
Abstract
In health, humans spend approximately one-third of their lives asleep. Sleep involves all organ systems, and it is an inherent mechanism for regulation and optimisation of bodily functions. Critical illness commonly results in a wide range of adverse health outcomes, many of which may theoretically be ameliorated by functions that are enhanced by sleep. Sleep deprivation and its subsequent organ dysfunction leads to muscle weakness, immunocompromise and the cardiovascular changes of the stress responses; these features are common features of critical illness and its sequalae. Sleep is reframed as an inherent mechanism for recovery and repair and a key mechanism for improving critical care outcomes. An understanding of how sleep affects our patients could lead to novel therapies that would enhance their recovery. This review covers sleep physiology, measurements to assess it in the critically ill, common pathological features that impact sleep during critical illness and the logical interventions and areas for research that might optimise sleep related outcomes.
Introduction
Sleep is a normal, rapidly reversible, recurrent state of reduced responsiveness to external stimulation, accompanied by complex but predictable physiological changes. 1
Humans, in common with all endotherms, are obliged to sleep. While the duration and distribution of sleep architecture changes with age and sex, it is a function that is essential to health, and which takes up approximately one-third of our lives. 2
The functions of sleep are known from observational studies in healthy animals and humans. Sleep deprivation studies, where a clinical outcome or biomarker is measured in rested or sleep deprived subjects, are used to infer the functions of sleep or generate hypothesise of function that can then be tested.
Sleep deprivation is associated with increased neuropsychiatric, cognitive, cardiovascular, respiratory, immune function and endocrine system adverse effects.3,4 In the critically ill, it is also associated with poor glucose control, an increased length of hospital stay and increased mortality.5–7 Improving sleep is may therefore be associated with improved outcomes from critical illness, making sleep physiology and methods of altering it important targets.
Sleep deprivation is associated with delirium, which it has a bidirectional relationship with, however teasing out causality or association between sleep and delirium is illusive. 8
More broadly, it is universally accepted that sleep deprivation is disliked, making preservation of sleep a humanitarian act. While there is no legal definition of sleep deprivation, ‘persons subjected to sleep deprivation as a form of torture have no agency and no ability to modify their environments or habits to ensure sleep’. 9 Necessary clinical interventions within the ICU have a significant impact on sleep quality, and if left unmitigated, may be seen as cruel, or lead to significant harm.
Measures to improve sleep and hence improve health outcomes encompass environmental modifications, behaviours and in some cases medications, but significantly effective interventions are lacking for the critically ill. 10
This narrative review aims to give an overview of the normal physiology of sleep, its relevance to critical illness and to identify potential physiology based therapeutic targets that will improve sleep and therefore critical illness outcomes.
Literature search
A narrative review of the literature was performed. Relevant articles were identified by searching the EMBASE, MEDLINE, Ovid and Prospero databases. Search terms included ‘critical illness’, ‘intensive care unit’ ‘sleep’, ‘sleep disturbance’, ‘circadian sleep disorder’, ‘health outcomes’, ‘inflammation’, ‘Sleep physiology’, ‘ICU environment’, ‘Sleep measurement’, ‘Critical care AND Patient experience’ and ‘sleep interventions’. Studies varied in size and included clinical studies with patients, healthy volunteers and with laboratory studies where relevant. Clinical guidelines and expert consensus statements were included and their references considered for inclusion.
Sleep physiology
Sleep induces changes in multiple organ systems and can be measured both objectively and subjectively. When measured objectively, sleep can be seen to follow cycles, divided into distinct stages. Normal sleep shows cycles based on polysomnography and clinical observations which are summarised in Table 1. Each 4 stage sleep cycle will pass through these stages 4–5 times per night, each complete cycle taking 90–100 min. 11
Simplified America Academy of Sleep Medicine stages of sleep or sleep architecture.
