
Abstract
This study investigates the outcomes of 1106 patients with Dupuytren’s disease treated with limited fasciectomy or percutaneous needle fasciotomy over 16 years according to the different domains of patient-reported hand function. These patients completed the Michigan Hand Outcomes Questionnaire before and 3 months after surgery. Scores for the various outcome parameters were calculated and linear regression analyses were used to examine associations between the changes in digital extension deficit and change in Michigan Hand Outcomes Questionnaire (sub)scores. We found the largest effects of surgical treatment in the decreases in extension deficit, the appearance of the hand, and the satisfaction with the hand function. However, associations between different domains of evaluation were weak. We conclude that improvement of digital extension deficits is not parallel to varying aspects of patient satisfaction. The findings underline the importance of assessing domains relating to patient satisfaction other than objective hand function measures in Dupuytren’s disease.
Keywords
Introduction
Hand surgical treatment options are focused on restoring the function of the upper extremity. Improvements in range of motion or hand strength are widely used, which provide an objective measurement of the hand function. Additionally, patient-reported outcome measures (PROMs) are used to reflect the patients’ perspectives of the impact of disease treatment on hand function. In Dupuytren’s disease it is generally assumed that improvement of the hand function is an important goal for patients, with the aim to improve the range of motion of a finger or fingers by reducing the contracture(s). However, several studies have shown that an increase in range of motion is poorly correlated with an improvement in patient-reported hand function (Degreef et al., 2009; Zyluk and Jagielski, 2007). Comparative studies between various treatments have shown that, despite similar contracture reduction, differences exist in patient-assessed hand function and satisfaction with hand function (Zhou et al., 2016b; 2017). Thus, improvement of patient-reported hand function is not simply achieved by correcting the extension deficits.
While most Dupuytren’s disease-related studies focus on contracture correction and self-reported hand function, several studies regarding rheumatoid arthritis have shown that postoperative hand appearance was an important determinant of patient’s satisfaction (Bogoch et al., 2011; Mandl et al., 2002). Zhou et al. (2016a) demonstrated that hand appearance is an important predictor for patient satisfaction in Dupuytren's disease. Kan et al. (2016) examined patients’ preferences for treatment and found that complete contracture reduction was the most important attribute, but that patients were willing to trade up to almost 5% increase in recurrence rate and 4° of residual contracture deficit for an excellent aesthetic result compared with a moderate result. This suggests that other issues besides hand function might be important to patients with Dupuytren’s disease.
Clinicians may already recognize that aspects such as aesthetics play an important role, but most PROMs solely assess hand function (Johnson et al., 2015). For example, the Disability of the Arm, Shoulder and Hand questionnaire (DASH), does not assess hand appearance or satisfaction. The same is true for the only Dupuytren-specific PROM available, the Unité Rhumatologique des Affections de la Main (URAM) (Beaudreuil et al., 2011). Other PROMs, for example the Patient Evaluation Measure (Macey et al., 1995), have a single question on the appearance of the hand, but these are included in a total score, making assessment of various issues impossible. However, the Michigan Hand Outcomes Questionnaire (MHQ) has separate domains on hand appearance and satisfaction (Shauver and Chung, 2013) to assess different domains of patient-reported hand function.
We assessed the effect of treatment of Dupuytren’s disease on the different domains of patient-reported hand function as measured with the MHQ and assessed to what extent change in the different domains of the MHQ was associated with the change in contracture correction.
Methods
Patients and followup
Patients who underwent either limited fasciectomy or percutaneous needle fasciotomy for Dupuytren’s contractures between February 2011 and June 2017 at a consortium of 16 hand surgery practice sites in the Netherlands were selected from a prospectively maintained database designed for clinical and research purposes. Following the definition of Tang and Giddins (2016), all surgeons were specialists with level II to IV experience; all have between 2 and 20 years of experience of being hand surgeons, including one senior expert in the field of Dupuytren’s disease. Total extension deficit of the affected fingers was assessed prior to surgery and 3 months after surgery. Patients with baseline finger goniometry and a completed MHQ at baseline were eligible for this study. Patients with an affected thumb at baseline were not eligible, as problems with the thumb affect hand function very differently compared with other fingers. Patients with both finger goniometry and a completed MHQ at follow-up were included in the final analyses. Patient- and disease-specific characteristics derived from this database were age, sex, occupational status, family history of Dupuytren’s disease, hand dominance, whether surgery was for primary or recurrent disease, and type of surgery.
