
Abstract
Background:
Suboptimal adherence to maintenance medication has been associated with poor outcomes in asthma. This study examined single-inhaler inhaled corticosteroid (ICS)/long-acting β2 agonist (LABA) adherence and asthma-related outcomes.
Methods:
This retrospective observational study of patients with asthma initiating ICS/LABA used data from IQVIA PharMetrics Plus (1 January 2014–31 March 2019). Patients included were ⩾18 years old and had ⩾12 months continuous eligibility before, and ⩾180 days follow-up after, the index date. Adherence was measured as proportion of days covered ([PDC] adherent ⩾ 0.8; non-adherent <0.8) each quarter, with outcomes measured each subsequent quarter. Endpoints were asthma-related overall and severe (inpatient/emergency department [ED] visit) exacerbations, rescue medication use, and asthma-related healthcare resource utilization and costs. Regression models evaluated associations between adherence and outcomes, controlling for repeated measures and differences in baseline characteristics.
Results:
Overall, 50,037 patients were included (mean age 45.3 years; mean follow-up 23.3 months). Adherent patients were less likely to experience asthma-related overall (adjusted odds ratio [aOR] 95% confidence interval [CI]: 0.942 [0.890, 0.998]; p = 0.041), or severe exacerbations (aOR [95% CI]: 0.778 [0.691, 0.877]; p < 0.001) per quarter versus non-adherent patients. Adherent patients had lower severe exacerbation rates (adjusted rate ratio [aRR] [95% CI]: 0.792 [0.702, 0.893]; p < 0.001) but similar overall exacerbation rates (aRR [95% CI]: 0.993 [0.945, 1.044]; p = 0.783) versus non-adherent patients. The odds of rescue medication use were lower per 20% PDC increase (aOR [95% CI] short-acting β2 agonist: 0.991 [0.985, 0.996]; p = 0.001; oral corticosteroid: 0.988 [0.982, 0.995]; p < 0.001). Adherent patients were less likely to visit EDs per quarter (aOR [95% CI]: 0.775 [0.680, 0.883]; p < 0.001) and odds of hospitalization were lower per 20% PDC increase (aOR [95% CI]: 0.930 [0.881, 0.982]; p = 0.009). Across most measures, adherent patients incurred lower costs.
Conclusion:
This real-world study highlights the short-term clinical and economic benefits of ICS/LABA adherence in asthma, particularly in reducing severe exacerbations.
Introduction
Asthma is a chronic respiratory disease characterized by inflammation-mediated narrowing of airways that can limit airflow to and from the lungs. 1 In the United States, asthma is a prevalent disease that affected more than 25 million individuals in 2019 2 and, globally, asthma was the second leading cause of death and morbidity among chronic respiratory diseases in 2017. 3 In addition to its substantial clinical burden, asthma is also associated with a considerable economic burden, which was estimated at $81.9 billion (US dollars) in 2013 in the United States. 4 Despite advances in asthma management, the disease remains uncontrolled in approximately half of patients in the United States.5,6 Uncontrolled asthma is associated with higher medical costs and increased risk of exacerbations, highlighting important unmet needs among patients.7–9 Treatment with inhaled corticosteroids (ICSs) is the cornerstone of long-term asthma maintenance treatment and is recommended by the national asthma treatment guidelines as a preferred component of maintenance therapy for persistent asthma.1,10 However, for patients who are unable to control their asthma symptoms with ICS alone, the addition of long-acting β2 agonists (LABAs) to the treatment regimen is recommended,1,10 and these are available as fixed combination (ICS/LABA) therapies (examples available in the United States include fluticasone propionate/salmeterol [FP/SAL], fluticasone furoate/vilanterol [FF/VI], mometasone/formoterol [M/FOR], and budesonide/formoterol [BUD/FOR]). 11
Adherence to medication has been highlighted as an important component in asthma management.1,10 Suboptimal adherence to ICS-containing medications has been associated with poor asthma outcomes, including increased morbidity, mortality, and healthcare resource utilization (HRU).12,13 Two studies have reported that improved adherence to FP/SAL therapy is associated with fewer asthma exacerbations, reduced asthma-related HRU, and improved asthma control.12,13 However, there is limited real-world information available on the association between adherence and asthma outcomes in patients who are prescribed other ICS/LABAs.
This study used a large claims database, representing multiple commercial health plans in the United States, to evaluate the relationship between adherence to single-inhaler fixed-dose combination ICS/LABAs and asthma outcomes, including asthma-related exacerbations, rescue medication (short-acting β2 agonist [SABA] and oral corticosteroid [OCS]) use, asthma-related HRU, and asthma-related healthcare costs, among adult patients with asthma.
Methods
Data source
Health insurance claims from the IQVIA PharMetrics Plus database were used, with data from 1 January 2014 to 31 March 2019. This database comprises more than 150 million unique enrollees across all 50 US states, and patients have an average health plan enrollment of 39 months. Commercial insurance is the most frequent plan type captured (the database is generally representative of the <65 years of age, commercially insured population in the United States), but other types can also be found, including commercial Medicare, commercial Medicaid, self-insured employer groups (as managed by health plan), and pharmacy-only plans. The database contains data on patient demographics, health plan enrollment, as well as inpatient, outpatient (OP), and pharmacy claims. The data comply with the Health Insurance Portability and Accountability Act and are de-identified.
