
Abstract
This prospective study investigates the extent to which a better experience with healthcare delivery is associated with better postoperative treatment outcomes after surgery for Dupuytren’s contracture. Patients undergoing limited fasciectomy or percutaneous needle fasciotomy for Dupuytren’s contractures completed the Michigan Hand Outcomes Questionnaire before and 3 months after surgery, together with a patient reported experience measure, while hand therapists assessed the straightness of the finger with a goniometer. Regression analyses were used to examine associations. We found that a better experience with healthcare delivery was associated with better patient-reported outcomes, while association with residual extension deficit was minimal. Strongest associations were seen with communication of the physician, postoperative care and information about the treatment. Experience with the treatment explained up to 12% of the variance in treatment outcome. These findings suggest that patient reported treatment outcomes in Dupuytren’s disease can be improved by improving the treatment context.
Introduction
In modern practice, both physical treatment outcomes and patient-reported outcome measures (PROMs) are used to evaluate health outcomes after treatment. Most recently, patient-reported experience measures (PREMs) were added to this evaluation (CMS, 2017; Roland, 2004). PREMs focus on aspects such as respect and dignity, communication by physicians and cleanliness or hygiene of facilities, and can be used to routinely measure and quantify different aspects of treatment context or experience with healthcare delivery (Manary et al., 2013). Besides being useful in the evaluation of treatment, PREMs can be useful in clarifying the relation between experiences with healthcare delivery and treatment outcomes. Several observational studies have shown that a better experience with healthcare delivery is associated with better patient-reported outcomes (Black et al., 2014). Although these observational studies do not provide causal evidence for this relationship, recent meta-analyses of randomized clinical trials have shown that influencing the context, for instance by improving the communication between patient and clinician, directly improves the patient-reported health status (Di Blasi et al., 2001; Kelley et al., 2014).
Despite being deemed important (Warwick, 2017), these relationships have not yet been studied in Dupuytren’s disease nor in hand surgery all together. Therefore, the objective of this prospective study was to investigate the extent to which a better experience with healthcare delivery is associated with better postoperative treatment outcomes after surgery for Dupuytren’s contracture, as assessed by both a PROM as well as remaining extension deficit in the finger recorded by a therapist.
Methods
Study design
Patients who underwent either limited fasciectomy or percutaneous needle fasciotomy for Dupuytren’s contractures between February 2011 and December 2016 at a consortium of 16 hand surgery practice sites in the Netherlands were selected from a prospectively maintained database that was designed for clinical and research purposes. Patients who had completed a postoperative PROM and PREM and had finger goniometry recorded were included in the final analysis (Figure 1). All patients provided written informed consent for the use of their data. As part of routine outcome measurement, patients were invited to complete a PROM questionnaire before surgery and both a PROM and PREM questionnaire three months afterwards. Two reminders were mailed to non-responders. Patient- and disease-specific characteristics derived from this database were age, sex, occupational status, co-morbidities, current tobacco and alcohol use, family history of Dupuytren’s disease, hand dominance and postoperative degree of contracture. The study protocol (MEC-2017-1036) was approved by the institutional review board of the Erasmus Medical Centre.