As part of routine outcome measurement, patients were invited to complete the MHQ prior to surgery and 3 months afterwards (Chung et al., 1998). This thoroughly developed, hand-specific PROM assesses six domains of hand function: overall hand function, activities of daily living (ADL), work performance, pain, aesthetics, and patient satisfaction with hand function. All questions were answered by means of a five-point Likert scale. Domain and total scores, ranging from 0 (poorest function) to 100 (best function), were calculated according to the questionnaire developer’s instructions (Chung et al., 1998). Two reminders were mailed to non-responders. Only the scores pertaining to the treated hand were used. As a measure of treatment effectiveness, the change between the pre- and postoperative PROM for each patient was calculated.
The degree of total active extension deficit was assessed by hand therapists during visits prior to surgery and 3 months after surgery by summing the degree of active extension deficit at the metacarpophalangeal, proximal interphalangeal, and distal interphalangeal joints. Assessment prior to and after surgery were done at times by the same or by different hand therapists. Any hyperextension was converted to 0° at an individual joint level to prevent underestimation of the total degree of extension deficit. As a measure of treatment effectiveness, the change between the pre- and postoperative extension deficit for each patient was calculated. When multiple digits were affected, we used the measurements pertaining to the most severely contracted digit at baseline.
Statistical analyses
Cohen’s D effect sizes for paired data were calculated to facilitate comparison between the various outcome parameters. This standardized measure of effect describes the magnitude of change and can be interpreted as follows: 0.20, small; 0.50, medium; 0.80, large effect size (Sullivan and Feinn, 2012).
The relationship between the change in finger goniometry and change in different (sub)scores of the MHQ was assessed using linear regression analyses. For each MHQ (sub)score, two separate models were used. In the first model, the change in the various MHQ (sub)scores were introduced as the dependent variable and the change in extension deficit as the independent variable, along with the extension deficit at baseline prior to surgery to correct for baseline differences. In the second model, the above-mentioned patient- and disease-parameters were added as independent variables to the first model to correct for potential confounding of the association studied in the first model. The explained variance was calculated of both models to assess to which extent the independent variables could explain the variance in MHQ (sub)scores.
A power analyses for the multivariable linear regression models determined that a sample size of 394 patients would provide a power of 80% with 20 independent variables (to account for dummy variables) in the model, given a significance threshold of 0.05 and an expected explained variance of 5%.
Results
Information and characteristics of 1106 patients.
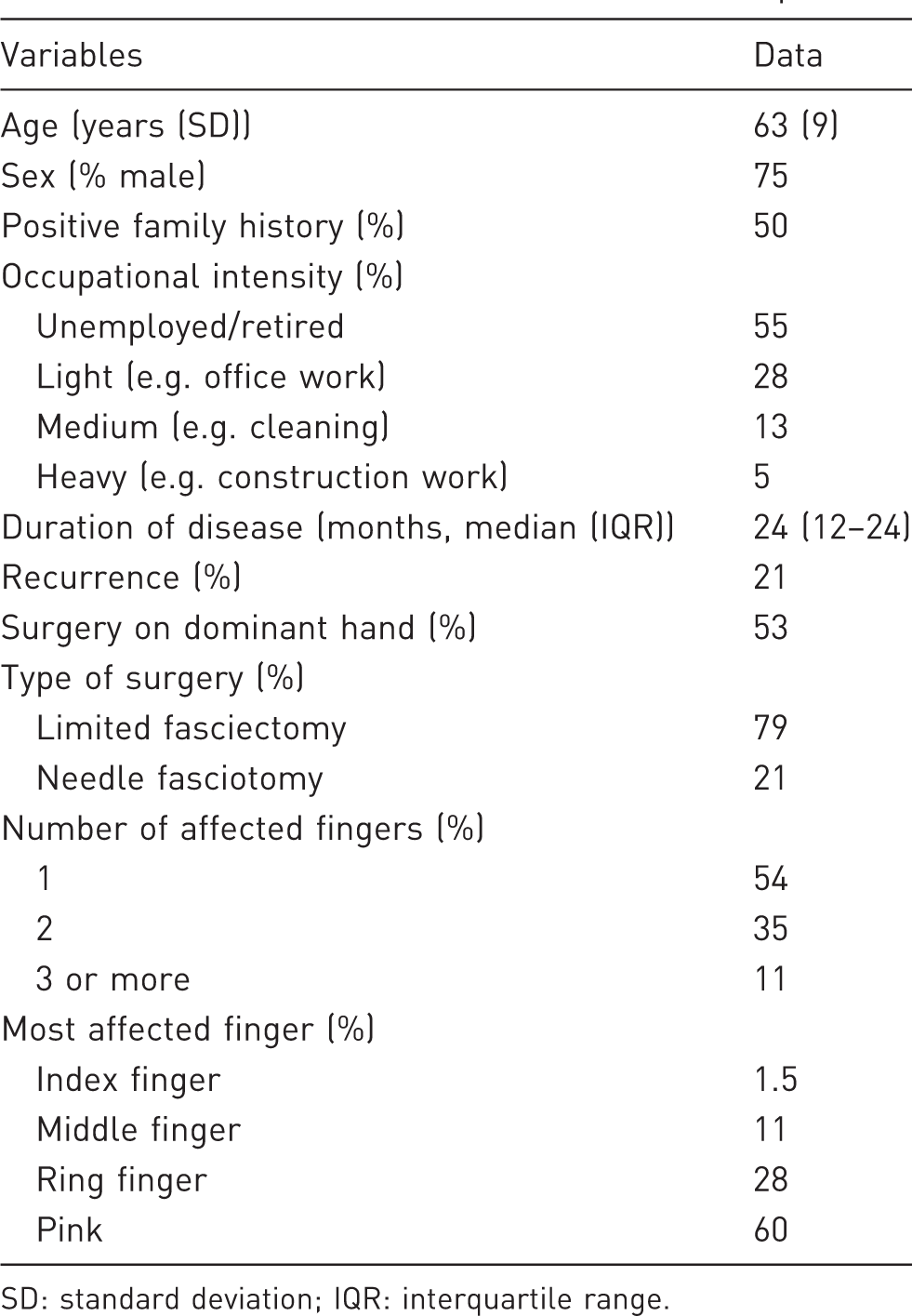
SD: standard deviation; IQR: interquartile range.
Mean and standard deviation (in parenthesis) before surgery (baseline) and 3 months after surgery of 1106 patients.
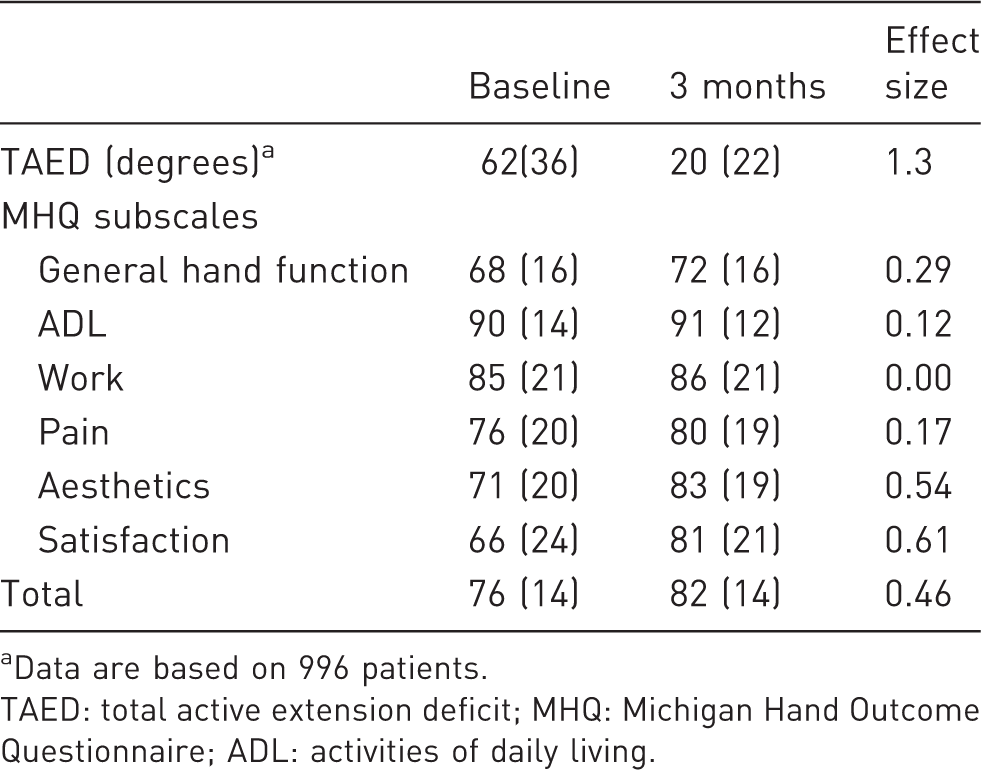
Data are based on 996 patients.