Study design
This was a retrospective, longitudinal, open-cohort study of patients with asthma using single-inhaler ICS/LABA and the association between adherence to these ICS/LABA medications and asthma outcomes. The study design, shown in Figure 1, was similar to previously published work. 12
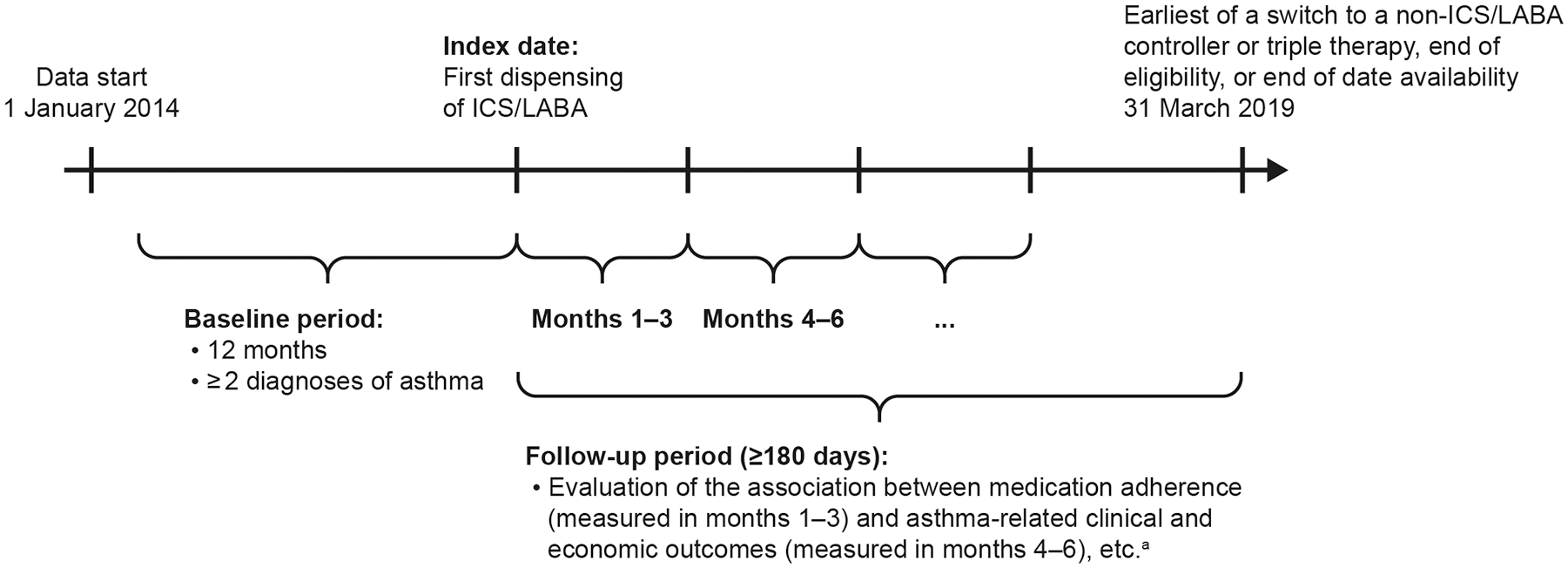
Study design.
The index date was defined as the date of the first dispensing of fixed-dose ICS/LABA in the study period. Patient characteristics were evaluated in the 12-month period prior to the index date (baseline period). The follow-up period spanned from the index date until the earliest of: a switch from the index medication to a non-ICS/LABA single-maintenance medication (ICS-, LABA-, or long-acting muscarinic antagonist [LAMA]-containing single inhaler); a switch to triple therapy (single-inhaler or multiple-inhaler triple therapy, defined as ⩾1 overlapping days’ supply for fills of an ICS, LABA, and LAMA in any formulation); health plan disenrollment; or end of data availability (31 March 2019).
The follow-up period was partitioned into quarterly (90-day) intervals. Adherence to ICS/LABA was measured in each quarter, and the relationship with asthma-related outcomes was evaluated in the subsequent quarter for all complete quarters of follow-up (Figure 1). The first quarter was reserved for the assessment of medication adherence, and asthma-related outcomes were evaluated from the second-quarter onwards; patients were thus required to have at least two quarters (⩾180 days) of follow-up data available. Adherence was measured by the proportion of days covered (PDC). PDC was calculated for each quarter by dividing the number of days that ICS/LABA medication was available (based on filled prescriptions) over 90 days. Patients were classified via an open-cohort approach as adherent (PDC ⩾ 0.8) or non-adherent (PDC < 0.8) for each quarter.
Study population
Patients ⩾ 18 years of age at the index date with ⩾ 2 dispensings for fixed-dose ICS/LABA during the study period (first dispensing defined as the index date) were included according to the following criteria: ⩾ 2 diagnoses of asthma (International Classification of Diseases [ICD]-9-CM: 493.0x, 493.1x, 493.8x, 493.9x; ICD-10-CM: J45.3x, J45.4x, J45.5x, J45.9xx) in any position during the baseline period or on the index date; ⩾ 12 months of continuous eligibility prior to the index date; and ⩾ 180 days of follow-up after the index date. Patients were excluded if they had any of the following conditions or procedures during the baseline or follow-up periods: chronic obstructive pulmonary disease (COPD) or asthma/COPD overlap syndrome; lung cancer; bronchiectasis; alpha-1 antitrypsin deficiency; or lung transplant. Patients were also excluded if they had acute respiratory failure, cystic fibrosis, or a pharmacy claim for LAMA during the baseline period or on the index date.
Study endpoints
The primary endpoint for this study was asthma-related overall exacerbations, reported as the proportion of patients who had at least one exacerbation and the rate of exacerbations per patient per quarter (PPPQ). Asthma-related overall exacerbations were defined as an asthma-related (based on a primary diagnosis of asthma) inpatient (IP) visit or emergency department (ED) visit, or an asthma-related OP visit with a systemic corticosteroid dispensing (for acute treatment of asthma) within ±5 days of the visit. If two or more exacerbations were observed for a patient within 14 days of each other, they were considered as one exacerbation episode and classified based on the highest severity contributing event. 9
Secondary endpoints included asthma-related severe exacerbations, defined as an asthma-related IP or ED visit; SABA and OCS use; and asthma-related (identified with a primary diagnosis of asthma) HRU and medical costs. Severe exacerbations were reported as the proportion of patients who had at least one severe exacerbation and the rate of severe exacerbations PPPQ. SABA and OCS use were reported as the proportion of patients who had at least one dispensing, and the rate of canister dispensings PPPQ. HRU was reported as the proportion of patients with at least one visit (hospitalization, ED visit, OP visit) and as the rate of visits PPPQ. Total medical costs were reported PPPQ and stratified by hospitalization, ED visit, and OP visit components. Due to the high proportion of patients with zero costs, cost outcomes were evaluated among patients with any asthma-related hospitalization, ED visit, or OP visit costs in a given quarter.