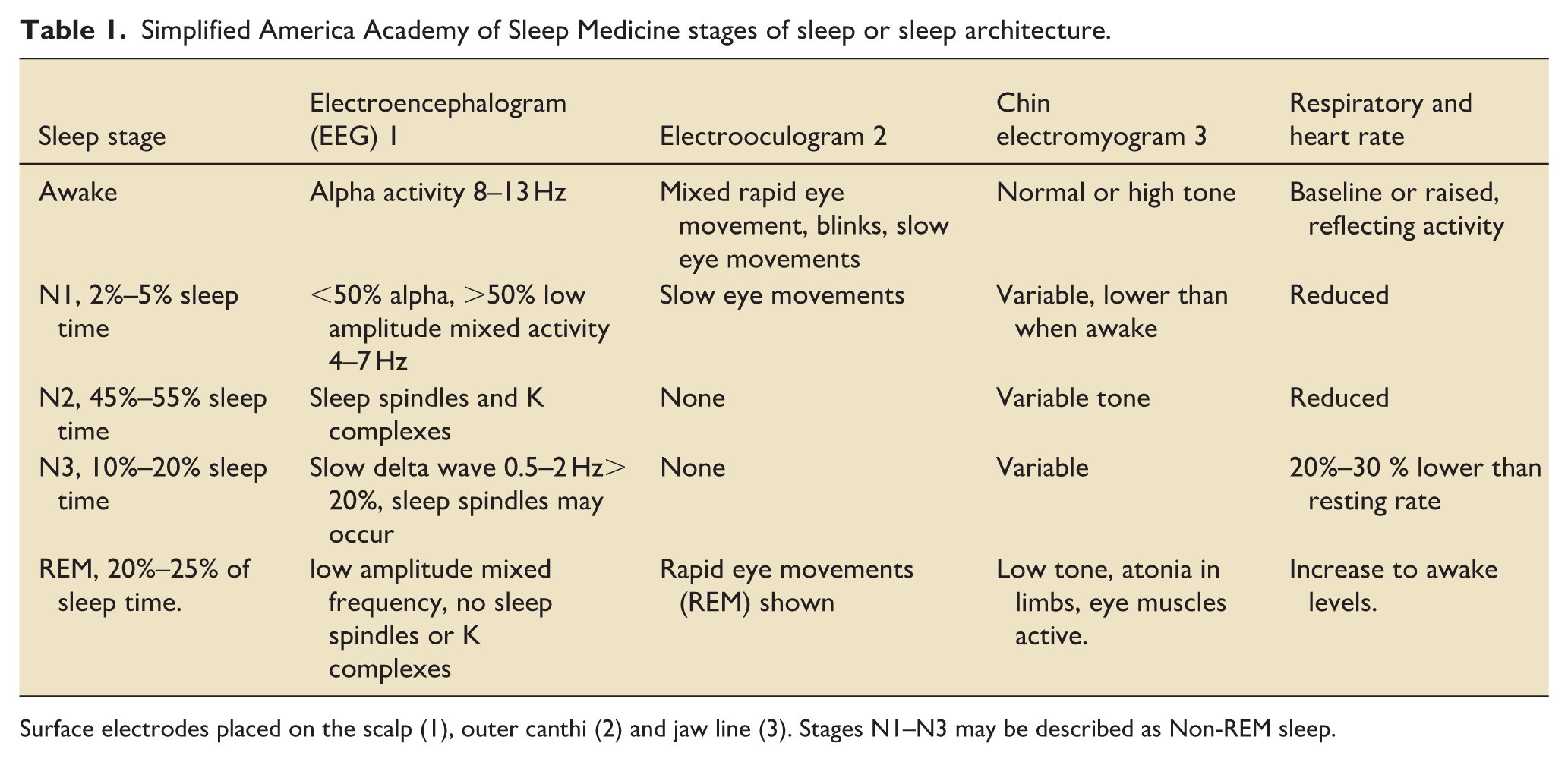
Surface electrodes placed on the scalp (1), outer canthi (2) and jaw line (3). Stages N1–N3 may be described as Non-REM sleep.
