
Abstract
The aim of this study is to describe the prevalence of single single-nucleotide polymorphisms (SNPs) as well as their combinations in genes encoding proteins involved in the immune response in children with bacterial meningitis. The prospective study group consisted of 39 children with bacterial meningitis and 49 family members surveyed between 2012 and 2016. Eleven SNPs in seven genes involved in immune response were analysed. The mean number of minor frequency alleles (MAF) of studied SNPs was lowest in the control group and highest in patients with pneumococcal meningitis. We found that carrying ≥6 MAF of studied SNPs was associated with an increased risk of pneumococcal meningitis. The prevalence of risky variants was noted to be higher in patients with pneumococcal meningitis as compared to the control group. In conclusion, genetic factors are a relevant factor in determining the susceptibility to bacterial meningitis. A statistically significant cumulative effect of mutated variants on increasing the risk of bacterial meningitis was detected. Combining all three SNPs in MBL2 improves the prediction of susceptibility to pneumococcal meningitis. Analysis of risky alleles can help indicate people prone to the disease who are ‘gene-immunocompromised’.
Introduction
Streptococcus pneumoniae and Neisseria meningitidis are two of the main bacterial pathogens responsible for meningitis in children.1–4 Colonisation with S. pneumoniae is common in the general population and reaches up to 50% in pre-school children, while N. meningitidis is detected in nasopharyngeal swabs only in around 10% of the general population.3,5 Prevalence of bacterial meningitis in children aged 1 mo to 2 yr is estimated to occur in 20 per 100,000 cases.2,3 A clinically important question is why some patients develop devastating infections, while others become only asymptomatic carriers. In the general population, it is difficult to find one defined risk factor affecting the susceptibility to an invasive bacterial disease. Analysis of one single-nucleotide polymorphism (SNP) does not give an answer to this question. Keeping in mind the complexity of the immune system, in our study we have analysed 11 SNPs in seven different genes involved in the immune response.
The complement pathway represents an important part of innate immunity. It is widely known that complement factor C5–C9 deficiency predisposes to invasive bacterial diseases.6–8 Complement factor H-related protein (CFHR) is responsible for the down-regulation of complement activation. Polymorphisms in CFH are independently associated with predisposition to meningococcal disease. 9 Individuals with SNPs in the CFH region, leading to higher factor H levels, are more prone to invasive meningococcal disease.9,10 Mannose-binding lectin (MBL) is an opsonin which recognises pathogen polysaccharides, and activates an additional (lectin) complement pathway.11–13
The polymorphisms in the MBL gene are attributed to an increased susceptibility to pneumococcal and meningococcal infections.12–14 Three polymorphisms in the MBL2 gene have structural variants resulting in lowered levels of MBL. 14 MBL deficiency leads to reduced opsonisation in the early phase of infection, inducing longer initial survival of S. pneumoniae, thus enhancing the possibility of invasion and subsequent bacterial meningitis. 14
TLRs belong to PRRs, which are crucial for initiating the immune response. SNPs in the TLR2 gene has a substantial effect on the susceptibility to and severity of invasive bacterial infections.15,16 Mutated variants of TLR4 result in hyporesponsiveness to LPS and thus enhance the susceptibility to invasive meningococcal and pneumococcal infections.14–16 Toll-interleukin 1 receptor domain containing adaptor protein (TIRAP) is a protein which binds to the intracellular domain of TLR2 and TLR4, and initiates the MyD88-dependent response leading to TNF-α, IL-12 and other cytokine production.17,18 Khor et al. showed a protective effect of the heterozygotic variant of the TIRAP gene against pneumococcal infection, bacteraemia, malaria and tuberculosis.18,19
This study aims to describe the prevalence of single SNPs, as well as the combinations of SNPs in genes coding proteins involved in the immune response in children with bacterial meningitis.
Patients and methods
Our prospective study group consisted of 39 children with bacterial meningitis. All children were hospitalised at the St. Joseph Children’s Hospital in Poznań, Poland. It is one of the two infectious disease departments serving the population of children of the Greater Poland Voivodeship. We collected blood samples from all of the patients hospitalised with meningitis, which was caused by either S. pneumoniae or N. meningitides, from 2012 to 2016. The bacterial aetiology was confirmed either by a cerebrospinal fluid microbiological culture or an identification of the pathogen’s DNA using PCR. All children were previously healthy and not diagnosed with any immunodeficiencies. All group individuals were vaccinated according to the Polish vaccination schedule – which did not include pneumococcal and meningococcal vaccines. Clinical data were collected from patients’ medical records.