Statistical analyses
Baseline characteristics were reported using descriptive statistics. Differences in baseline characteristics between cohorts were assessed using the standardized difference (std. diff.); a std. diff. of <10% was considered as a negligible imbalance between cohorts. 14 A generalized estimating equations (GEEs) approach was used to control for repeated measures and the correlation of observations within patients, and multivariable adjustment was used to control for differences in baseline characteristics between adherent and non-adherent patients. Odds ratios (ORs) with 95% confidence intervals (CI) and p values were reported for categorical outcomes and were calculated from GEE models with binomial distribution (ie, logistic regression). Rate ratios (RRs) with 95% CIs and p values were reported for continuous outcomes and were calculated from GEE models with Poisson distribution. Mean cost differences from GEE models were reported for cost outcomes; because cost data are positive values that follow a non-normal distribution, 95% CIs and p values were calculated using non-parametric bootstrap procedures. 15 All costs were inflation-adjusted to 2019 US dollars based on the medical care component of the Consumer Price Index. Effect measures (ORs, RRs, and cost differences) were reported for adherent (PDC ⩾ 0.8) versus non-adherent (PDC < 0.8) patients and per 20% increase in PDC.
Results
Baseline patient characteristics
Of 707,639 adult patients with at least two dispensings of single-inhaler fixed-dose ICS/LABA between January 2014 and March 2019, a total of 50,037 met all study inclusion and exclusion criteria (Figure 2).

Patient disposition.
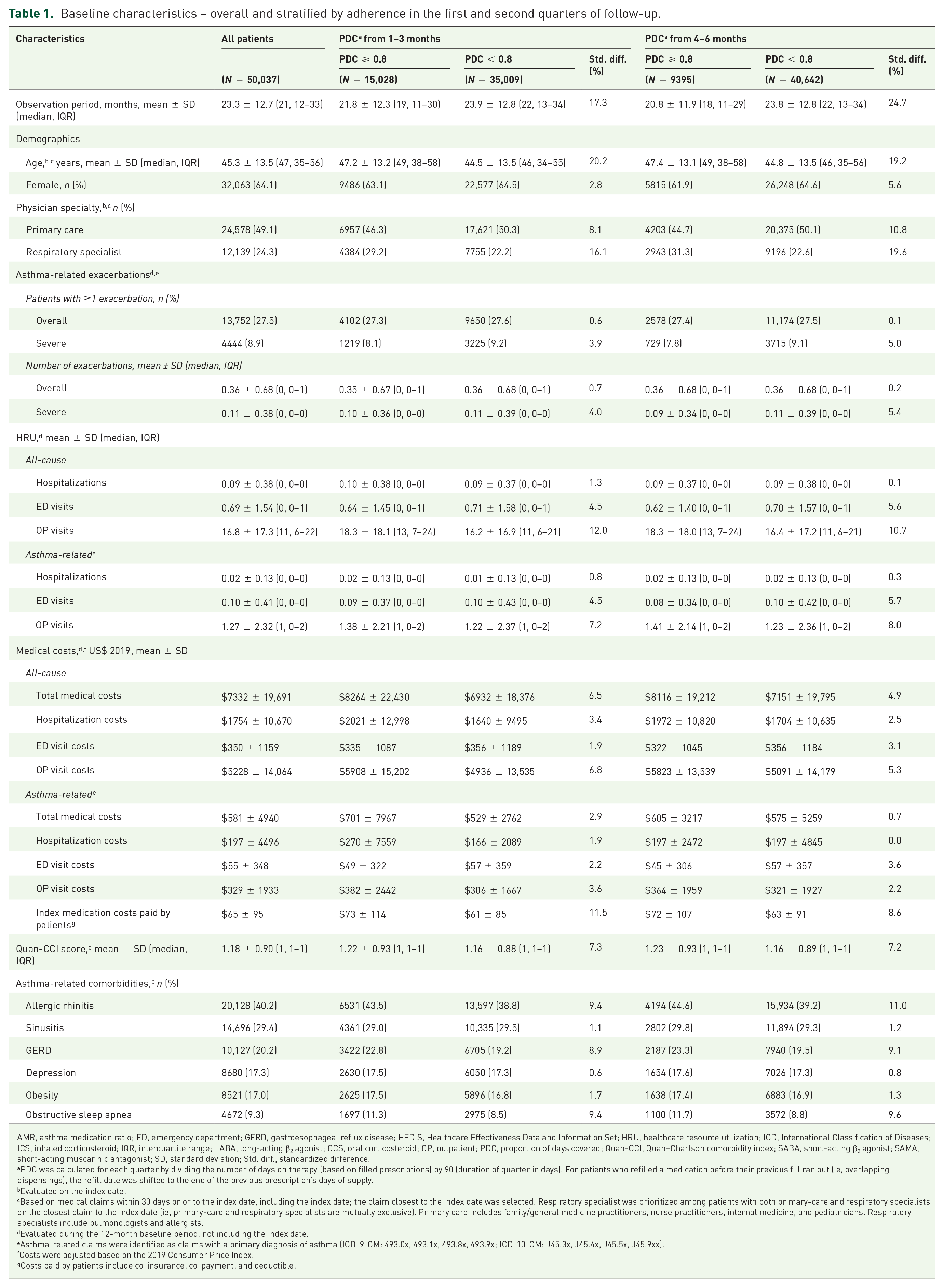
In the first quarter of follow-up, 15,028 patients (30.0%) were adherent (PDC ⩾ 0.8) and 35,009 (70.0%) were non-adherent (PDC < 0.8) to ICS/LABA treatment (Table 1).
