guidelines in 27.3% of patients with a mild exacerbation and in 23.3% of patients with a moderate exacerbation. Overtreatment was identified in 69.3% of mild and in 13.3% of moderate exacerbations. Only 3.4% of the mild but up to 69.3% of the moderate exacerbations were undertreated. Treatment of severe exacerbations after discharge was not analysed because of patient referral to hospital.
Discussion
The predominance of females (78.1%) among the asthmatic patients in this study is remarkable. The estimated prevalence of females within the asthmatic population in Spain is 52.9–63.9% [Bassagana et al. 2001]. Moreover, 64% of the asthmatic patients assigned to the primary care centres are females according to the latest census of patients.
The frequency of exacerbation resolution by the primary care physicians was optimal, with only 1.6% of patients referred to hospital. This is similar to previous, albeit limited, studies performed in primary care in Spain [Molina et al. 2005; Neville et al. 1997].
As in acute exacerbations of other chronic diseases, exacerbation of asthma can be dealt with in primary care [Global Initiative for Asthma, 2007; Molina et al. 2005; Plaza et al. 2003; Neville et al. 1997] and most of these episodes can be resolved without referral to hospital. To achieve this objective, a good professional standard and good motivation are needed, together with less tight schedules, since attending an asthma exacerbation took an average of 30 min. This time may appear to be excessive considering the large work load of primary care teams and the short time available for each patient [Barnes, 2004]. This is an important limiting factor, since patients with mild or moderate exacerbations should be under observation in a primary care centre for at least for 1 h to confirm clinical stability before discharge [Wilson et al. 2003]. Adequate care of an exacerbation does not finish with the discharge of the patient. This is the most appropriate time to reinforce healthcare education, to set a date for the follow-up visit and, in some patients, to implement a self-management plan [Lincourt et al. 2010; Global Initiative for Asthma, 2007; Álvarez et al. 2004].
Several studies, most of them performed in the hospital setting, have shown important drawbacks in the approach to patients with an asthma exacerbation [Barnes, 2004; Adams et al. 2000; Cimas et al. 1997]. Initial management of an asthma exacerbation should aim to establish its severity, combining clinical parameters with objective measurements, at the same time as the first treatment is given. The same parameters must be evaluated in subsequent visits, bearing in mind that subjective assessment of improvement of dyspnoea is not reliable and must be complemented with measurement of PEF and physical examination (respiration rate, heart rate and respiratory auscultation). Pulse oximetry could also help in making therapeutic decisions and should always be performed in the most severe exacerbations; unfortunately, this measurement was not done because the devices were not available at the centre at the time of the present study. In the study of De Diego Damiá (2000), the initial value of PEF and changes in the value after treatment were the only factors that predicted the course of acute exacerbation of asthma. In our study an attempt was made to measure PEF in every patient, but a valid measurement was obtained in little more than half of the episodes (because of inappropriate technique by the patient). Similarly, other studies have reported the measurement of PEF in 30–76% of episodes [Global Initiative for Asthma, 2007; Wilson et al. 2003; Neville et al. 1997]. Nonetheless, our results are better than those reported by Álvarez and colleagues (2004), who observed that only 18% of patients had undergone PEF measurement in the primary care setting in Spain. It is worth noting that in our study PEF was determined more frequently in younger patients, perhaps because elderly patients did not understand the technique well. The PEF measurement is a more reliable indicator of the severity of airflow limitation than the severity of symptoms, and is available in most primary care centres and doctor’s offices. Unfortunately, healthcare education related to the use of PEF in asthma attacks is still lacking and this measurement is not routinely used in medical practice in Spain.
Asthma severity was classified according to GINA guidelines [Global Initiative for Asthma, 2007]. There are differences in the proportions of all types of asthma in this study compared with the literature [Molina et al. 2005; Rabe et al. 2000], particularly regarding the small number of severe asthma cases. These differences may occur because previous studies were performed in the hospital setting, and also because patients with severe asthma are frequently referred to hospital for follow up, so they may preferentially attend the emergency department when an exacerbation occurs. In another study performed in primary care, the mild type of exacerbation was predominant, followed by the moderate type [Molina et al. 2005]. In addition, a significant number of severe asthma exacerbations develop at night, related to the circadian rhythm of airway obstruction; because the primary care centre is closed at night, this may account in part for the low number of attendances for severe attacks.
The frequency of use of SABAs in this study was low, despite this being one of the main treatments for exacerbations [Wilson et al. 2003]. This may be because physicians do not appreciate the importance of mild exacerbations. In this study, all treatments with SABAs were given using a large-volume chamber, in contrast to other studies in primary care and in hospitals reporting a predominance of treatment by nebulization. The use of a large-volume chamber was sufficient to resolve most exacerbations [Cates et al. 2006; Neville et al. 1997].
Prescription of oral corticosteroids after discharge was observed in 35.7% of exacerbations, a lower percentage than that described in other studies. International guidelines do not recommend the use of antibiotics [Global Initiative for Asthma, 2007], though these were prescribed in 18.6% of exacerbations in our study. Another study reported antibiotic prescription in 40% of exacerbations [Neville et al. 1997]. Patients often develop symptoms suggestive of underlying infection, possibly indicating a subjacent inflammatory process or a viral infection, which some physicians may erroneously interpret as being caused by bacterial infection. Antibiotic use should be restricted to patients with clear evidence of pneumonia or to situations in which there is no adequate response to anti-inflammatory medication. In the present study no patient received parenteral corticosteroids, which is in agreement with the evidence indicating that oral administration is as effective as the intramuscular or the intravenous route [Fitzgerald, 2001; Manser et al. 2001].
It is important to emphasize that, as observed by Molina and colleagues (2005), patients with undertreatment at baseline presented more severe exacerbations. This is another consequence of noncompliance with guidelines for the treatment of asthma.
The results obtained in this study confirm that treatment of asthma exacerbations is frequently inadequate and it is not often developed following existing guidelines [Neville et al. 1997]. Undertreatment during acute exacerbation and after discharge are key aspects of asthma management. Activities to promote knowledge of guidelines and implement their use would lead to an improvement in results. Wider prescription of anti-inflammatory medications is needed. On the other hand, physicians require sufficient time to attend patients with an acute exacerbation [Barnes, 2004], since the intervention of primary care physicians is crucial in reducing the morbidity of asthma exacerbations.
This study was designed and developed in an urban primary care centre. It demonstrates the effectiveness of the primary care team in resolving most asthma exacerbations while also bringing to light many aspects that need to be improved in the management of acute asthma exacerbations in primary care. However, as this study was carried out in only one primary care centre in an urban area, its conclusions cannot be extrapolated to other geographical areas. Further extensive studies are required in order to improve understanding of the quality of the medical care of this frequent disease.
Footnotes
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
The authors declare no conflicts of interest in preparing this article.