The control group consisted of 49 healthy family members, with no history of meningitis during childhood. We collected data from 32 different families. In seven patients, we were unable to collect material from their family members, due to parental refusal to give blood, and/or the absence of parents during hospitalisation.
We have evaluated 11 SNPs in seven genes that are involved in the inflammatory response. The number of minor frequency alleles (MAF) of studied SNPs was determined for the studied individuals. Alleles with a higher prevalence in patients than in healthy controls were called ‘risky alleles’. Synergism between the SNPs was investigated to identify possible combinations of alleles that could affect the occurrence of the disease. Data on the frequency of the SNPs in the Caucasian population were taken from the 1000 Genomes Project (http://www.ensembl.org). 20
DNA extraction
Genomic DNA was extracted from 1.2 ml of peripheral blood according to the manufacturer’s specifications, and using a Gentra Puregene Blood Kit (Qiagen, Germany). The quality and quantity of isolated DNA was assessed spectrophotometrically. The venipuncture was performed using a standard procedure commonly used for routine blood tests.
SNP genotyping
The PCR was performed in 25 µl of a reaction mixture containing 2 µl of isolated DNA, 10 pmol of each primer, 4 nmol of each deoxynucleotide, 1.5 U of Taq DNA Polymerase (Sigma-Aldrich, USA), 1 × PCR reaction buffer (containing 15 mM MgCl2; Sigma-Aldrich, USA) and additionally 25 mmol MgCl2. PCR products were further purified with thermosensitive Exonuclease I and FastAP Alkaline Phosphatase (Fermentas, Thermo Fisher Scientific, USA) and sequenced with BigDye® Terminator v3.1 Cycle Sequencing Kit on an ABI Prism 3130XL Analyzer (Applied Biosystems, Foster City, CA, USA) according to the manufacturers’ protocols.
The sequences were compared between cases and healthy family members and the general population separately for N. meningitidis and S. pneumoniae cases.
The study was performed with the approval of the Poznan Medical University Ethical Committee and a written informed consent was obtained from all of the parents.
Statistics
Statistical association between disease status and cluster membership was performed to identify genes associated with bacterial meningitis. Hardy–Weinberg analysis was used to check the genotype distribution in patients and in the control group. In this analysis the χ 2 test and software available on the website: https://ihg.gsf.de/cgi-bin/hw/hwa1.pl have been applied. Haploview v4.2 software was used for linkage disequilibrium (LD) analysis. Comparisons between groups were performed using the Pearson χ 2 test of the Fisher exact test as appropriate, and odds ratio (OR) and 95% confidence intervals (95% CIs) were calculated. The Bonferroni correction was applied in the case of analysis of the effect of multiple alleles. All calculations were performed using GraphPad Prism software v6.04. Differences were considered statistically significant when P < 0.05. The Bonferroni correction was applied in the case of analysis of the effect of multiple alleles.
Results
Single allele analysis
Genotype distribution in patients with meningitis, family members and general population.
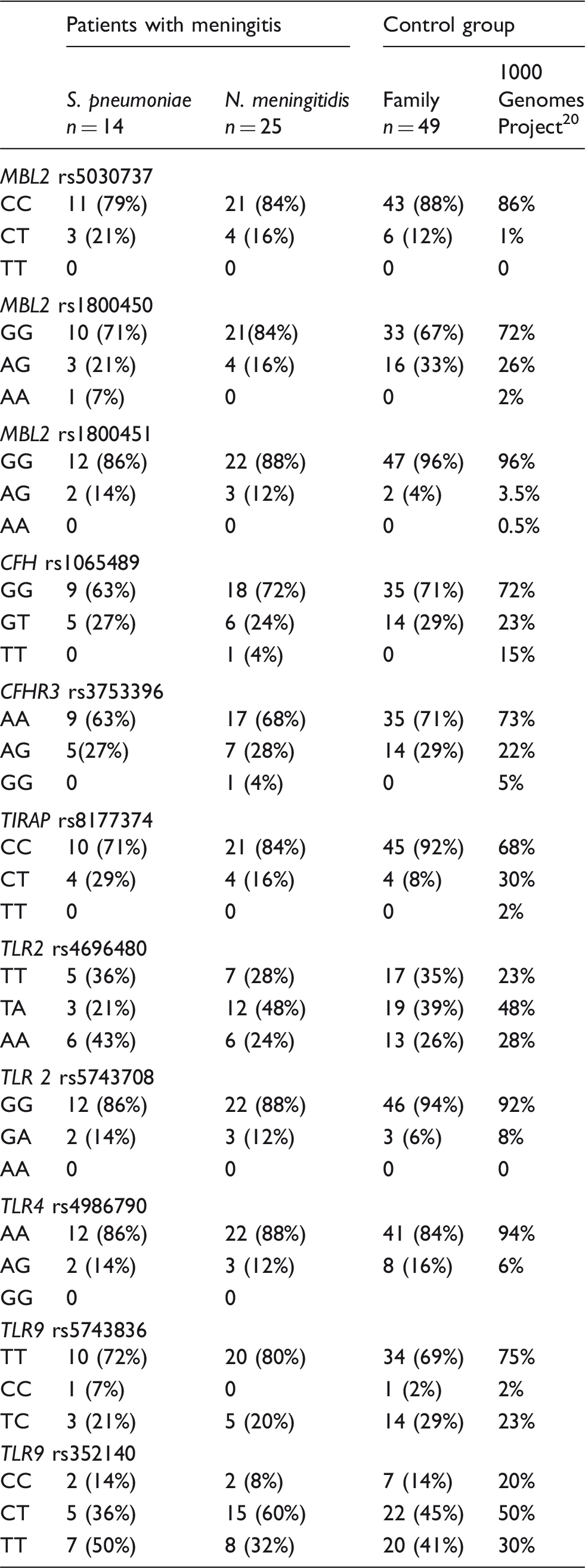
CFH: complement factor H-related protein; MLB: mannose-binding lectin; TIRAP: Toll-interleukin 1 receptor domain containing adaptor protein.