Baseline characteristics – overall and stratified by adherence in the first and second quarters of follow-up.
AMR, asthma medication ratio; ED, emergency department; GERD, gastroesophageal reflux disease; HEDIS, Healthcare Effectiveness Data and Information Set; HRU, healthcare resource utilization; ICD, International Classification of Diseases; ICS, inhaled corticosteroid; IQR, interquartile range; LABA, long-acting β2 agonist; OCS, oral corticosteroid; OP, outpatient; PDC, proportion of days covered; Quan-CCI, Quan–Charlson comorbidity index; SABA, short-acting β2 agonist; SAMA, short-acting muscarinic antagonist; SD, standard deviation; Std. diff., standardized difference.
PDC was calculated for each quarter by dividing the number of days on therapy (based on filled prescriptions) by 90 (duration of quarter in days). For patients who refilled a medication before their previous fill ran out (ie, overlapping dispensings), the refill date was shifted to the end of the previous prescription’s days of supply.
Evaluated on the index date.
Based on medical claims within 30 days prior to the index date, including the index date; the claim closest to the index date was selected. Respiratory specialist was prioritized among patients with both primary-care and respiratory specialists on the closest claim to the index date (ie, primary-care and respiratory specialists are mutually exclusive). Primary care includes family/general medicine practitioners, nurse practitioners, internal medicine, and pediatricians. Respiratory specialists include pulmonologists and allergists.
Evaluated during the 12-month baseline period, not including the index date.
Asthma-related claims were identified as claims with a primary diagnosis of asthma (ICD-9-CM: 493.0x, 493.1x, 493.8x, 493.9x; ICD-10-CM: J45.3x, J45.4x, J45.5x, J45.9xx).
Costs were adjusted based on the 2019 Consumer Price Index.
Costs paid by patients include co-insurance, co-payment, and deductible.
Baseline characteristics, overall and stratified by adherence in the first and second quarters of follow-up, are presented in Table 1 and Supplementary Table S1. Overall, the mean follow-up duration was 23.3 months, mean age was 45.3 years, and 64.1% of patients were female. Slightly more adherent patients had respiratory specialists as their index ICS/LABA prescribing physicians, and fewer had primary-care-prescribing physicians versus non-adherent patients. Approximately half of patients used a maintenance medication prior to initiating ICS/LABA, with a higher proportion in the adherent versus non-adherent cohort (54.6% vs 45.3%; std. diff. 18.7%). Similar rates of baseline exacerbations were observed in the adherent and non-adherent groups; 27.5% of all patients experienced at least one asthma-related exacerbation, and 8.9% had a severe exacerbation in the baseline period. Adherent patients incurred slightly higher all-cause medical costs during baseline (adherent: $8264; non-adherent: $6932; std. diff. 6.5%), mainly driven by higher all-cause OP costs, and asthma-related medical costs were well balanced. The mean Quan–Charlson comorbidity index score was 1.18 and was similar between adherent and non-adherent patients. The most common asthma-related comorbidities were allergic rhinitis (40.2%), sinusitis (29.4%), and gastroesophageal reflux disease (20.2%). Similar trends in characteristics between adherent and non-adherent patients were observed in the second quarter.
Adherence to ICS/LABA
Adherence (PDC ⩾ 0.8) decreased sharply from 30.0% in the first quarter to 18.8% in the second quarter of follow-up. Mean PDC (standard deviation) was 0.63 (0.26) in the first quarter and 0.37 (0.36) in the second quarter of follow-up. Thereafter, adherence decreased more gradually to a stable 12–13% by the sixth quarter of follow-up (data not shown).
Asthma-related exacerbations
The rate of asthma-related overall exacerbations over the entire follow-up period (excluding the first quarter) was 16.4 per 100 person-years, and 20.6% of patients had at least one overall exacerbation. The rate of asthma-related severe exacerbations (defined by asthma-related IP or ED visit) was 3.62 per 100 person-years, and 5.2% of patients had at least one severe exacerbation during follow-up (Supplementary Table S2). During the first quarter of follow-up, adherent patients generally experienced slightly fewer exacerbations than non-adherent patients (Supplementary Table S3). Throughout the entire follow-up period, roughly 3–5% of both adherent and non-adherent patients had at least one overall exacerbation per quarter, and 0–1% had at least one severe exacerbation (data not shown).
After adjusting for differences in baseline patient characteristics, adherent patients were significantly less likely to experience any asthma-related exacerbation in the quarter following assessment when compared with non-adherent patients (adjusted OR [aOR] [95% CI]: 0.942 [0.890, 0.998]; p = 0.041), though the rate of asthma-related overall exacerbations PPPQ was similar between the groups (adjusted RR [aRR] [95% CI]: 0.993 [0.945, 1.044]; p = 0.783; Table 2).
Impact of ICS/LABA adherence on asthma-related exacerbations.

CI, confidence interval; ED, emergency department; GEE, generalized estimating equations; HRU, healthcare resource utilization; ICS, inhaled corticosteroid; LABA, long-acting β2 agonist; OP, outpatient; OR, odds ratio; PDC, proportion of days covered; PPPQ, per patient per quarter; Quan-CCI, Quan–Charlson comorbidity index; Ref, reference; RR, rate ratio; SABA, short-acting β2 agonist; std. diff., standardized difference.
Results calculated using GEE.