In the elderly, there is less stage N3 sleep and more stage N2 sleep (see Figure 1), with more nighttime awakenings and sleep fragmentation. 12 The reduction in slow wave activity is most likely linked to cortical atrophy in medial and pre-frontal cortex. 13
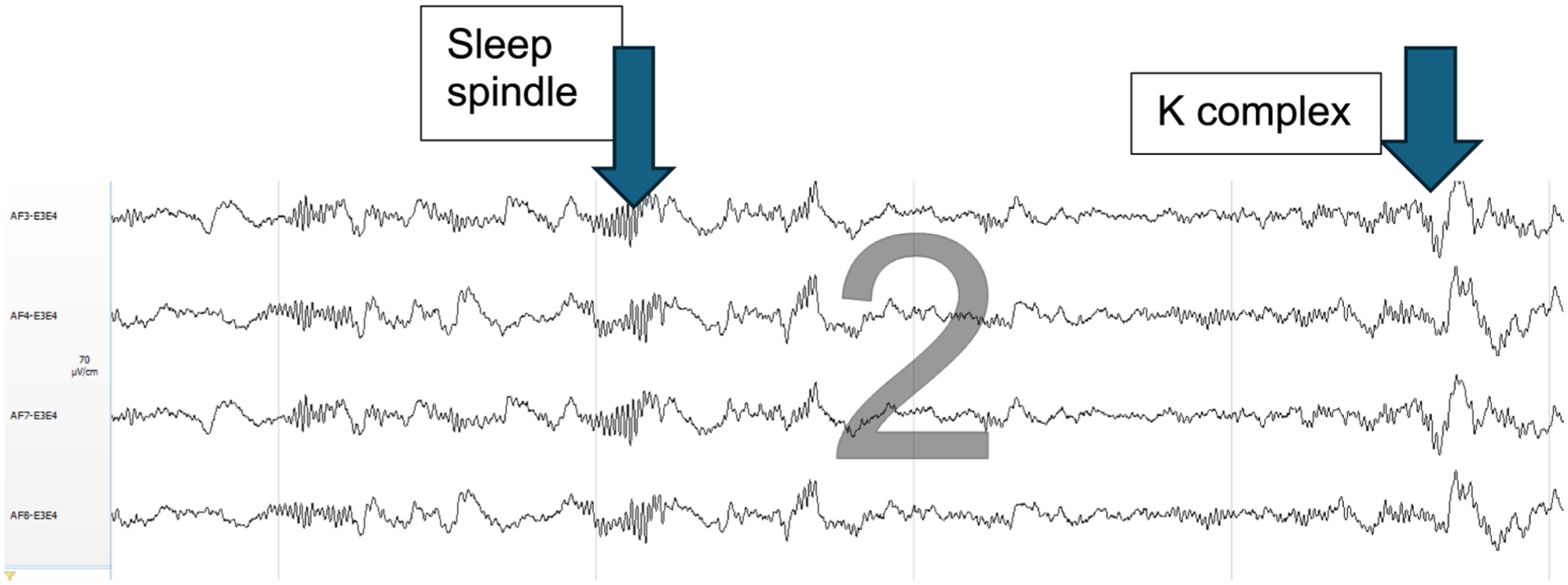
N2 sleep.N2 sleep with sleep spindle and K complex taken during sleep study (with thanks to Dr I Crossingham).
Sleep duration and deprivation
The optimal duration of sleep for health varies with age, sex and across individuals. Sleep deprivation may be called total when a whole night’s sleep is lost, partial when a normal sleep time is prevented, or selective, when a specific stage of sleep is prevented. 12 There is no definition for sleep deprivation during critical illness. Specific stages of sleep have health implications, which will be covered within this article.