Distribution of MBL genotypes.
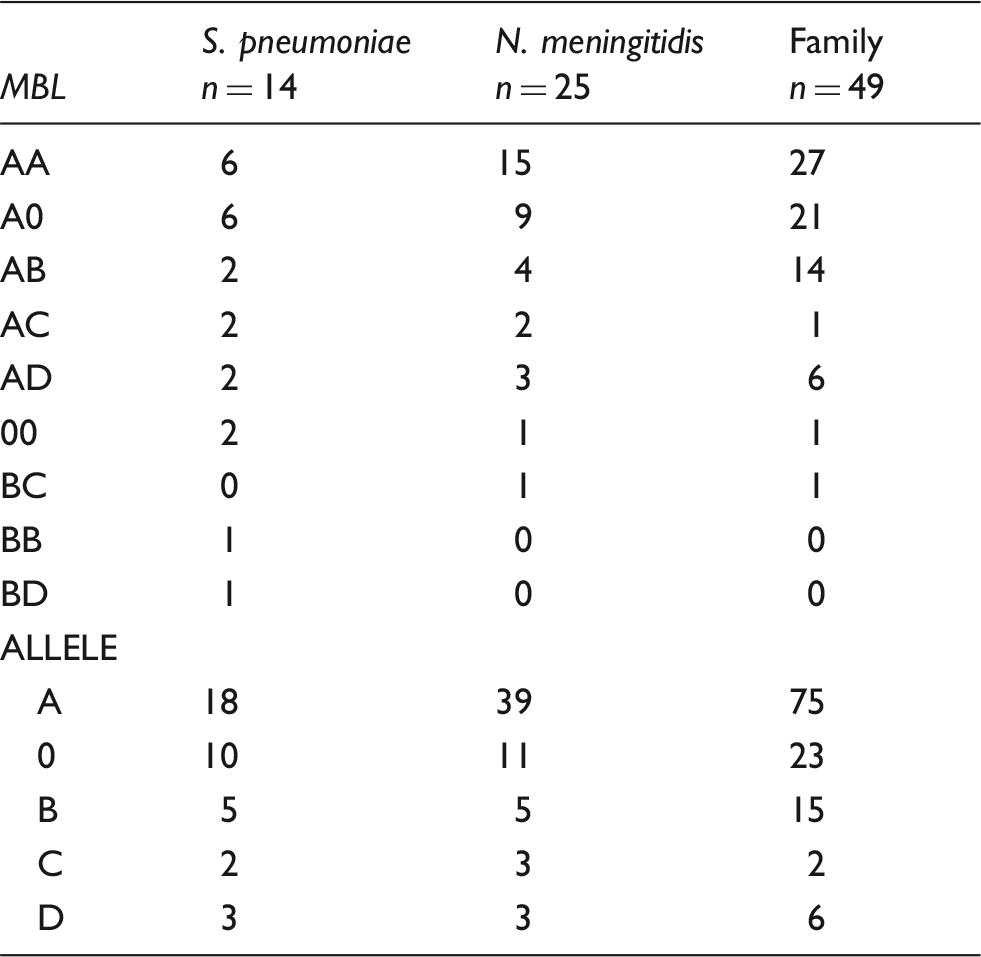
AA: wild type; A0: heterozygotes; 00: homozygotes. Allele: A: wild type; 0: mutated variant of MBL2; rs1800450 variant B, rs1800451 variant C, rs5030737 variant D. MLB: mannose-binding lectin.