Adjusted models control for baseline covariates with ⩾10% std. diff. between adherent (PDC ⩾ 0.8) and non-adherent (PDC < 0.8) patients in the first or second quarters, as well as Quan-CCI, baseline HRU, and baseline healthcare costs. The variables included were the following: age, year of index date, physician specialty (primary care and respiratory specialist), medication use (number of unique medication class categories, use of any maintenance medication, number of SABA canisters, asthma medication ratio, and ICS dose of index medication), comorbidities (Quan-CCI, allergic rhinitis, obstructive sleep apnea), baseline HRU (all-cause and asthma-related hospitalizations, ED visits, and OP visits), and baseline healthcare costs (all-cause and asthma-related hospitalization costs, ED visit costs, OP visit costs, and patient-paid index medication costs).
The rate of asthma-related severe exacerbations PPPQ was significantly lower for adherent patients than non-adherent patients (aRR [95% CI]: 0.792 [0.702, 0.893]; p < 0.001). Adherent patients were significantly less likely to experience an asthma-related severe exacerbation per quarter than non-adherent patients (aOR [95% CI]: 0.778 [0.691, 0.877]; p < 0.001). Similar patterns were observed when comparing continuous change in PDC per 20% incremental increase: the odds of an overall exacerbation per quarter decreased by 3.9% per 20% increase in PDC (p < 0.001), and the odds of a severe exacerbation decreased by 4.8% per 20% increase in PDC (p < 0.001; Table 2).
Rescue medication use
Overall, approximately 22–37% of patients used SABA per quarter (data not shown). The odds of SABA use were significantly lower per 20% increase in PDC of ICS/LABA (aOR [95% CI]: 0.991 [0.985, 0.996]; p = 0.001), though the difference between adherent and non-adherent patients (based on 0.8 PDC threshold) was not statistically significant (aOR [95% CI]: 0.991 [0.966, 1.017]; p = 0.490; Table 3).
Impact of ICS/LABA adherence on SABA and OCS use.

CI, confidence interval; ED, emergency department; HEDIS, Healthcare Effectiveness Data and Information Set; HRU, healthcare resource utilization; ICS, inhaled corticosteroid; LABA, long-acting β2 agonist; OCS, oral corticosteroid; OP, outpatient; OR, odds ratio; PDC, proportion of days covered; PPPQ, per patient per quarter; Quan-CCI, Quan–Charlson comorbidity index; Ref, reference; RR, rate ratio; SABA, short-acting β2 agonist; std. diff., standardized difference.
Results calculated using generalized estimating equations.
For SABA use, canisters were defined based on HEDIS guidelines. One canister of inhaled SABA contains 100 doses of albuterol and equates to 100 doses of a nebulized albuterol.
Adjusted models control for baseline covariates with ⩾10% std. diff. between adherent (PDC ⩾ 0.8) and non-adherent (PDC < 0.8) patients in the first or second quarters, as well as Quan-CCI, baseline HRU, and baseline healthcare costs. The variables included were the following: age, year of index date, physician specialty (primary care and respiratory specialist), medication use (number of unique medication class categories, use of any maintenance medication, number of SABA canisters, asthma medication ratio, and ICS dose of index medication), comorbidities (Quan-CCI, allergic rhinitis, and obstructive sleep apnea), baseline HRU (all-cause and asthma-related hospitalizations, ED visits, and OP visits), and baseline healthcare costs (all-cause and asthma-related hospitalization costs, ED visit costs, OP visit costs, and patient-paid index medication costs).
Increased adherence (per 20% PDC) did not have a significant impact on the number of SABA canisters used (aRR: 1.00; p = 0.867), though adherent patients had a higher relative rate of use of SABA canisters than non-adherent patients (aRR [95% CI]: 1.048 [1.025, 1.072]; p < 0.001).
Overall, 12–26% of patients used OCS per quarter (data not shown). As with SABA rescue medication, the odds of OCS use was significantly lower per 20% increase in PDC (aOR [95% CI]: 0.988 [0.982, 0.995]; p < 0.001) though the difference between adherent and non-adherent patients was not statistically significant (aOR [95% CI]: 0.982 [0.954, 1.011]; p = 0.215). Rates of OCS dispensings PPPQ were significantly lower per 20% increase in PDC (aRR [95% CI]: 0.993 [0.987, 0.999]; p = 0.023), but there was no significant difference between adherent and non-adherent patients (aRR [95% CI]: 1.007 [0.979, 1.035]; p = 0.635; Table 3).
Asthma-related HRU
Hospitalizations and ED visits were rare, with approximately 0–0.3% of patients having a hospitalization per quarter and 0–1% of patients having an ED visit per quarter; OP visits were more common, with roughly 15–23% of adherent patients and 9–19% of non-adherent patients having an OP visit per quarter (data not shown). The odds of hospitalization was significantly lower by 7.0% per 20% increase in PDC (aOR [95% CI]: 0.930 [0.881, 0.982]; p = 0.009); though the difference between adherent and non-adherent patients was non-significant (aOR [95% CI]: 0.824 [0.638, 1.063]; p = 0.136; Table 4).
Impact of ICS/LABA adherence on asthma-related HRU.

AMR, asthma medication ratio; CI, confidence interval; ED, emergency department; HRU, healthcare resource utilization; ICS, inhaled corticosteroid; LABA, long-acting β2 agonist; OP, outpatient; OR, odds ratio; PDC, proportion of days covered; PPPQ, per patient per quarter; Quan-CCI, Quan–Charlson comorbidity index; Ref, reference; RR, rate ratio; SABA, short-acting β2 agonist; std. diff., standardized difference.
Results calculated using generalized estimating equations.
Asthma-related claims were identified as claims with a primary diagnosis of asthma (ICD-9-CM: 493.0x, 493.1x, 493.8x, 493.9x; ICD-10-CM: J45.3x, J45.4x, J45.5x, J45.9xx).
