
Abstract
Pleural disease in lung cancer can be benign or malignant with the latter carrying a grave prognosis. In this review, we describe and discuss the advances in pleural imaging, procedures, and biomarkers for the diagnosis of pleural diseases in lung cancer. Ultrasound and computed tomography are increasingly applied in the planning of pleural procedures to enhance diagnostic accuracy and safety whilst pleuroscopy gives excellent yield in excess of 93% in the evaluation of cytology negative pleural effusions. Invasion beyond the elastic layer of the visceral pleura upstages lung cancer, and may indicate a need for adjuvant chemotherapy. Biomarkers isolated from pleural fluid or tissue may aid in diagnosis and guide treatment in the future. Magnetic resonance imaging, positron emission tomography, narrow band imaging of the pleura and autofluorescence thoracoscopy are technologies that require further evaluation to better define their respective roles in the diagnostic algorithms of pleural diseases in lung cancer.
Introduction
Pleural disease in lung cancer can be malignant or benign. In the work up of a patient with lung cancer presenting with pleural effusion, chest X-ray (paired frontal and lateral decubitus views) and contrast-enhanced computed tomography (CT) are performed to confirm the presence of fluid in the pleural cavity, and to evaluate the pleura for nodularity or thickening which might suggest metastasis. Investigators may perform thoracentesis after review of lateral decubitus films or with ultrasonography (US) which further improves the safety of the procedure. Image-guided aspiration of pleural fluid and biopsy of parietal pleura are increasingly performed, however yield from these noninvasive methods is variable as it is dependent on the nature and extent of pleural involvement by lung cancer as well as errors related to sampling. Surgical techniques such as video-assisted thoracoscopy (VATS) or thoracotomy improve sampling accuracy but require general anesthesia and are associated with higher morbidity and mortality. Diagnostic tools for evaluating pleural diseases have made considerable advances in the last decade, so it is opportune to review current technologies in imaging, techniques for acquiring pleural biopsy, and biomarkers (Table 1).
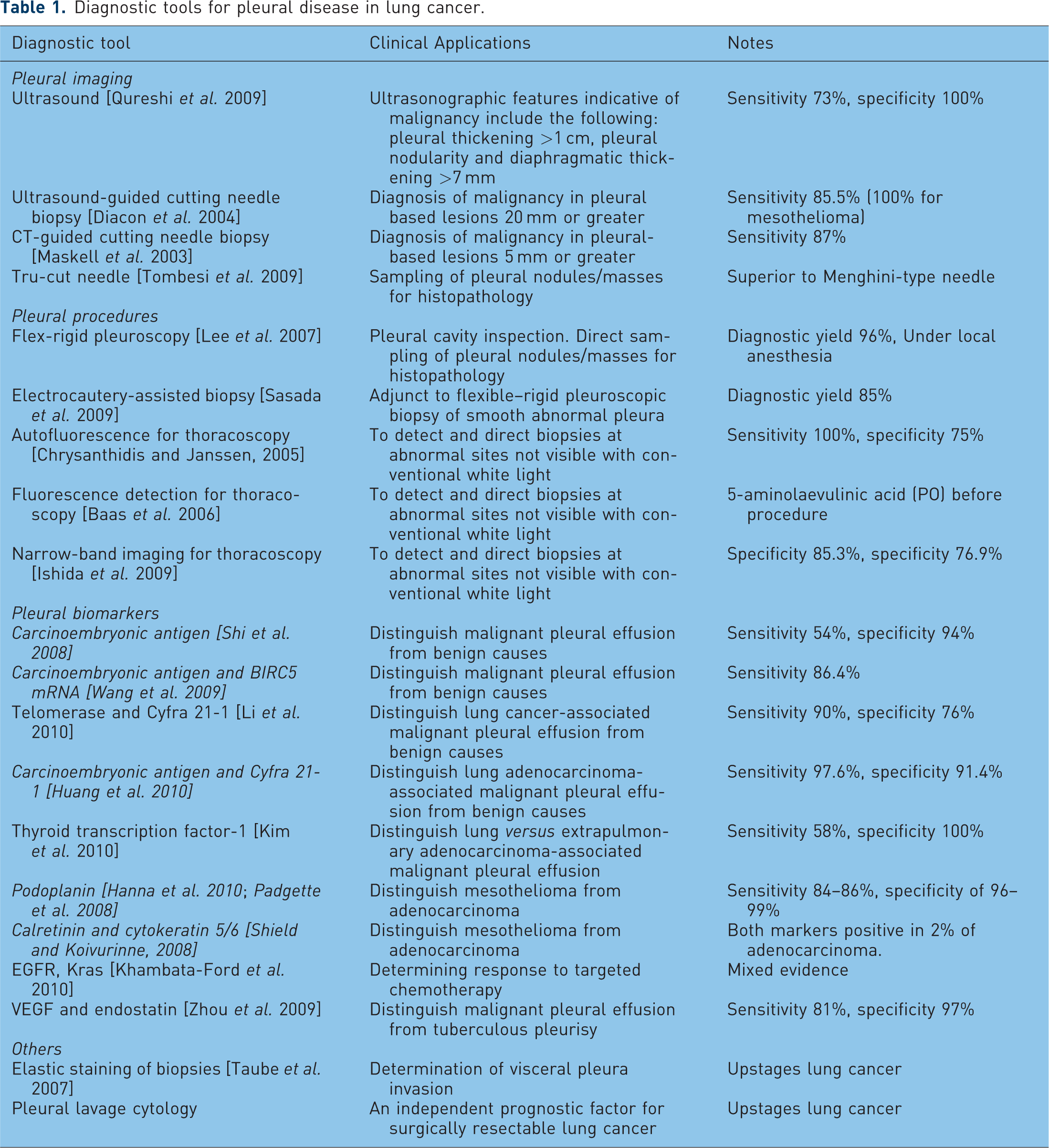
Diagnostic tools for pleural disease in lung cancer.
Visceral pleural invasion
Following resection of lung cancer, careful examination for visceral pleural invasion (VPI) beyond the elastic layer of the visceral pleura should be carried out [Travis et al. 2008] as VPI is considered an important stage-defining feature for lung cancer in the absence of nodal involvement. VPI can result in either stage IB or IIA depending on tumor size, and may indicate a need for adjuvant chemotherapy for stage IIA and