Flowchart of subject inclusion.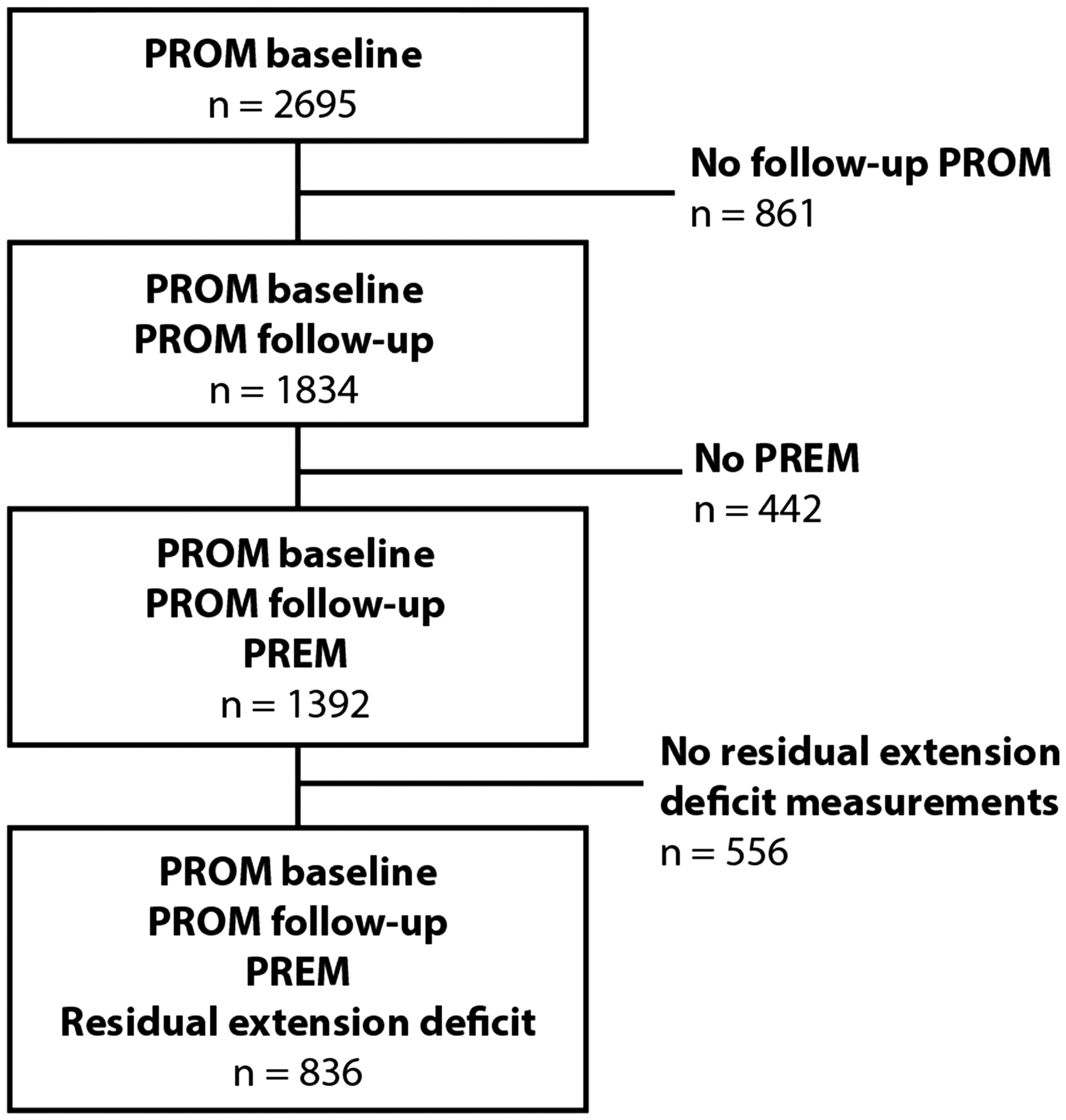
PROM
Patients completed the Michigan Hand Outcomes Questionnaire (MHQ) (Chung et al., 1998). This rigorously developed, hand-specific PROM assesses six domains of hand function: overall hand function; activities of daily living; work performance; pain; aesthetics; and patient satisfaction with hand function. All questions are answered by means of a five-point Likert scale. Domain and total scores, ranging from 0 (poorest function) to 100 (best function), were calculated according to the questionnaire developer’s instructions (Chung et al., 1998). As most of the patients in our population were either unemployed or retired, the domain on work performance was not included in this study. Only the scores pertaining to the treated side were used. As a measure of treatment effectiveness, the change between the pre- and postoperative PROM for each patient was calculated.