TAED: total active extension deficit; MHQ: Michigan Hand Outcome Questionnaire; ADL: activities of daily living.
Beta-coefficients for the change in MHQ (sub)scales adjusted for baseline extension deficit (n = 996).
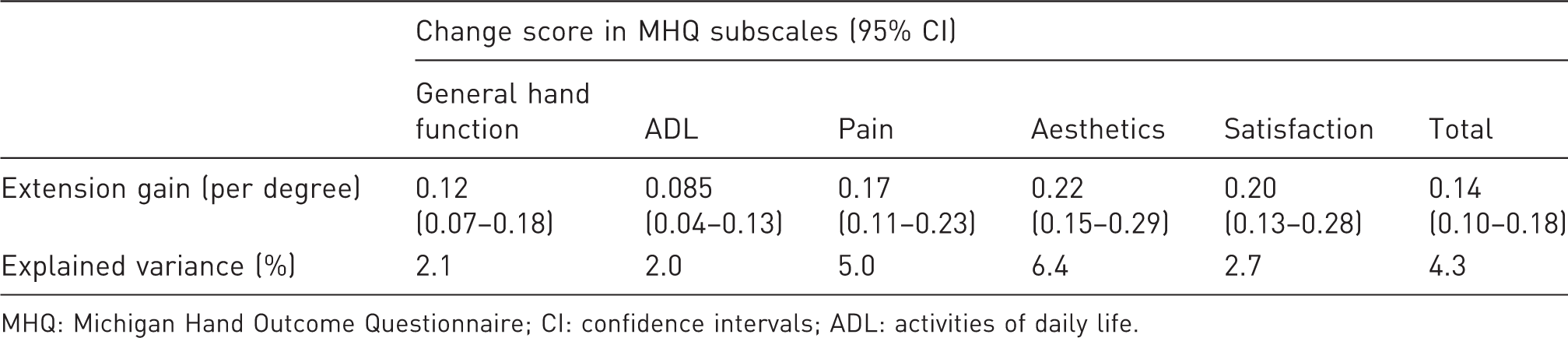
MHQ: Michigan Hand Outcome Questionnaire; CI: confidence intervals; ADL: activities of daily life.
Beta-coefficients a for the change score in MHQ (sub)scales (n = 996).