Comparison of allele frequency between patients with pneumococcal meningitis and family members.
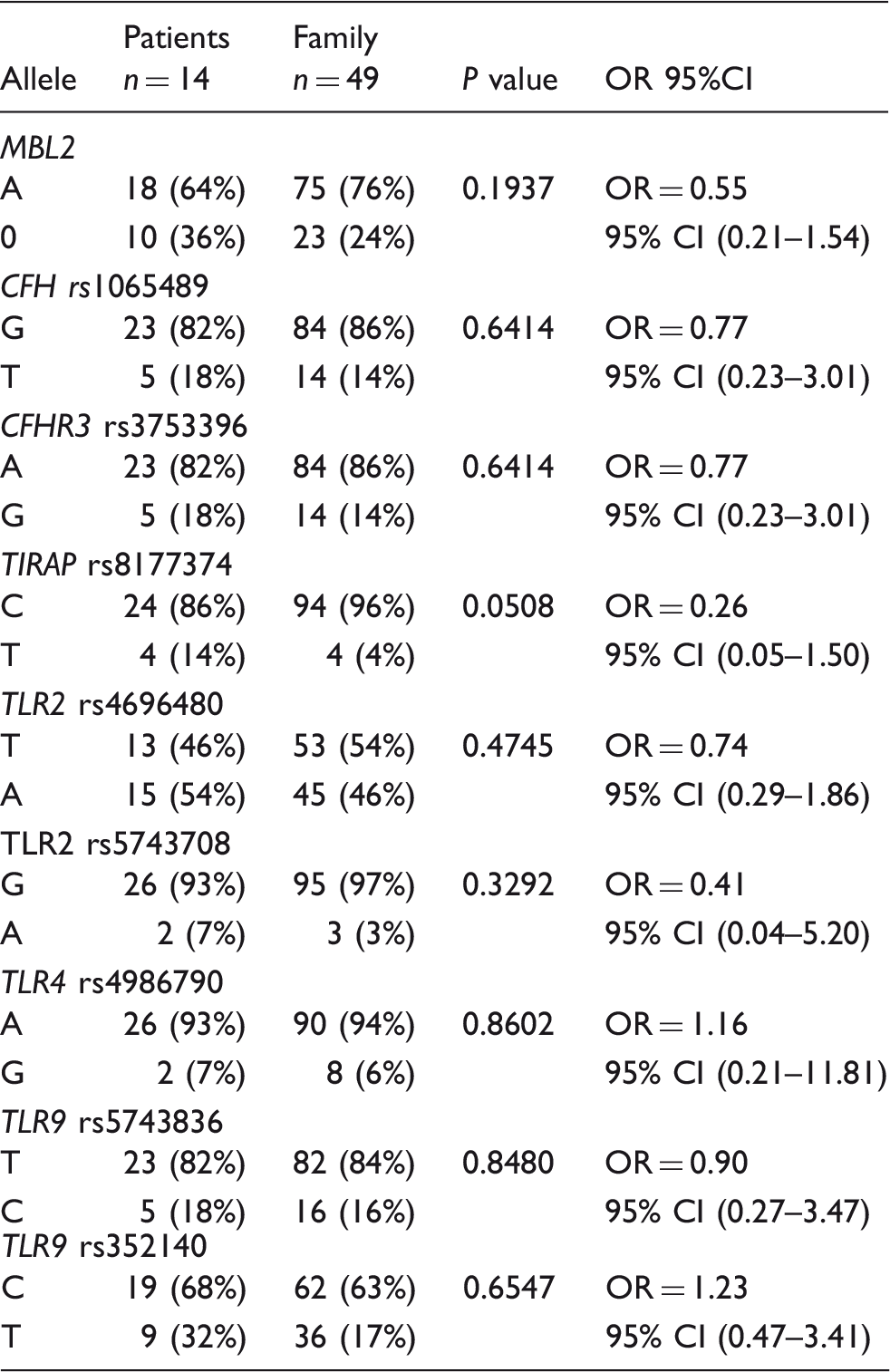
CFH: complement factor H-related protein; MLB: mannose-binding lectin; TIRAP: Toll-interleukin 1 receptor domain containing adaptor protein; OR: odds ratio; 95% CI: 95% confidence interval.
Comparison of allele frequency between patients with meningococcal meningitis and family members.