select stage IB if the primary tumor measures greater than 4 cm in size [Shim et al. 2009; Yoshida et al. 2009]. Elastin staining should therefore be routine for all specimens [Taube et al. 2007]. Metastatic spread of lung cancer to the pleura adversely affects survival: in the new TNM staging of lung cancer the presence of pleural metastasis is now defined as M1a (from T4) with a corresponding change in stage from stage IIIB to stage IV [Rami-Porta et al. 2009].
Advances in pleural imaging and pleural biopsy
Standard CT for staging of lung cancer should include the chest, liver and adrenals. Contrast-enhanced CT is preferred to evaluate the pleura and features such as nodularity, irregularity and pleural thickness greater than 1 cm are highly suggestive of malignancy [Traill et al. 2001; Leung et al. 1990]. Magnetic resonance imaging (MRI) is superior to CT in delineating soft tissue and vascular planes, and is especially useful in evaluating the surgical resectability of superior sulcus tumors [Webb et al. 1991; Heelan et al. 1989]. If accurate assessment of chest wall invasion is required, dynamic contrast-enhanced MRI can be performed [Kajiwara et al. 2010]. Dynamic contrast-enhanced MRI has also facilitated discrimination of rounded atelectasis (benign pleural infolding) from peripheral pulmonary nodule [Horn et al. 2010], and epithelioid mesothelioma from sarcomatioid and biphasic subtypes by registering higher diffusion coefficient values [Gill et al. 2010].
Positron emission computed tomography (PET) is a functional diagnostic imaging technique. F-18 fluoro-2-deoxy-D-glucose (FDG), an analog of glucose, is the most commonly used radiotracer in PET imaging. The F-18 FDG uptake in tumor cells is directly proportional to glucose metabolism in the cells, and since glucose metabolism is increased several folds in the malignant tumors, PET images show preferential higher FDG uptake in malignant cells as compared with normal cells. The addition of CT to PET has led to better specificity and sensitivity than either modality alone as combined PET-CT demonstrates both functional and structural details. PET-CT is widely used in lung cancer because of its superiority over other imaging techniques in staging nodal and metastatic disease, for recurrent disease and monitoring therapy response [Fischer et al. 2010; Kligerman and Digumarthy, 2009; Shim et al. 2006]. In the evaluation of the pleura, PET-CT is preferred although conditions such as infection, inflammation or prior talc pleurodesis can give false-positive results. PET-CT is also useful for detecting malignancy in symptomatic patients with pre-existing benign pleural pathologies. A pilot study of 12 patients with lymphangio-leiomyomatosis, no FDG uptake was observed by benign pleural lesions compared with avid uptake by malignant ones [Young et al. 2009].