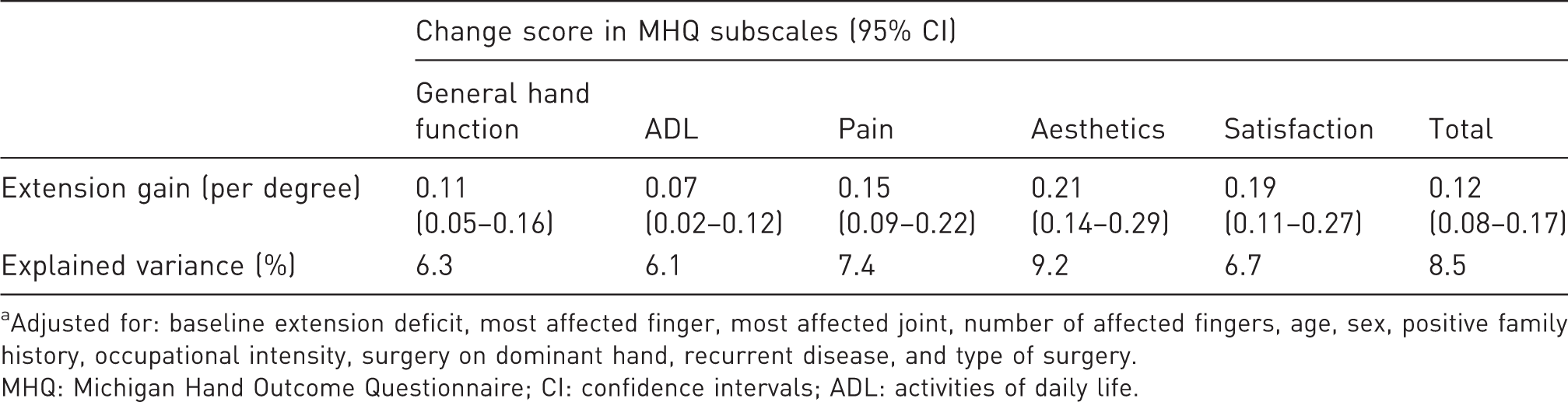
Adjusted for: baseline extension deficit, most affected finger, most affected joint, number of affected fingers, age, sex, positive family history, occupational intensity, surgery on dominant hand, recurrent disease, and type of surgery.
MHQ: Michigan Hand Outcome Questionnaire; CI: confidence intervals; ADL: activities of daily life.
Discussion
We found that the effect size of surgery on goniometry was more than double that of the PROMs. Within the PROMs, we found that a decrease in extension deficit mainly improved the appearance of the hand and the satisfaction with the hand function. General hand function and ADL subscales of the MHQ also improved, but less than subscales for hand appearance and satisfaction with hand function, and these effects may not be clinically relevant. All of the improvements in patient-reported outcomes had a positive but weak association with the improvement in extension deficit. Confounding by patient- and disease-specific characteristics was limited across most subscales. Most notably, recurrent disease, the type of treatment, and the number of affected fingers did not confound the associations between the improvements in the various subscales of the MHQ and the improvement in extension deficit. The association between the improvement in extension deficit and the improvement in the ‘aesthetics’ subscale was the strongest association with the highest explained variance.
These results show that the appearance of the hand might be important to patients with Dupuytren’s disease, as is suggested by the large improvement in the ‘aesthetics’ subscale and the relative strong association with the improvement of finger goniometry compared with the more function-related subscales. This is in line with findings in patients with degenerative and inflammatory joint diseases or with injuries, which showed that despite a clear loss in function, patients have concerns about hand appearance (Chung et al., 2006; Ni et al., 2012). For example, in rheumatoid arthritis, patients reported larger improvements in appearance than function or pain relief after metacarpophalangeal joint arthroplasty (Chung et al., 2012). Since patients with Dupuytren’s disease develop contractures resulting in highly visible hand deformities, similarly to patients with hand osteoarthritis, this aesthetic discomfort in Dupuytren’s disease might be associated with depressive symptoms and poor health-related quality of life (Hodkinson et al., 2012). The discrepancy between the improvement in the ‘general hand function’ subscale and ‘satisfaction with hand function’ subscale is remarkable. This discrepancy suggests that patients separately assess their hand function and how satisfied they are with this function. A possible explanation is that satisfaction is determined by multiple factors, including the expectations and experience of a treatment as well as psychological and emotional factors of a patient (Hageman et al., 2015; Kavalniene et al., 2018; Marks et al., 2011).