PREM
Patients completed the PREM questionnaire, which is widely used in private practice clinics in The Netherlands. This questionnaire aims at measuring the patient’s experience with the clinic, marketing position of the clinic and logistics within a clinic. For the current analysis, 25 items concerning the patient’s experience were used. With help of an exploratory factor analysis six subscales were identified: physician communication and competence (six items); perioperative care (four items); postoperative care (four items); general information (two items); treatment information (three items); quality of facilities (six items) (see appendix S1 which contains the questions used in the PREM questionnaire). The subscale regarding perioperative care was reduced to two items for patients undergoing needle fasciotomy, dropping the items concerning the anaesthetist, as this procedure is done under local anaesthesia administered by the hand surgeon.
Each item pertaining to one of the six domains of healthcare delivery was graded by the patient according to the Dutch academic grading system consisting of a ten-point scale, where one represents a very poor result and ten an excellent result. When a question did not apply to a patient, for example, if they did not use the website, there was a possibility to answer so. Scores on different subscales were determined as the mean of the items on that subscale.
Internal consistency in our sample, assessed using Cronbach’s α, was: physician communication and competence = 0.95; perioperative care = 0.83 (for needle fasciotomy patients = 0.62); postoperative care = 0.89; general information = 0.84; treatment information = 0.87; and quality of facilities = 0.87.