Imaging of the pleura can be easily performed at the patient’s bedside using US. US is increasingly applied as a safety adjunct to guide pleural procedures in selecting appropriate sites for thoracentesis, tube thoracostomy, and thoracoscopy [Hersh et al. 2003]. Certain US features such as pleural thickening >10 mm, pleural nodularity and diaphragmatic thickening >7 mm are diagnostic of malignancy with 73% sensitivity and 100% specificity [Qureshi et al. 2009]. An ‘echogenic swirling pattern’ characterized by numerous free-floating echogenic particles swirling in the pleural cavity during respiratory movement or heartbeat is also reported as another sign indicative of malignant pleural effusion [Chian et al. 2004]. Contrast-enhanced sonography was investigated in a group of patients with pleural-based pulmonary lesions where aqueous suspension of stabilized AF6 microbubbles (SonoVue®, Bracco Diagnostics Inc, UK) was administered intravenously. Time to, extent of, and homogeneity of enhancement did not differ between benign and malignant pleural-based lesions although all cases of compression atelectasis and 62% pneumonia demonstrated rapid time to and marked enhancement. Delayed time to and reduced enhancement were noted in all patients with pulmonary embolism and 62 % peripheral malignant lesions [Gorg et al. 2006]. Notwithstanding that these US features may predict pleural metastasis, histology is still the gold standard, and where thoracoscopy is not readily available, image-guided pleural biopsy represents a good alternative.
A randomized trial comparing CT-guided needle biopsy with Abram’s needle biopsy of parietal pleura measuring >5 mm (Figure 1) showed that CT-guided needle biopsy achieved 87% yield for malignancy compared with 47% with the Abram’s needle [Maskell et al. 2003]. Diacon and coworkers also achieved an impressive yield of 85.5% when they applied US instead of CT to biopsy pleural lesions measuring 20 mm and more using the 14 gauge cutting needle; yield for malignant mesothelioma was 100% and the rate of pneumothorax was 4% [Diacon et al. 2004].

Pleural nodularity due to metastases.
The type of needle appears to be important in assuring good yield for transthoracic biopsy. In a randomized trial consisting of 307 patients with pleural-based lung lesions that were biopsied under US guidance, the Tru-cut needle achieved 95.4% diagnosis compared with 85.8% using the modified Menghini (aspiration/suction) needle [Tombesi et al. 2009]. In another recent study, the Abram’s needle was found to be better for sampling of the parietal pleura than the Tru-cut needle in suspected tuberculous pleural effusions [Koegelenberg et al. 2010].
Advances in evaluation of pleural space
Thoracoscopy allows the physician a view into the pleural space, visually guided biopsy of abnormal parietal pleura, chest tube placement and pleurodesis. A major advance in thoracoscopy is the introduction of the flex–rigid pleuroscope (model LTF 160/240, Olympus, Japan) that is fashioned in the same way as a flexible bronchoscope (Figure 2). The flex–rigid pleuroscope consists of a handle, and a shaft that measures 7 mm in outer diameter and 27 cm in length. The shaft consists of 22-cm proximal rigid portion and 5-cm flexible distal end. The flexible tip is movable by a lever on the handle which allows two-way angulation 160° up and 130° down. It consists of a 2.8-mm working channel that accommodates biopsy forceps, needles and other accessories, and is compatible with various electrosurgical and laser procedures (Figure 2). The LTF 160 model also allows autoclaving [Munavvar et al. 2007]. A notable advantage of the flex–rigid pleuroscope over rigid instruments is its easy interface with existing processors (CV-160, CLV-U40) and light sources (CV-240, EVIS-100 or 140, EVIS EXERA-145 or 160) made by the manufacturer for flexible bronchoscopy or gastrointestinal endoscopy which are available in most endoscopy units at no additional costs [Lee and Colt, 2005].

Flex–rigid pleuroscope.
Pleuroscopy can be performed safely in the bronchoscopy suite with the patient under local anesthesia and conscious sedation and represents a good alternative to VATS, which requires general anesthesia and single lung ventilation [Lee et al. 2010]. Flex–rigid pleuroscopy is not only well tolerated by patients requiring low doses of midazolam and opioids, importantly it is an excellent tool for staging lung cancer patients with cytology negative pleural effusions or in the diagnostic evaluation of pleural effusions of unclear etiology where repeated thoracentesis and needle biopsy fail [Lee et al. 2007; Munavvar et al. 2007]. A major factor that affects diagnostic yield is when encountering smooth and thickened pleura or if mesothelioma is suspected. This is because the flexible forceps lacks mechanical strength necessary for obtaining representative pleural specimens of sufficient depth. In these situations, electrocautery using the insulated tip (IT) diathermic knife can be incorporated where full thickness parietal pleural biopsies are obtained using the IT knife via the working channel of the flex–rigid pleuroscope. Yield with the IT knife (85%) is superior over 60% with the flexible forceps [Sasada et al. 2009].