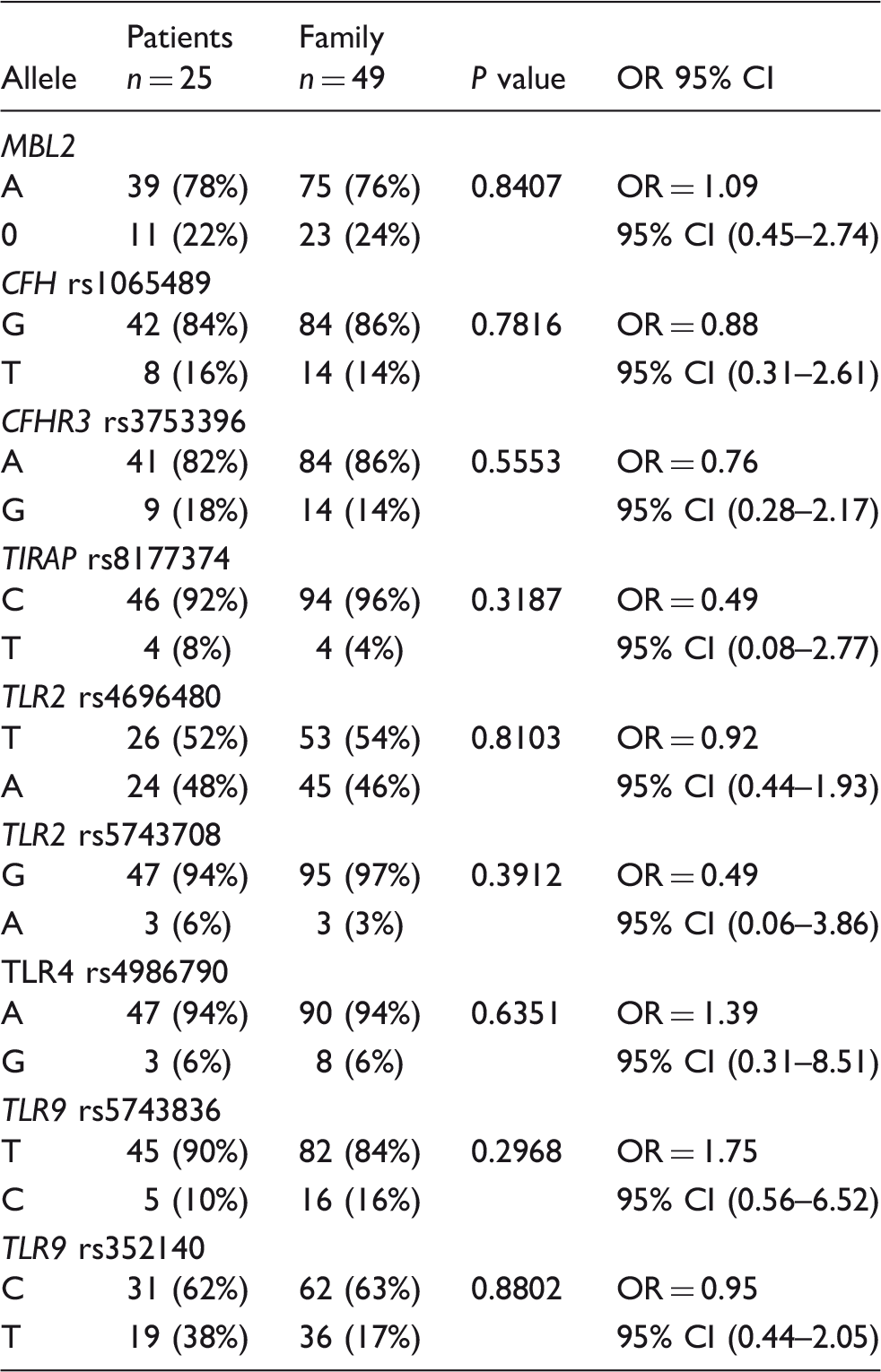
CFH: complement factor H-related protein; MLB: mannose-binding lectin; TIRAP: Toll-interleukin 1 receptor domain containing adaptor protein; OR: odds ratio; 95% CI: 95% confidence interval.
In analysis of a single SNP, we observed that the TIRAP rs8177374 T allele was associated with pneumococcal meningitis at the level of statistical tendency (P = 0.0508).
Cumulative effect of studied polymorphisms
Cumulative effect of 11 studied polymorphisms.