Residual extension deficit
The degree of total residual contracture was assessed by certified hand therapists during visits occurring 6–12 weeks after treatment by calculating the sum of the degree of active extension deficit at the metacarpophalangeal, proximal interphalangeal and distal interphalangeal joint levels. Any hyperextension was converted to 0° at an individual joint level to prevent underestimation of the total degree of extension deficit. When multiple digits were affected, we used the measurements pertaining to the most severely contracted digit at follow-up.
Missing data
Diabetes, smoking and alcohol status was unknown in 18% of the patients. In the PREM questionnaire there were missing data in the ‘postoperative care’, ‘general information’ and ‘perioperative care’ subscales of 17%, 21% and 29%, respectively. In the three remaining PREM subscales, the missing data were < 1%. Subscales with missing data were not calculated, as most of the missing data were accounted for by patients answering that a question did not apply to them.
Statistical analyses
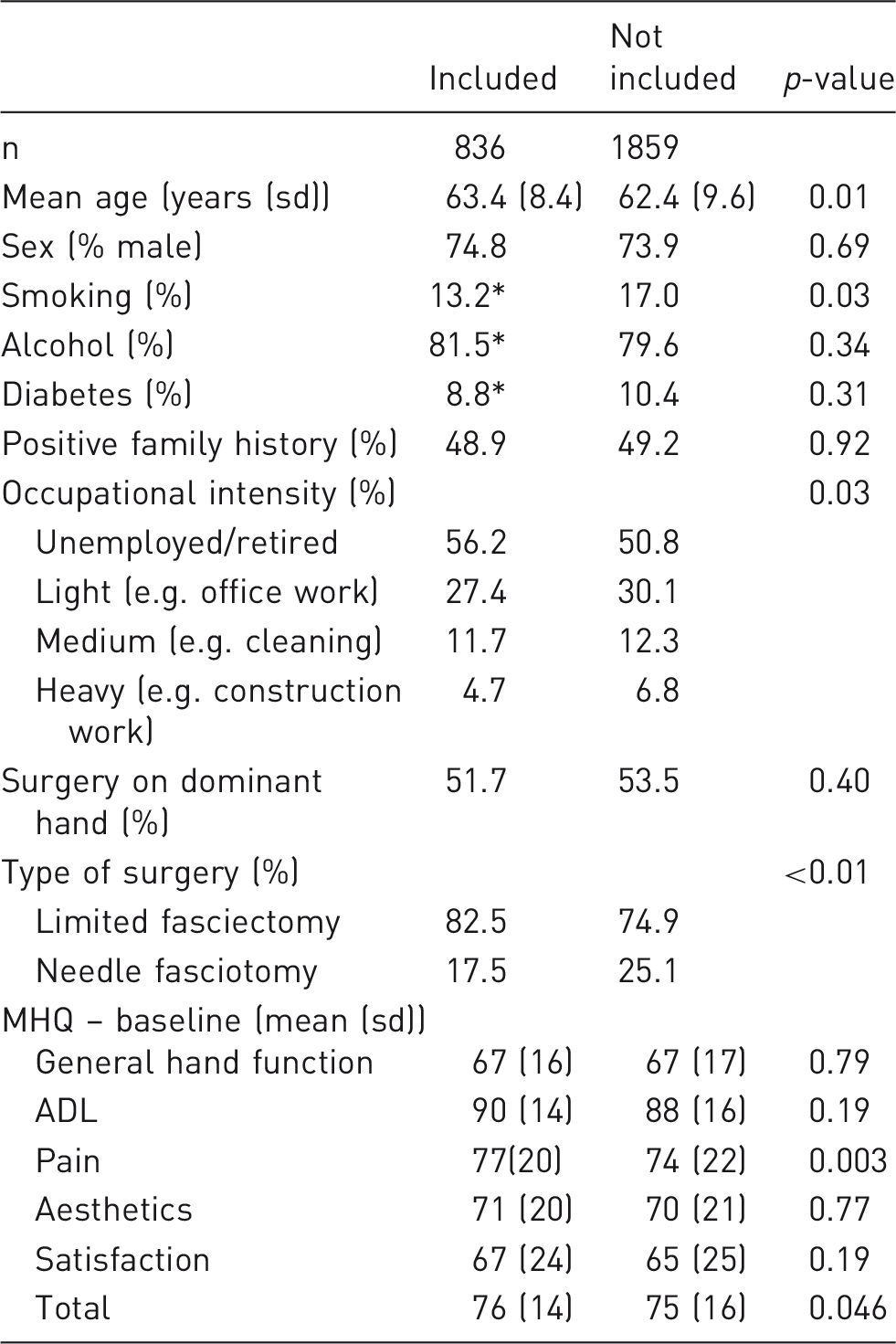
Significance testing was done by means of a Student’s t test for normally distributed data, a Wilcoxon rank-sum test for non-normally distributed data and a chi-squared test for categorical data. Distribution of the data was evaluated with histograms and QQ norm plots. To assess the potential of selection bias, we compared baseline patient characteristics between patients who met the inclusion criteria and those who did not.