Autofluorescence video thoracoscopy may accentuate the appearance of malignant pleural deposits by inducing color change. Lesions that appear white or pink on white light thoracoscopy become red under green light. Autofluorescence thoracoscopy has high sensitivity 100% but lower specificity 75% [Chrysanthidis and Janssen, 2005]. In another study, oral ingestion of 1.5–2.5 g aminolaevulinic acid (5-ALA) 3–4 hours before thoracoscopy appears to improve detection of malignant mesothelioma not visible on conventional white light thereby facilitating biopsy [Baas et al. 2006]. Similarly narrow band imaging (NBI), a technology built into the flexi–rigid pleuroscope that uses an optical filter to emit discrete bands of blue and green light, highlights mucosal structures and vessels (Figure 3). Abnormal vascular patterns such as blood vessels with irregular caliber or punctate vessels associated with malignancy are more easily identified with NBI than white light, and may be useful in selecting biopsy sites [Ishida et al. 2009].

White light pleuroscopy and narrow-band imaging (NBI) showing abnormal vascular pattern due to malignant mesothelioma.
Advances in pleural biomarkers
Distinguishing malignant versus benign pleural effusions
Pleural fluid cytology for the diagnosis of malignant effusion gives an average yield of 60% with repeated [Hooper et al. 2010] and large volume thoracenteses (>50 ml) [Abouzgheib et al. 2009]. Biomarkers in the pleural fluid are investigated in an attempt to improve its sensitivity. In a systematic review, carcinoembryonic antigen (CEA) is found to confer good specificity 94% but poor sensitivity 54% for the diagnosis of malignant pleural effusion [Shi et al. 2008], and some investigators have combined various biomarkers to improve test accuracy. Forty-one patients with histology proven malignant pleural effusion due to lung adenocarcinoma, and 93 patients with benign pleural effusions were evaluated. Pleural fluid CEA (>6.0 µm/l) combined with cytokeratin fragment (Cyfra) 21-1 (> 60 µm/l) resulted in 97.6% sensitivity and 91.4% specificity for malignancy [Huang et al. 2010]. In another study of 80 patients with malignant pleural effusions due to lung cancer, and 50 patients with benign pleural effusions, pleural fluid Cyfra 21-1 combined with telomerase yielded 90% sensitivity, 76% specificity and an overall 86.9% accuracy for malignancy [Li et al. 2010]. Others had also investigated CEA and BIRC5 mRNA expression in the pleural fluid of patients with malignant effusions [Wang et al. 2009] and although results appeared encouraging, they required validation in larger studies.
In areas of high tuberculosis prevalence, the finding of lymphocyte-rich pleural effusion may be due to tuberculous pleurisy or malignancy. Both diagnoses may be elusive since tuberculous pleurisy is pauci-bacillary and Ziehl–Neelsen smear negative whilst pleural malignancy can be cytologically negative. Since vascular endothelial growth factor (VEGF) and endostatin levels are both elevated in malignant pleural effusion, VEGF combined with endostatin at respective cut-off values 1.60 ng/ml and 4.00 ng/ml, respectively, can differentiate malignancy from tuberculous pleurisy with good sensitivity and specificity [Zhou et al. 2009].
Pulmonary versus extrapulmonary adenocarcinoma
Immunohistochemical markers especially thyroid transcription factor-1 (TTF-1) can aid in discriminating malignant pleural effusions from lung cancer versus extrapulmonary sites [Pu et al. 2008a, 2008b] since staining positive for thyroid transcription factor-1 (TTF-1) is 100% specific for lung adenocarcinoma [Kim et al. 2010]. Similarly diagnosing malignant mesothelioma in serosal effusions continues to be a major challenge because some of its cytomorphological features closely resemble lung adenocarcinomas and immunohistochemistry is a valuable tool. Immunostaining for calretinin and cytokeratin 5/6 from cell block preparations of pleural fluid can be helpful as positive staining for calretinin and cytokeratin 5/6, respectively, was present in 97% of mesothelioma cases compared with 3% and 6% of lung adenocarcinomas. In fact no cases of mesothelioma were negative for both calretinin and cytokeratin 5/6 [Shield and Koivurinne, 2008]. Recently podoplanin is recognized as a positive marker for mesothelioma [Padgett et al. 2008; Chu et al. 2005]. Hanna and coworkers evaluated paraffin-embedded cell blocks of 86 pleural effusions where slides prepared from these cell blocks were stained for podoplanin. They found that podoplanin was expressed in 94% of malignant mesothelioma cases (17/18) and 0% of lung adenocarcinoma cases. All positive cases of malignant mesothelioma demonstrated strong membranous reactivity to podoplanin, which in combination with calretinin could be more specific than CK5/6 in differentiating epithelioid malignant mesothelioma from adenocarcinoma of the lung [Hanna et al. 2010].
