
Abstract
Universal 2 implants may be an alternative to total wrist arthrodesis for the salvage of failed Biaxial total wrist prostheses. We assessed 40 Universal 2 revision implants retrospectively. Fourteen of these wrists were converted to total wrist arthrodeses, and two wrists received a third total wrist arthroplasty after a mean period of 5.5 years. Twenty-four of the Universal 2 implants that remained in situ after a mean follow-up of 9 years (range 4 to 13 years) were re-examined. Sixteen functioned satisfactorily. Patient-Rated Wrist and Hand Evaluation scores and Quick Disabilities of the Arm, Shoulder and Hand scores were 53 and 47, respectively. Twenty-nine patients would choose the Universal 2 again and would also recommend it to other patients. The survival of the revision implants was 60% at a mean follow-up of 9 years.
Introduction
Rheumatoid arthritis and post-traumatic or idiopathic osteoarthritis may eventually totally destroy the wrist joint. Total wrist arthroplasty (TWA) aims at restoring function and relieving pain in these severely damaged wrists. In 1983, Beckenbaugh (1991) introduced the formerly widely used Biaxial implant (BIAX, DePuy, Inc., Warsaw, IN), a third generation TWA with a single-pronged distal component. Despite promising short-term outcomes, the BIAX implant faced failure rates of 17% to 19% after 5 to 8 years (Harlingen et al., 2011; Krukhaug et al., 2011; Takwale et al., 2002). This was generally caused by fixation failure of the distal component (Talwalkar et al., 2005).
Replacing the failed BIAX implant with the same type of prosthesis is either impossible or likely to fail due to poor carpal and especially metacarpal bone stock (Cobb and Beckenbaugh, 1996). Conversion to a total wrist arthrodesis used to be the inevitable consequence for these patients (Adams et al., 2016; Talwalkar et al., 2005).
Only a few studies reviewed the revision of a failed TWA by replacing the implant with a different type (Cobb and Beckbaugh, 1996; Fatti et al., 1991; Khan et al., 2014; Lorei et al., 1997; Pinder et al., 2018; Rettig and Beckenbaugh, 1993). These studies concerned small and/or heterogeneous case series or case reports and described short-term, sometimes mid-term, outcomes. They generally reported on obsolete implant designs and had high implant failure rates.
In 2004 we started using the Universal 2 total wrist prosthesis (Integra, Plainsboro, NJ, USA) for revision of failed BIAX implants. In this study, we present a case series with mid-term results of patients with failed BIAX total wrist implants that were converted to Universal 2 implants.
Methods
Study design
The study was conducted retrospectively. A database search identified patients with failed BIAX implants that were converted to Universal 2 implants between 2004 and 2013 at the Albert Schweitzer Hospital in Dordrecht, The Netherlands. A letter of notification was sent to inform the patients about the upcoming survey. Patients could reply to the letter to confirm or decline participation. Contact was initiated when patients did not respond or confirmed to participate. After verbal agreement, questionnaires were conducted by telephone or sent by (e-)mail, and relevant data were extracted from the medical records: demographics; perioperative findings; X-rays; complications; and indication for revision of the BIAX and Universal 2 implant. Other hospitals and/or the patient’s general practitioner were contacted in case of missing data. Patients who passed away or who could not be reached were excluded from this study. The study was approved by the Medical Ethical Committee at the Albert Schweitzer Hospital in Dordrecht, The Netherlands.
Surgical technique and postoperative treatment
All operations were performed by two senior surgeons (CMvL and CBIJ, experience level V (Tang, 2009). Preoperatively, all patients received a single dose of antibiotic. The patient’s upper limb was positioned in 90° abduction with the palm facing downwards. A tourniquet (250–300 mmHg) was used. The wrist was approached through a 7 cm dorsal incision in the existing longitudinal scar. The third extensor compartment was opened and the extensor pollicis longus tendon was retracted radially. The fourth extensor compartment was elevated from the radius and capsule and held ulnarly. The dorsal wrist capsule was opened longitudinally. Osteotomes were used to remove the BIAX implant, taking care to preserve carpal and metacarpal bone stock. The proximal carpal row and ulnar head had already been resected in all wrists during the previous operation. The uncemented Universal 2 implant was inserted according to the operative technique described by Adams (2004). Autologous corticocancellous bone graft from the iliac crest was used in all patients to augment carpal and metacarpal bone stock and to improve distal component fixation. The bone graft was fixed between the Universal 2 carpal plate and the remaining distal carpal bones using the screws of the carpal plate. No graft or cement was used in the radius. A drain was used in all cases, which was generally removed the first postoperative day.