To assess the relationship between PREM scores and PROM change scores and residual extension deficit, linear regression analyses were used. Beta-coefficients were used to determine the effect size of each PREM subscale. As the measurement error for goniometry is commonly accepted to be roughly 3–5° per joint (Engstrand et al., 2012), an effect size of < 10° for the residual extension deficit (all joints summed up) was regarded as not clinically relevant. To determine to what extent the variation in treatment outcome between patients could be explained by the experience with healthcare delivery, all six PREM subscales were introduced simultaneously in the same model as independent variables. Multivariable regression models were used to adjust for potential confounders. The significance threshold was set at 0.05.
Results
Baseline characteristics of included vs. not included patients.
n = 688.
MHQ: Michigan Hand Outcome Questionnaire; ADL: activities of daily life.
Outcome measurements of included patients (n = 836).
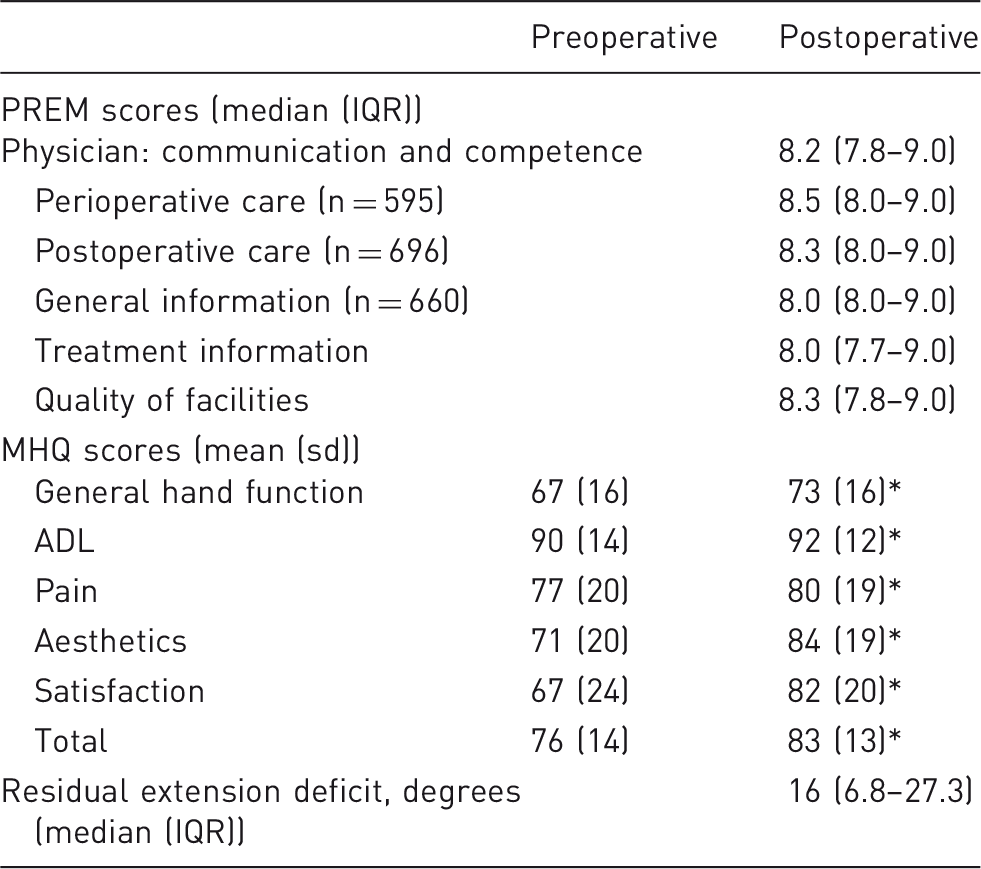
Difference pre- and postoperative with p < 0.01.
MHQ: Michigan Hand Outcome Questionnaire; PREM: patient-reported experience measure; ADL: activities of daily life; IQR: interquartile range; sd: standard deviation.
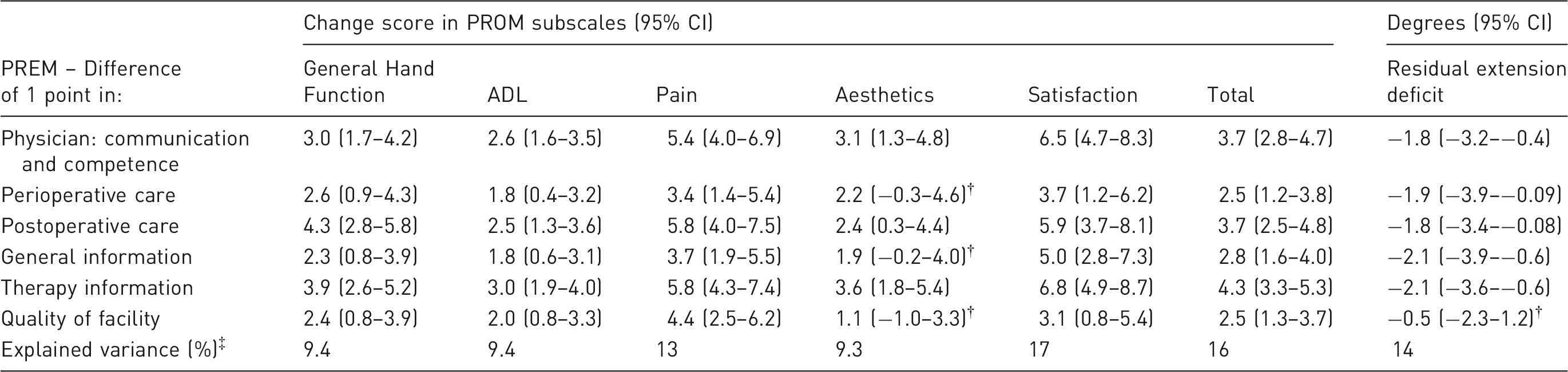
Unadjusted beta-coefficients of change score in PROM subscale and residual extension deficit associated with 1-point difference in PREM score.