Adjusted models control for baseline covariates with ⩾10% std. diff. between adherent (PDC ⩾ 0.8) and non-adherent (PDC < 0.8) patients in the first or second quarters, as well as Quan-CCI, baseline HRU, and baseline healthcare costs. The variables included were the following: age, year of index date, physician specialty (primary care and respiratory specialist), medication use (number of unique medication class categories, use of any maintenance medication, number of SABA canisters, AMR, and ICS dose of index medication), comorbidities (Quan-CCI, allergic rhinitis, and obstructive sleep apnea), baseline HRU (all-cause and asthma-related hospitalizations, ED visits, and OP visits), and baseline healthcare costs (all-cause and asthma-related hospitalization costs, ED visit costs, OP visit costs, and patient-paid index medication costs).
Due to the correlation between asthma-related OP visits in baseline and follow-up, the list of covariates for adjustment was limited to age, year of index date, physician specialty (primary care and respiratory specialist), medication use (number of unique medication class categories, use of any maintenance medication, number of SABA canisters, AMR, and ICS dose of index medication), comorbidities (Quan-CCI, allergic rhinitis, and obstructive sleep apnea), baseline HRU (all-cause hospitalizations, ED visits, and OP visits, and asthma-related hospitalizations and ED visits), and baseline healthcare costs (all-cause and asthma-related hospitalization costs, ED visit costs, OP visit costs, and patient-paid index medication costs).
Adherent patients were significantly less likely to have an ED visit per quarter than non-adherent patients (aOR [95% CI]: 0.775 [0.680, 0.883]; p < 0.001) and the odds of an ED visit decreased by 4.7% per 20% increase in PDC (p < 0.001). In addition, adherent patients were significantly more likely to have an OP visit per quarter than non-adherent patients (aOR [95% CI]: 1.187 [1.154, 1.221]; p < 0.001). Similar results were found for the rates of hospitalizations, ED visits, and OP visits.
Asthma-related healthcare costs
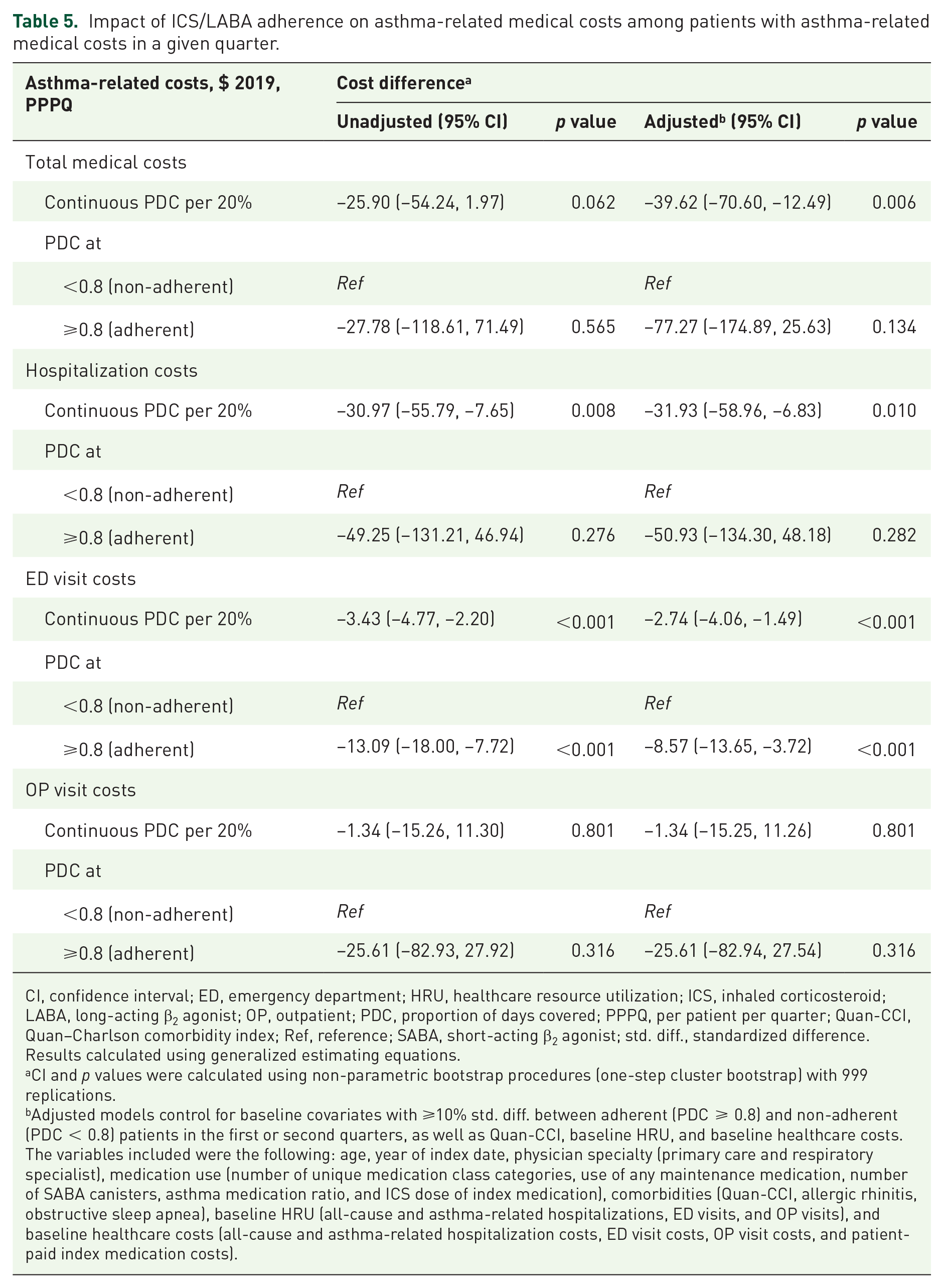
Costs varied widely during follow-up; mean hospitalization costs ranged from $50 to $700, ED visit costs ranged from $15 to $50, and OP visit costs ranged from $200 to $700 per quarter (data not shown). In general, mean total medical costs PPPQ ranged from $300 to $1200. Overall, adherent patients incurred lower costs across most measures (Table 5).