Postoperative treatment consisted of cast-immobilization for 4 weeks, followed by hand therapy. A custom-made splint was fabricated and intermittently used during heavy physical activity.
Clinical evaluation
The outcome of the Universal 2 implant was primarily assessed by implant survival. The Universal 2 implants that remained in situ were assessed with patient-related outcome measures (PROMs): the Patient-Rated Wrist and Hand Evaluation questionnaire (PRWHE; Dutch version) (MacDermid et al., 1998), the Quick Disabilities of the Arm, Shoulder and Hand questionnaire (QuickDASH; Dutch language version) (Kennedy et al., 2011) and visual analogue scale pain scores. Additionally, patients were evaluated for the use of a wrist brace and for limitations in performing activities of daily living. All included patients were asked if they would choose the Universal 2 implant again as the salvage treatment for their failed BIAX implant and if they would recommend the Universal 2 implant revision to other patients with a failed BIAX implant. Patients with a Universal 2 implant in one wrist and a total wrist arthrodesis in the opposite wrist were asked to determine if they preferred the Universal 2 implant to a total wrist arthrodesis as the treatment for their failed BIAX implant. The cumulated survival of the Universal 2 was calculated according to the Kaplan–Meier method without including the patients lost to follow-up.
Radiographic assessment
The first and fifth author (HJAZ and CBIJ, respectively) evaluated the radiographs and related reports. Radiographs of the BIAX (just before revision) and Universal 2 implants were evaluated for implant positioning and signs of osteolysis. The immediate postoperative and final radiographs (before Universal 2 removal in case of Universal 2 failure or at final follow-up in case the Universal 2 had not failed) were evaluated in the medical records. Since there is no validated grading system for periprosthetic osteolysis at the wrist joint, we evaluated osteolysis as follows: (I) no radiolucent lines; (II) radiolucent lines; (III) extensive radiolucency without implant subsidence and/or radiographic signs of (sub)luxation; (IV) extensive radiolucency with implant subsidence and/or radiographic signs of (sub)luxation.
Statistics
The chi-squared test was used to examine the relation between the degree of osteolysis surrounding the BIAX implant and the incidence of subsequent Universal 2 implant failure. The chi-squared test was also used to examine the difference between rheumatoid and non-rheumatoid patients in terms of implant failure. The level of significance was set at p < 0.05.
Results
Follow-up and demographics
The database search identified 52 patients (57 wrists) with failed BIAX implants that were converted to Universal 2 implants. Fifteen patients were excluded from this study: two patients did not want to participate, two had died of an unrelated condition and 11 could not be reached (Figure 1). Thirty-seven patients (40 wrists, 21 women and 16 men) with a mean age of 58 years (range 32 to 83) were included in this study. In 24 patients the diagnosis was rheumatoid arthritis, in 11 it was osteoarthritis and in two Kienböck’s disease.
Flow diagram of the search and inclusion of cases.
Clinical evaluation
Indications for the revision of failed implants.
Radiographic evaluation
Radiographic findings of BIAX (just before revision) and Universal 2 (long-term, but before revision in case of implant removal) implants are described in Table 2 and are demonstrated in Figure 2. Adequate Universal 2 implant positioning was seen in all immediate postoperative X-rays. There was no relation between osteolysis surrounding the BIAX implant before revision and subsequent Universal 2 implant failure (p = 0.22).