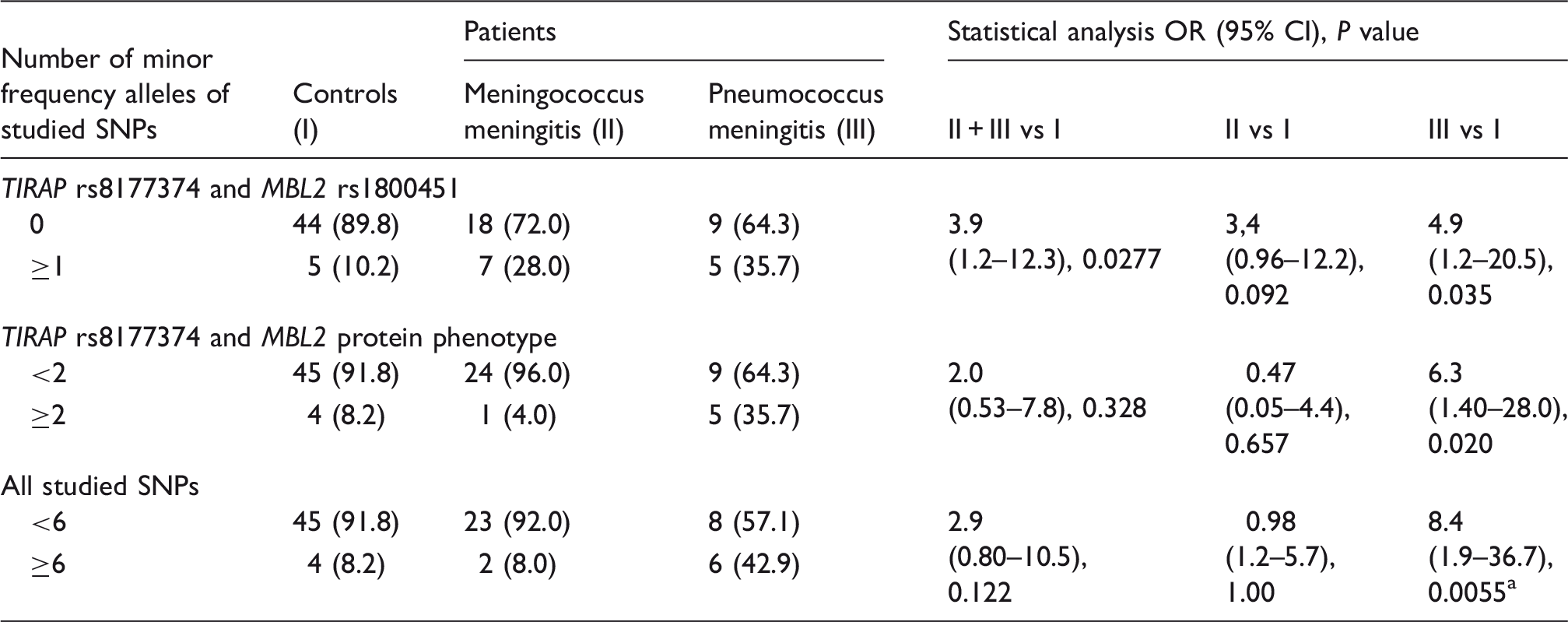
Bonferroni correction for the number of studied genes, P = 0.049. CFH: complement factor H-related protein; MLB: mannose-binding lectin; SNPs: single-nucleotide polymorphisms; TIRAP: Toll-interleukin 1 receptor domain containing adaptor protein; OR: odds ratio; 95% CI: 95% confidence interval.
The mean number of MAF of the studied SNPs was lowest in the control group (family members) (3.35 ± 1.64), intermediate in patients with meningococcal meningitis (3.44 ± 1.66) and highest in patients with pneumococcal meningitis (4.07 ± 2.13). Carrying ≥ 6 MAF of the studied SNPs was associated with an increased risk of developing pneumococcal meningitis (OR 8.4 (95% CI 1.9–36.7); P = 0.0055); Table 5; Supplementary Table a). This result was also statistically significant after an adjustment for the number of studied genes (P = 0.049).
Haplotype analysis
The genotyping of both TLR9 SNPs allows all four rs352140–rs5743836 haplotypes to be distinguished: T-T (0.498), C-T (0.354), T-C (0.138), and C-C (0.010). Because of the small sample size and relatively rare frequency of the rs5743708 SNP, only the three common TLR2 rs5743708-rs4696480 haplotypes were observed in the studied population: T-G (0.477), A-G (0.477), and T-A (0.045). For both genes we observed high values of D’ (0.817 and 1.00, respectively), but relatively low values of r2 (0.066 and 0.043, respectively), which is another measure of LD. Thus, we might therefore conclude that both variants should be tested in an analysis of susceptibility.