The small effect in the ‘ADL’ subscale, indicating a lack of sensitivity for evaluating the treatment effect in Dupuytren’s disease, may be related to the specific, predefined tasks included in the relatively generic hand function measure. Patients with Dupuytren’s disease experience a broad range of functional problems, which are not covered by the items of the ADL subscale of the MHQ. The specific tasks included in the MHQ might not be those tasks that are problematic in patients with Dupuytren’s disease, and patients already score near the maximum score prior to treatment. The same problems occur in other questionnaires, including the DASH and URAM (Engstrand et al., 2009; Rodrigues et al., 2015). A possible solution would be to use patient-specific PROMs, such as the Patient-Specific Functional Scale (Fairbairn et al., 2012) or the Canadian Occupational Performance Measure (Van de Ven-Stevens et al., 2015), which allow patients to specify tasks with which they have difficulty and score their progress. Relating the improvement in these scores to the reduction in extension deficit may give a more accurate estimate to what extent the reduction in extension deficit really does improve the performance of tasks patients seek help for.
The large loss to follow-up (60%) is a limitation of this study. This may have led to under- or overestimation of the identified associations, as it is unknown if the patients lost to follow-up represent a group with good or poor results. However, sensitivity analyses found no significant or clinically relevant differences in baseline between patients included in this study (with both goniometry and MHQ at follow-up) and patients not included in this study (Online Table S1). Similarly, no significant differences were seen in goniometry or in minor differences (2 points or less) in MHQ scores between included patients and patients with partial follow-up measurements (with MHQ at follow-up, but no goniometry (n = 667) and vice versa (n = 225)) (Online Table S2). A second limitation in this study is the possible lack of sensitivity in the various function-related subscales. Lastly, 3 months might be too early to notice full functional recovery following fasciectomy. However, in patients with Dupuytren’s disease, the time to follow-up remains a trade-off between the time to full hand function recovery and the recurrence of Dupuytren’s disease, which could be as early as 3 months after surgery (Dias et al., 2013).
Supplemental Material
JHS890284 Supplemental Material1 - Supplemental material for Patient’s satisfaction beyond hand function in Dupuytren’s disease: analysis of 1106 patients
Supplemental material, JHS890284 Supplemental Material1 for Patient’s satisfaction beyond hand function in Dupuytren’s disease: analysis of 1106 patients by Ralph Poelstra, Yara E. van Kooij, Mark J. W. van der Oest, Harm P. Slijper, Steven E. R. Hovius, Ruud W. Selles and the Hand-Wrist Study Group in Journal of Hand Surgery (European Volume)
Supplemental Material
JHS890284 Supplemental Material2 - Supplemental material for Patient’s satisfaction beyond hand function in Dupuytren’s disease: analysis of 1106 patients
Supplemental material, JHS890284 Supplemental Material2 for Patient’s satisfaction beyond hand function in Dupuytren’s disease: analysis of 1106 patients by Ralph Poelstra, Yara E. van Kooij, Mark J. W. van der Oest, Harm P. Slijper, Steven E. R. Hovius, Ruud W. Selles and the Hand-Wrist Study Group in Journal of Hand Surgery (European Volume)
Footnotes
Acknowledgement
We would like to thank all patients for their participation. The members of the Hand-Wrist Study Group are: Arjen Blomme, Berbel Sluijter, Corinne Schouten, Dirk-Jan van der Avoort, Erik Walbeehm, Gijs van Couwelaar, Guus Vermeulen, Hans de Schipper, Hans Temming, Jeroen van Uchelen, Luitzen de Boer, Nicoline de Haas, Oliver Zöphel, Sebastiaan Souer, Thybout Moojen, Reinier Feitz, Xander Smit, Rob van Huis, Pierre-Yves Pennehouat, Karin Schoneveld, Robbert Wouters, Paul Zagt, Folkert van Ewijk, Frederik Moussault, Rik van Houwelingen, Joris Veltkamp, Arenda te Velde, Alexandra Fink, Jarry Porsius, Kim Spekreijse, Chao Zhou, Jonathan Tsehaie, Miguel Janssen, Stefanie Evers, Jak Dekker, Matijs de Jong, Jasper van Gestel, Marloes ter Stege, Menno Dekker, Roel Faber, Frank Santegoets, Monique Sieber-Rasch and Ton Gerritsen.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for research, authorship, and/or publication of this article
Ethical approval
The study protocol (MEC-2018-1088) was approved by the institutional review board of the Erasmus Medical Centre.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.