Radiographs of the right hand of a 61-year-old woman with post-traumatic osteoarthritis demonstrating periprosthetic osteolysis. (a) The BIAX implant before revision. (b) The Universal 2 implant 8 years after revision. Radiographic findings: periprosthetic osteolysis and subsidence. I: no radiolucent lines. II: radiolucent lines. III: extensive radiolucency without implant subsidence or (sub) luxation. IV: extensive radiolucency with implant subsidence and/or (sub) luxation. The radiographs of one patient were missing.
Complications and revisions
No immediate postoperative complications (infection, complex regional pain syndrome, dislocation or tendon ruptures) had occurred after primary revision. Sixteen Universal 2 implants eventually failed and were converted to a total wrist arthrodesis in 14 patients and a tertiary TWA in two, again using a Universal 2 implant, after a mean period of 5.5 years (range 0 to 10). The cumulated survival of the Universal 2 implants is shown in Figure 3. There was no significant difference between rheumatoid and non-rheumatoid patients in terms of in Universal 2 implant failure (p = 0.79).
The secondary Universal 2 cumulated survival rate.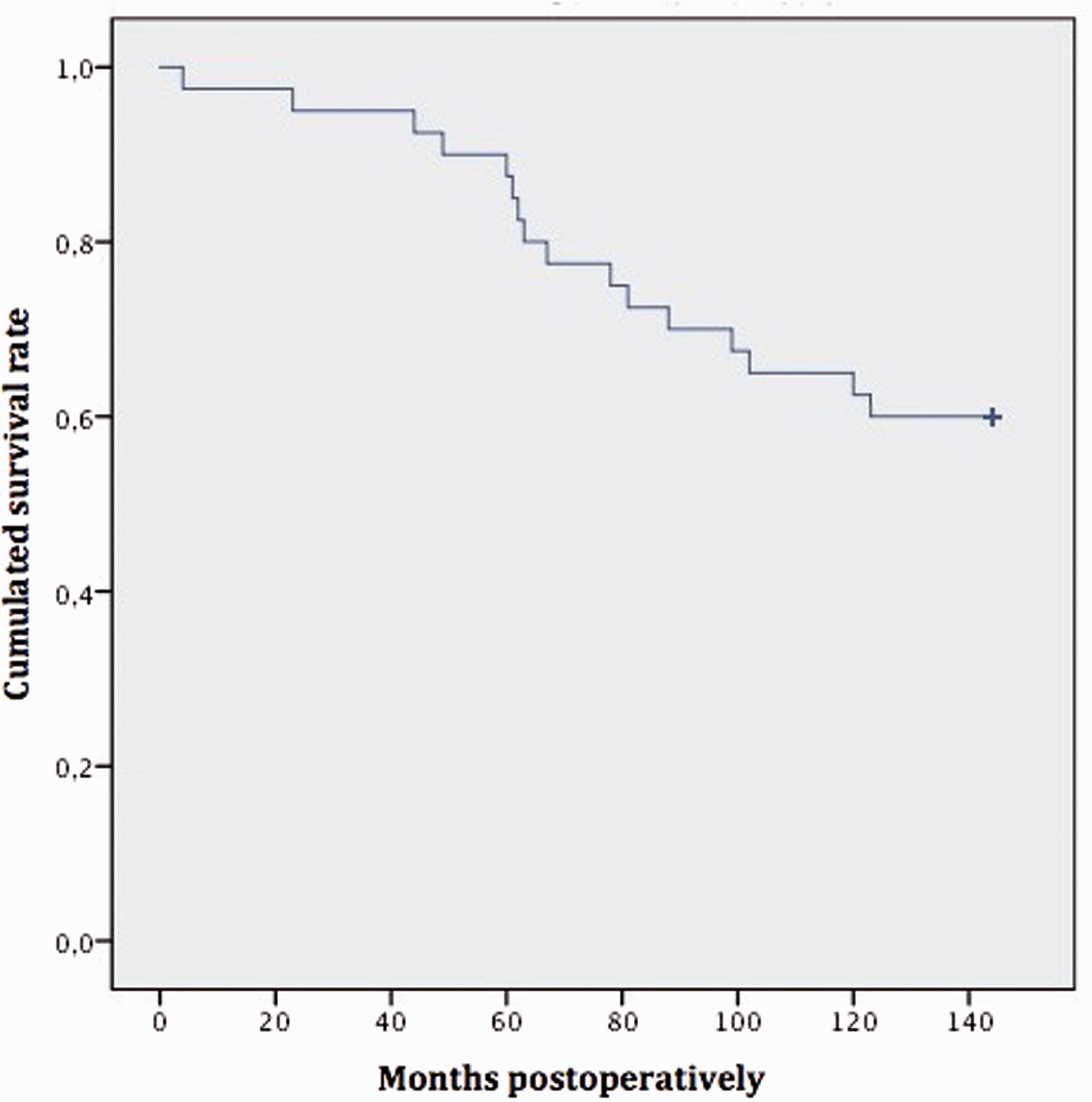
Discussion
Total wrist arthrodesis for the salvage of failed TWA results in a complete limitation of wrist flexion/extension and radial/ulnar deviation (Adams et al., 2016). To prevent these limitations, failed implants can possibly be salvaged by a revision implant. Pinder et al. (2018) evaluated BIAX and Universal 2 implants that were used to salvage failed BIAX, Swanson and Universal 2 implants. At 5 years follow-up, two of the nine Universal 2 implants had failed. Two other studies reported on failed BIAX implants that were converted to Universal 2 implants (Cooney et al., 2012; Kretschmer and Fansa, 2007). However, the aim of both studies was to report on the initially used implant (i.e. the BIAX implant) and therefore they did not extensively report on the revisional Universal 2 implant. In contrast to the current literature, our study evaluated a larger case series.
Outcome was assessed by implant survival, PROMS and a patient satisfaction survey. Implant survival was 60% at 9 years follow-up, which is definitely lower compared with the survival rate in primary Universal 2 implants (82% to 85% at 7 years follow-up) (Kennedy et al., 2018; Pfanner et al., 2017). This discrepancy can probably be explained by the poor local bone stock after BIAX implant removal, which implies a higher risk of repeat implant failure. Implant survival alone is not sufficient to assess the true revisional implant outcome, since patients may tolerate a non-functioning implant using a wrist brace or by avoiding high demand activities. In our study, three patients were unable to perform certain activities because of wrist complaints and four other patients used a wrist brace on a regular basis.