Discussion
Our analysis showed a cumulative effect of SNPs in genes involved in the immune response in increasing the risk of meningitis in children. In order to assess the risk of developing meningitis, it is essential to analyse SNPs in several genes involved in the immune response, for example, complement pathway and pattern-recognition particles, because the cumulative effect of SNPs is of clinical importance. Although risky alleles of the examined SNPs were more prevalent in patients compared to controls, the difference was not statistically significant, but carrying more than six MAF of any of the examined SNPs increased the risk of meningitis. This effect was not previously described in the literature. It can be explained by the interactions and complexity of the immune response. We were able to test such associations because in contrast to many other studies, our control group was composed of family members. We could check the SNPs profile in any member of the control group, not only prevalence of the single MAF. Comparing MAF frequency with data from the general population proved representative of the control group.
In patients, risky alleles of 11 studied SNPs were more frequent than in the control group. Most of them alone did not have a statistically significant effect, but the cumulative effect of co-occurrence of different SNPs in patients was significant in comparison to the effect of a single SNP. Our results indicated that there is a cumulative effect of the co-occurrence of variants of MBL2 rs1800451 and TIRAP rs8177374. This effect has not been previously described. Both proteins are involved in immune response at different levels. But a combination of defects could give a bigger immune deficit. Weakening of the immune response at several steps (with the participation of different genes) gives a cumulative effect and increases the risk of meningitis. A cumulative effect of different SNPs was described for TLR2 rs5743708 and TLR4 rs4986790. 21 In our previous study we did not detect the significance of a cumulative effect of those SNPs. 22 Only in the case of two polymorphisms – TLR9 rs352140 and TLR4 rs4986790 – were MAF more common in the control group than in the patient group. This is in accordance with literature data. Yuan et al., based on the analysis of a group of 85 children with pneumococcal sepsis, proved that there was a protective effect of the TLR4 rs4986790 polymorphism. 23 Van Well et al. arrived at the same conclusion, based on the analysis of 391 survivors of meningococcal meningitis. 21 In our group (patients and controls), we did not find allele A for TLR9 rs352140, which was showed by Sanders et al. to protect against meningococcal meningitis. 24
Our analysis has shown the important role of SNPs in the MBL2 gene. MBL deficiency is common in the general population. It leads to the reduction of opsonisation in the early phase of infection, leading to longer survival of S. pneumoniae, thus enhancing the possibility of invasion.25,26 Around 5% of the general population has polymorphic variants. 27 Because of its high frequency, MBL polymorphisms may be present in around 32% of patients with meningococcal disease. 28 Our results are in line with some recent studies of MBL deficiency and infections. However, the importance of MBL deficiency in susceptibility to infections is still being discussed, and previous studies have yielded conflicting results. A study by Faber et al. suggested that MBL2 variants are significantly associated with the susceptibility to invasive childhood meningococcal disease in an age-dependent manner and that low serum levels of MBL have been associated with a five-fold increased risk of death due to pneumococcal disease. 28 In this group of patients, the overall frequency of MBL variants was 31.8% versus 8.2% in the general population. Roy et al. reported that individuals with homozygous mutations for MBL codon variants are at an increased risk of invasive pneumococcal disease. 13 Lundbo et al. in their study of 451 Danish children did not show any increased incidence of invasive pneumococcal disease, but this analysis was performed only on patients with pneumococcal meningitis. 25
A crucial role of TLR in invasive bacterial infections was previously confirmed by a number of studies.29–31 S. pneumoniae and N. meningitidis have the potential to activate immune cells through TLR2, TLR4 and TLR9. In meningococcal infections, TLR2 recognises porin B and TLR4 recognises LOS.32–35 In our patients we have not found statistically important results when compared to the control group.
We have shown that components of signal transduction routes of TLRs, such as TIRAP, are important in the pathogenesis of bacterial meningitis. We also studied the TIRAP variant, which was associated with bacterial meningitis in this study, at the level of tendency in analysis of single SNP, and significantly in the analysis of multiple alleles. Some previous studies suggest that the variation in TIRAP is potentially important in determining the susceptibility to infectious diseases, such as tuberculosis. 8 Ladhani et al. showed that polymorphic variants of TIRAP were associated with an increased risk of invasive Haemophilus influenzae disease. 17 Homozygous variants of TIRAP rs8177374 are rare in developing countries. 17 This fact supports speculation that the homologous recessive TIRAP variant may increase the susceptibility to specific infectious diseases to such an extent that it may have selected itself out of population. 19
The previously described association between SNPs in CFH and meningococcal meningitis was not found in our population.9,10,36 Davila et al. showed in two studies a protective effect of minor alleles of CFH rs1065489. The prevalence of mutated variants in patients was 12% and 17% in the control group. Bradley et al. had similar results in the patient group, that is, 11.5% (both studies used the same control group).9,36 In our patients, the prevalence of CFH-mutated variants was similar to the control group population. We do not have data for the Polish population, but the data for the control group were similar to the Central European Group (CEU) from the 1000 Genome Project. MAF frequency in CFH differs between populations: high frequency in East Asia (49.7%), moderate frequency in America (19.1%) and Europe (18.3%), and low in Africa (3.7%). 20 The prevalence of meningococcal disease is the opposite, namely highest in Sub-Saharan Africans, for whom the frequency of MAF is the lowest.