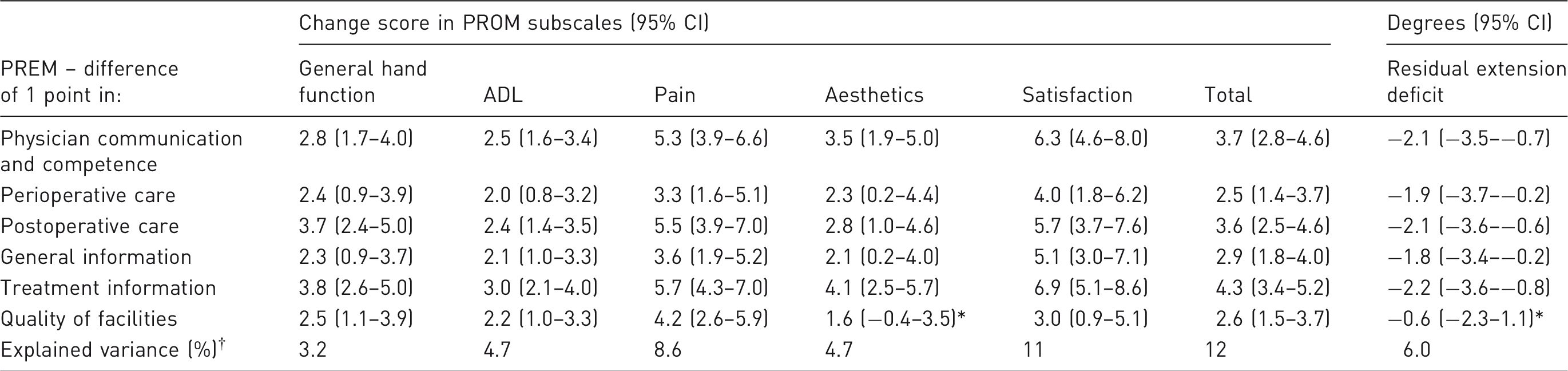
p > 0.05, all others p < 0.05.
All six PREM subscales as independent variables simultaneously to predict either the PROM subscales or residual extension deficit.
PROM: patient-reported outcome measure; PREM: patient-reported experience measure; ADL: activities of daily life.
Similarly, for the univariate relation between the PREM score and residual contraction, we found positive associations between all PREM subscores and straightness of the finger (i.e. a lower residual extension deficit), with only the association between the quality of the facilities and residual contraction not being significant (Table 3). For example, an increase of one point in the physician PREM scale was associated with a decrease of 2.1° in residual extension deficit. However, none of the effect sizes for the residual extension deficit was > 10° and were therefore not clinically relevant.
Adjusted* beta-coefficients of change score in PROM subscale and residual extension deficit associated with 1-point difference in PREM score.
Adjusted for age, sex, diabetes, alcohol, smoking, positive family history, occupational intensity, surgery on dominant hand, recurrent disease and type of surgery.
p > 0.05, all others p < 0.05.
All six PREM subscales as independent variables simultaneously to predict either the PROM subscales or residual extension deficit with correction for potential confounders*.
PROM: patient-reported outcome measure; PREM: patient-reported experience measure; ADL: activities of daily life.
Discussion
In this study, we found that patients with Dupuytren’s contractures who reported more positive experiences with the way their care was delivered also showed more positive treatment outcomes. Confounding factors including patient- and disease-specific characteristics, most notably, recurrent disease, had a limited effect. Thus, previous experience with surgery for Dupuytren’s disease, and the type of surgery, did not influence the associations. While treatment context had a relatively large effect on patient-reported outcomes, the association with physical treatment outcomes was very small and may not be considered clinically relevant. These findings imply that the context of a surgical treatment for Dupuytren’s disease has a greater effect on the patient’s perceived outcomes than on physical treatment outcome measurements.