Prognostication and guiding chemotherapy for malignant pleural effusions
Although the general prognosis of malignant effusions is poor, certain biomarkers and mediators measured in pleural fluid have demonstrated worse outcome and these include VEGF levels >1350 ng/ml [Hsu et al. 2009], high quantities of tumor markers (CEA, CA 15-3, Cyfra 21-1, CA 125) [Bielsa et al. 2009], and increased expression of triggering receptor expressed on myeloid cells (TREM)-1 [Ho et al. 2008]. Several investigators have proposed the use of pleural biomarkers to guide choice of chemotherapy but current evidence is lacking due to conflicting results. Soh and coworkers reported that epidermal growth factor receptor (EGFR) mutations detected in malignant effusions were associated with better clinical response and survival in gefitinib-treated patients [Soh et al. 2006]. In another phase III trial, the converse was true where EGFR mutations assayed by direct sequencing, EGFR protein expression by immunohistochemistry, and EGFR gene copy number by fluorescent in situ hybridization from formalin-fixed, paraffin-embedded tissues of patients with advanced lung cancer did not impact survival nor predict response to cetuximab (EGFR antibody) [Khambata-Ford et al. 2010].
Future
Pleural lavage cytology
Malignant cells detected in the pleural lavage performed at the time of resection for lung cancer may be an important prognostic factor. Several studies have demonstrated association of positive pleural lavage with distant metastases and high rate of pleural recurrence [Satoh et al. 2007]. In a meta-analysis of 8763 patients where 5.8% had positive pleural lavage for malignant cells at the time of surgery, survival outcome of these patients was similar to individuals with one T-stage higher [Lim et al. 2010]. Aokage and co-workers also evaluated the impact of intraoperative pleural lavage on the survival outcome and recurrence in 2178 patients with surgically resectable lung cancer. In addition, they compared pre- and post-lung-cancer-resection pleural lavages which were performed in all patients. They reported that post-lung-resection pleural lavage was a strong predictor of cancer recurrence, and individuals with positive post–lung-resection pleural lavage had marginally better survival over their counterparts with malignant pleural effusions regardless of tumor size [Aokage et al. 2010; Shintani et al. 2009; Taniguchi et al. 2009; Enatsu et al. 2006]. In the cytology-negative pleural lavage, telomerase measurement by means of enzyme linked immunosorbent assay could further improve its sensitivity for detection of pleural micrometastasis. In the study by Li and coworkers, telomerase activity, positive pleural lavage cytology and pathologic TNM staging were significant independent prognostic determinants [Li et al. 2009].
Conclusion
Current British Thoracic Society guidelines recommend US to guide pleural procedures as well as early pleuroscopy for the evaluation of patients with cytology negative effusions [Havelock et al. 2010; Hooper et al. 2010; Rahman et al. 2010; Roberts et al. 2010]. In lung cancer patients with poor performance status and suspected with pleural metastasis, image-guided biopsy of pleural nodularity using the cutting needle is a good alternative [Hooper et al. 2010]. It is proposed as the standard of care for pathologists to examine the visceral pleura for tumor invasion, and the addition of intra-operative pleural lavage is emerging as an essential step towards enhancing lung cancer staging and prognostication. The future spells interest in sensitive technologies and techniques for imaging the pleura such as MRI, PET-CT, autofluorescence thoracoscopy and NBI as well as novel biomarkers which can translate to improved clinical diagnostic and staging accuracy. Strategies incorporating biomarkers combined with Bayesian statistics [Westfall et al. 2010] or clinical characteristics [Sales et al. 2009] are being developed to improve biomarker specificity in the diagnosis of malignant pleural effusions [Huang et al. 2010; Li et al. 2010; Pu et al. 2008a, 2008b], and validation studies are eagerly awaited before recommendation for use in diagnostic algorithms of pleural diseases.
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
None declared.