Impact of ICS/LABA adherence on asthma-related medical costs among patients with asthma-related medical costs in a given quarter.
CI, confidence interval; ED, emergency department; HRU, healthcare resource utilization; ICS, inhaled corticosteroid; LABA, long-acting β2 agonist; OP, outpatient; PDC, proportion of days covered; PPPQ, per patient per quarter; Quan-CCI, Quan–Charlson comorbidity index; Ref, reference; SABA, short-acting β2 agonist; std. diff., standardized difference.
Results calculated using generalized estimating equations.
CI and p values were calculated using non-parametric bootstrap procedures (one-step cluster bootstrap) with 999 replications.
Adjusted models control for baseline covariates with ⩾10% std. diff. between adherent (PDC ⩾ 0.8) and non-adherent (PDC < 0.8) patients in the first or second quarters, as well as Quan-CCI, baseline HRU, and baseline healthcare costs. The variables included were the following: age, year of index date, physician specialty (primary care and respiratory specialist), medication use (number of unique medication class categories, use of any maintenance medication, number of SABA canisters, asthma medication ratio, and ICS dose of index medication), comorbidities (Quan-CCI, allergic rhinitis, obstructive sleep apnea), baseline HRU (all-cause and asthma-related hospitalizations, ED visits, and OP visits), and baseline healthcare costs (all-cause and asthma-related hospitalization costs, ED visit costs, OP visit costs, and patient-paid index medication costs).
After controlling for differences in baseline characteristics, total medical costs PPPQ were $39.62 lower per 20% increase in PDC (95% CI: –$70.60, –$12.49; p = 0.006) and hospitalization costs were $31.93 lower per 20% increase in PDC (95% CI: –$58.96, –$6.83; p = 0.010). Costs were non-significantly different between adherent and non-adherent patients for total medical costs (adjusted cost difference [95% CI]: –$77.27 [–$174.89, $25.63]; p = 0.134) and hospitalization costs (adjusted cost difference [95% CI]: –$50.93 [–$134.30, $48.18]; p = 0.282). ED visit costs were significantly lower per 20% increase in PDC (adjusted cost difference [95% CI]: –$2.74 [–$4.06, –$1.49]; p < 0.001) and were significantly lower for adherent versus non-adherent patients (adjusted cost difference [95% CI]: –$8.57 [–$13.65, –$3.72]; p < 0.001). OP visit costs were not significantly different between adherent and non-adherent patients (adjusted cost difference [CI]: –$25.61 [–$82.94, $27.54]; p = 0.316). Of note, after excluding all quarters with zero asthma-related total medical costs, some of the remaining quarters still had zero costs for the individual medical cost components (ie, hospitalizations, ED visit, and OP visit costs).
Discussion
We evaluated the impact of adherence to ICS/LABA medication on asthma-related outcomes using real-world claims data from adult patients with asthma in the United States. In general, findings from this study showed that adherent patients (PDC ⩾ 0.8) experienced better clinical and economic outcomes than non-adherent patients. After adjustment for baseline characteristics, adherent patients experienced significantly fewer severe exacerbations compared to non-adherent patients. Furthermore, with the exception of OP visits, adherent patients had lower asthma-related HRU and incurred lower costs in quarters with asthma-related resource use.
In line with our results, previous studies have suggested that increased adherence to asthma medication reduces the likelihood of asthma-related exacerbations.12,13,16,17 Furthermore, a recent meta-analysis found that ⩾80% adherence to maintenance medications lowered the odds of asthma-related severe exacerbation by 47% across eight studies. 18 Delea et al. 12 who used a similar study design to this study, reported a 10% decrease in the odds of asthma-related ED visits or hospitalization per 25% increase in adherence. Those results align with the present study findings of a 4.8% decrease in the odds of severe exacerbation per 20% increase in adherence and 22.2% lower odds of severe exacerbation in adherent versus non-adherent patients. The difference in the magnitude of our results versus those of Delea et al. may be partially attributed to differing methods of assessing adherence. The medication possession ratio (MPR) was used by Delea et al., whereas we used PDC; both are valid adherence measures, but the MPR tends to overestimate adherence while the PDC is more conservative and is recommended by the Pharmacy Quality Alliance for most classes of chronic medications.19,20 In addition, we examined outcomes as a function of 20% increase in adherence, while Delea et al. examined a 25% increase which may also have contributed to the difference in the results. Moreover, the follow-up period in Delea et al.’s 12 study was censored at discontinuation of FP/SAL, whereas the follow-up period of this study was censored at a dispensing of a non-ICS/LABA controller. Censoring at discontinuation could be a limitation since the reason for discontinuation was not known and could lead to overestimations of adherence.
Our findings of reduced odds of SABA and OCS use with increasing adherence also align with the multivariable regression analysis of Delea et al., 12 who reported that for each 25% improvement in medication adherence, the odds of receiving SABA decreased by 10% and the odds of receiving a corticosteroid decreased by 3%, though again the associations observed in this study are smaller in magnitude. Use of SABA and OCS is indicative of poorly controlled asthma17,21 so the reduced use associated with increased ICS/LABA adherence may represent a meaningful improvement in asthma management. Furthermore, adverse events are associated with the use of OCS and these worsen with increasing cumulative dose, 22 suggesting that reducing reliance on OCS via improved medication adherence may reduce the likelihood of associated negative long-term outcomes. Unexpectedly, we found that adherent patients used increased rates of SABA canisters versus non-adherent patients despite adherent patients being less likely to use SABA. Similar findings have been reported previously,17,23 and this again reflects the results of Delea et al., 12 who, while not directly evaluating the association between adherence and rates of SABA dispensings, found in their unadjusted descriptive results an increasing trend of mean SABA dispensings with increased adherence.