The absence of physical examination to determine range of motion and implant stability is a limitation of this study. However, we think assessment of the performance of the revisional implant in daily life is a more important indicator of outcome in these cases. PROMs were used to assess wrist function and to compare our data with data reported in the literature. The absence of preoperative PROMs makes it impossible to demonstrate improvement of wrist function, which is another limitation of our study. The PRWHE scores found in our patients (53/100) are slightly better than in the revision TWAs described by Pinder et al. (2018) (61/100), but worse than the PRWHE scores found in our patients with primary Universal 2 implants (24/100 and 42/100) (Ferreres et al., 2011; Pfanner et al., 2017). The QuickDASH scores (47/100) were quite similar to those reported by others (46/100 and 49/100) (Badge et al., 2016; Pfanner et al., 2017). Most patients would choose the procedure again and would recommend it to other patients, and all four patients with a total wrist arthrodesis of one wrist and a Universal 2 implant in the opposite wrist preferred the Universal 2 implant. The discrepancy between the moderate PROM scores and the high patient satisfaction, plus the fact that no wrist problems were experienced in 16 of the 23 implants, may be explained by other problems of the affected limb, like rheumatoid arthritis in other joints. Another weakness of this study is its retrospective design with a high number of dropouts (17 of the 57 implants).
We hypothesized that failure of Universal 2 implants could be predicted by the degree of periprosthetic osteolysis before revision, but this could not be confirmed.
Loosening of the distal component remains a major problem in revision implants. In our opinion, a revision system that provides less stress on the carpal fixation points might give better results and avoid failures. The polyethylene component of the Re-motion implants (Stryker, Kalamazoo, MI, USA) permits a rotational articulation of 20° with the carpal plate. We believe this reduces stress on the carpal fixation points. For this reason, we have been using the Re-motion implant as salvage procedure for failed BIAX implants since 2015.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.