In general, the domains of ‘physician communication and competence’, ‘postoperative care’ and ‘treatment information’ had the strongest association with a more positive treatment outcome. This finding is in line with previous studies which reported that patient experience with the physician’s communication is the most important factor in the relationship with treatment outcome (Black et al., 2014; Fremont et al., 2001; Slatore et al., 2010). In addition, our results show that a good experience with the treatment information provided was also strongly associated with patient-reported treatment effectiveness. Overall, treatment context explained 11.6% of the variation of the total MHQ score. Addition of patient and disease characteristics as well as surgery type only added an additional 4% to the explained variance of the total MHQ score. These results suggest that treatment context, rather than patient and disease characteristics or the type of surgery, played a large role in predicting patient-reported outcomes in Dupuytren’s.
A possible explanation for these results could be that good communication and good treatment information results in better or more realistic expectations of the outcome. Expectations are seen as a crucial ingredient of placebo-like effects (Crow et al., 1999). It has been shown that expectation can be modulated by using an empathetic interaction style (Kaptchuk et al., 2008) or by discussing a patient’s treatment beliefs (Laferton et al., 2016), which in turn can have a beneficial effect on treatment (Howe et al., 2017; Rief et al., 2017).
Besides the role of optimized expectations, a more positive evaluation of the physician might also reflect a more trustful physician–patient relationship (Street et al., 2009). In turn, this might lead to better treatment adherence and arguably better treatment outcomes (Lin et al., 2017; Linetzky et al., 2017). However, it is also possible that patients with a better outcome will report a better experience, as they may be more inclined to accept shortcomings in their experience with the given care. In the absence of an interventional study, a definitive conclusion about the direction of this association between treatment context and health outcome cannot be made.
The main strengths of this study are the use of both patient-reported and physical outcome parameters, prospective collection of the data and the large sample size collected across the Netherlands. The relative large loss to follow-up (69%) is a limitation of this study, which may have led to under- or overestimation of the identified associations. However, our analyses did not show clinically relevant differences in baseline characteristics between patients who were included or excluded, reducing the likelihood of biased results. It is uncertain if the results are generalizable to other hand disorders. In Dupuytren’s disease, pain is not as prominent as in, for example, arthrosis. This might result in different associations, as patients with pain have different reasons to seek medical help and therefore different expectations from their treatment (Frouzakis et al., 2015). With regard to the patient-reported experience, the questionnaire used in this study is not as thoroughly developed and tested as some of the other experience questionnaires (Beattie et al., 2015). Nevertheless, the subscales showed good internal consistency.
In conclusion, this study shows that a better experience with healthcare delivery is associated with a better treatment outcome in the treatment of Dupuytren’s disease. Optimizing experience with healthcare delivery may provide a new and relatively unexplored pathway for improving healthcare outcomes in hand surgery.
Supplemental Material
Appendix -Supplemental material for Better patients’ treatment experiences are associated with better postoperative results in Dupuytren’s disease
Supplemental material, Appendix for Better patients’ treatment experiences are associated with better postoperative results in Dupuytren’s disease by Ralph Poelstra, Ruud W. Selles, Harm P. Slijper, Mark J.W. van der Oest, Reinier Feitz, Steven E.R. Hovius and Jarry T. Porsius in Journal of Hand Surgery (European Volume)
Footnotes
Acknowledgements
The authors thank all patients for their participation.
The members of the Hand-Wrist Study Group are: Arjen Blomme, Berbel Sluijter, Corinne Schouten, Dirk- Jan van der Avoort, Erik Walbeehm, Gijs van Couwelaar, Guus Vermeulen, Hans Schipper, Hans Temming, Jeroen van Uchelen, Luitzen de Boer, Nicoline de Haas, Oliver Zöphel, Sebastiaan Souer, Thybout Moojen, Xander Smit, Rob van Huis, Pierre-Yves Pennehouat, Karin Schoneveld, Yara van Kooij, Robbert Wouters, Paul Zagt, Folkert van Ewijk, Frederik Moussault, Rik van Houwelingen, Joris Veltkamp, Arenda te Velde, Alexandra Fink, Kim Spekreijse, Chao Zhou, Jonathan Tsehaie, Miguel Janssen, Stefanie Evers, Jak Dekker, Matijs de Jong, Jasper van Gestel, Marloes ter Stege, Menno Dekker, Roel Faber, Frank Santegoets, Monique Sieber-Rasch and Ton Gerritsen.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.