Previous studies have highlighted that poorly controlled asthma is associated with an increase in HRU and costs.4,24 We found that increased ICS/LABA adherence was associated with significantly fewer asthma-related hospitalizations and ED visits, suggesting that adherence confers better asthma control. 25 However, adherent patients had significantly more OP visits than non-adherent patients. The relationship between increased adherence and more frequent OP visits has been reported previously 26 and may reflect patients who are more health-conscious and more inclined to visit their physician despite their asthma being well controlled. 27 The diligence of patients regarding their asthma treatment may also relate to the increased rate of SABA canisters observed among adherent patients. Increased OP visits may also indicate that the patients’ physicians followed-up more closely with them, tracking their disease progression and response to treatment, thereby leading to improved adherence and management of symptoms. 28 Furthermore, it has been shown that some asthma patients take maintenance medication on an as-needed basis and may even alter the dose of their medication.29,30 The INSPIRE study investigated the attitudes and actions of patients with asthma using maintenance therapy and found that 66% of patients were more likely to manage their asthma independently rather than seeking help or advice from their physician. 29 In addition, a study investigating patients’ perception of barriers and facilitators to taking long-term controller medication for asthma found that some patients had the perception that their medication should be used in response to symptoms instead of on a regular basis, as prescribed. This perception translated to patients using their inhaler only when symptoms arose followed by discontinuation when symptoms subsided. 30 This may also explain the higher number of OP visits observed among adherent patients as non-adherent patients may be using their inhaler on an as-needed basis and without seeking guidance from their physician.
An important additional consideration related to adherence is the use of once- versus twice-daily dose medication. Both types of treatment were used by patients included in this study, but a potential limitation is that the study population was not stratified by the specific medications used. Previous studies have shown once-daily ICS/LABA treatment regimens to be associated with increased adherence versus twice-daily.31,32 Another recent study using IQVIA PharMetrics Plus data examined the use of once-daily FF/VI versus twice-daily BUD/FOR and reported better symptom control (fewer asthma-related exacerbations and lower SABA use) with FF/VI, supporting improved outcomes with once- versus twice-daily therapy. 32
This study was subject to certain limitations that reflect the nature of using claims databases in observational research. The OP pharmacy claims data used did not allow us to directly measure medication use, nor whether the medication was administered as prescribed; this is a known limitation associated with claims data, as is the possibility of coding inaccuracies. Furthermore, we lacked data regarding the use of over-the-counter, sample, or hospital administered non-parenteral medications. The exclusion of follow-up quarters with zero costs from the cost analysis may have led to an overestimation of non-adherent patients’ costs because non-adherent patients were less likely to have OP visits. However, this method was used as a consequence of the high proportion of zero costs per quarter, which subsequently led to challenges in appropriately modeling and interpreting cost outcomes. By excluding quarters of follow-up with zero costs, the reported cost differences represent the economic impact of adherence when asthma-related resources are used. Another potential limitation of this study is that ICS/LABA as needed therapy cannot be distinguished from non-adherence in the data. If a patient with mild asthma on low-dose ICS/LABA was stepped down to ICS/LABA as needed, and this new regimen involved skipping over 20% of the usually prescribed inhalations, then it would be recorded as non-adherence. However, it is important to note that prescription of ICS/LABA therapy for as-needed use is not approved in the United States and would therefore be for off-label use.
There were several strengths to this study. First, the large claims database used provided a diverse patient sample to assess the clinical and economic burden associated with ICS/LABA adherence among patients with asthma across all US census regions. Second, the database included detailed information on relevant clinical and economic measures as well as demographic characteristics of the patients analyzed. Finally, this study assessed asthma-related outcomes quarterly and examined the association with medication adherence in the previous quarter. Our results, therefore, demonstrate that the effects of adherence on asthma-related outcomes can be seen over a short timeframe. Adherence to medication is variable and tends to decrease over time; by using a series of short follow-up periods, we captured the immediate effects of adherence as opposed to overall effects over a longer period.
Conclusion
Adequate control of asthma remains an essential component in preventing and mitigating exacerbations, which can meaningfully improve a patient’s health-related quality of life and reduce the overall burden of disease. Thus, insight into the impact of adherence on the burden of asthma is important for healthcare stakeholders and can assist in directing future efforts to improve clinical and economic outcomes for patients with asthma.
We have shown that adherence to ICS/LABA medications is associated with reduced asthma-related exacerbations, rescue medication use, and HRU. Through the use of short-term follow-up periods, we also demonstrated that an impact of medication adherence on health outcomes is seen quickly. Adherence was additionally associated with lower ED and other medical costs in quarters with asthma-related HRU. The findings of this real-world study highlight the clinical and economic benefits of medication adherence to ICS/LABAs among patients with asthma, particularly in reducing asthma-related severe exacerbations leading to hospitalization or ED visits, which is critical to optimal asthma management.
Supplemental Material
sj-docx-1-tar-10.1177_17534666221116997 – Supplemental material for Impact of adherence to treatment with inhaled corticosteroids/long-acting β-agonists on asthma outcomes in the United States
Supplemental material, sj-docx-1-tar-10.1177_17534666221116997 for Impact of adherence to treatment with inhaled corticosteroids/long-acting β-agonists on asthma outcomes in the United States by Carlyne M. Averell, François Laliberté, Guillaume Germain, Mei Sheng Duh, Matthew D. Rousculp, Sean D. MacKnight and David J. Slade in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
Medical writing support for the development of this manuscript, under the direction of the authors, was provided by Fraser Shearer, PhD, and Ryan Riley, PhD, of Ashfield MedComms, Glasgow, United Kingdom, an Inzio company, and was funded by GSK plc. Trademarks are owned by or licensed to their respective owners (the GSK group of companies or IQVIA Inc.).
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.