A weak point of this study was the relatively small group of patients; for example, we did not have enough genotype data to study the role of the TLR2 and TLR9 haplotypes. Thanks to vaccination, the number of bacterial meningitis cases in children is decreasing, thus it is difficult to collect a large study group. On the other hand, we collected and studied a standardised group; all our patients were of Caucasian origin and were vaccinated according to the same vaccination schedule, not including pneumococcal and meningococcal vaccines. Our analysis was based on the co-occurrence of several SNPs, so we couldn’t use data from the general population to increase the control group. Prevalence of SNPs is different in each population, while our group was representative of the Polish population. Additionally, we examined the usefulness of available data from the CEU population for the analysis of haplotypes in this study. Unfortunately, the CEU population is underrepresented in the 1000 Genomes Project database (n = 99), and there were too few data to calculate LD for the studied TLR2 SNPs. In the case of TLR9, results were comparable to ours, showing high values of D’ (0.894) and low r2 (0.133; data not presented), which confirms the need to determine both variants for risk assessment.
From another point of view, the strength of this study was that we focused exclusively on meningitis patients in order to find the host genetic determinants of the disease. Our cohort of patients with meningitis was relatively small; however, the results that we found in this group were quite significant, especially for pneumococcal meningitis. Using healthy family members as a control group is another big advantage of our study. Family members share the same environmental risk factors and have similar exposure to pathogens, especially in the youngest group. This enabled the comparison, not only of single SNPs, but the co-occurrence of 11 SNPs in patients and their family members. It increased the chances of finding people with the same set of polymorphisms.
Our analysis showed that genetic factors are important in determining the susceptibility to bacterial meningitis. In order to assess the risk of developing bacterial meningitis, it is essential to analyse SNPs in several genes involved in the immune response, for example, complement pathway and pattern recognition particles. Not a single SNP carriership but the cumulative effect of several SNPs is of clinical importance. Different results were found for S. pneumoniae and N. meningitidis. Analysis of risky alleles can indicate people prone to the disease who are somehow ‘gene-immunocompromised’.
Conclusions
Genetic factors are important in determining the susceptibility to bacterial meningitis. We have detected a statistically significant cumulative effect of mutated variants on increasing the risk of bacterial meningitis in children. Carriers of at least six risky alleles have an 8.4-times higher risk of developing pneumococcal meningitis. Combining all three SNPs in the MBL2 gene improves the prediction of susceptibility to pneumococcal meningitis.
Supplemental Material
EG Suppl B - Supplemental material for How many single-nucleotide polymorphisms (SNPs) must be tested in order to prove susceptibility to bacterial meningitis in children? Analysis of 11 SNPs in five genes involved in the immune response and their effect on the susceptibility to bacterial meningitis in children
Supplemental material, EG Suppl B for How many single-nucleotide polymorphisms (SNPs) must be tested in order to prove susceptibility to bacterial meningitis in children? Analysis of 11 SNPs in five genes involved in the immune response and their effect on the susceptibility to bacterial meningitis in children by Ewelina Gowin, Bogna Świątek-Kościelna, Ewelina Kałużna, Ewa Strauss, Jacek Wysocki, Jerzy Nowak, Michał Michalak and Danuta Januszkiewicz-Lewandowska in Innate Immunity
Supplemental Material
EG Suppl Table A - Supplemental material for How many single-nucleotide polymorphisms (SNPs) must be tested in order to prove susceptibility to bacterial meningitis in children? Analysis of 11 SNPs in five genes involved in the immune response and their effect on the susceptibility to bacterial meningitis in children
Supplemental material, EG Suppl Table A for How many single-nucleotide polymorphisms (SNPs) must be tested in order to prove susceptibility to bacterial meningitis in children? Analysis of 11 SNPs in five genes involved in the immune response and their effect on the susceptibility to bacterial meningitis in children by Ewelina Gowin, Bogna Świątek-Kościelna, Ewelina Kałużna, Ewa Strauss, Jacek Wysocki, Jerzy Nowak, Michał Michalak and Danuta Januszkiewicz-Lewandowska in Innate Immunity
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support was obtained from the Poznan University of Medical Sciences.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.