Investigations for sleep
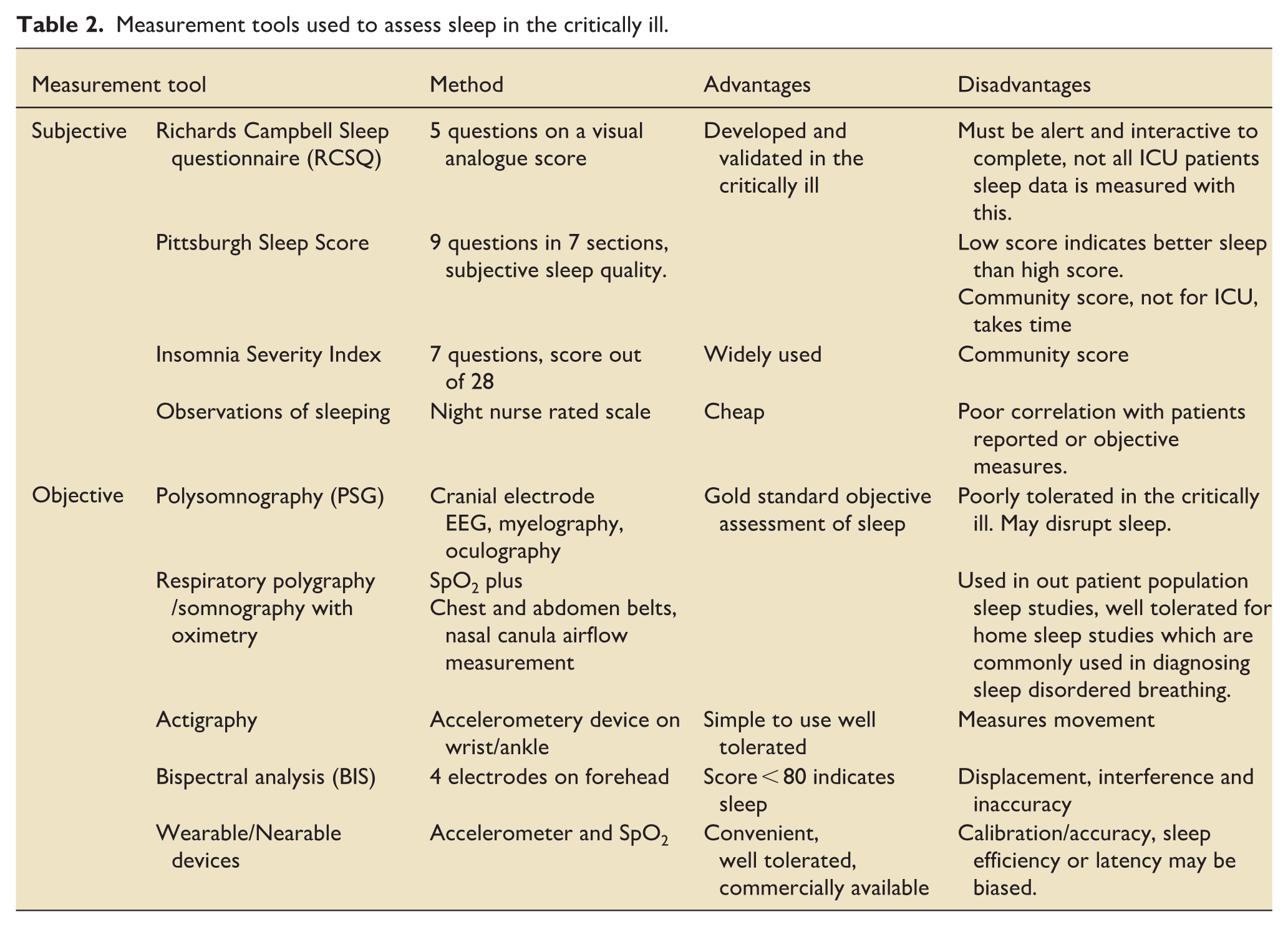
Measurements affected by sleep are either subjective (patient or observer rated scoring systems) or objective, where polysomnography (PSG) is seen as the gold standard. 11 Sleep monitoring in ICU is not currently recommended and is limited by a lack of a monitor that is both accurate and well tolerated in this cohort. A summary of sleep investigations and their clinical application in relation to the critically ill are given in Table 2.
Measurement tools used to assess sleep in the critically ill.
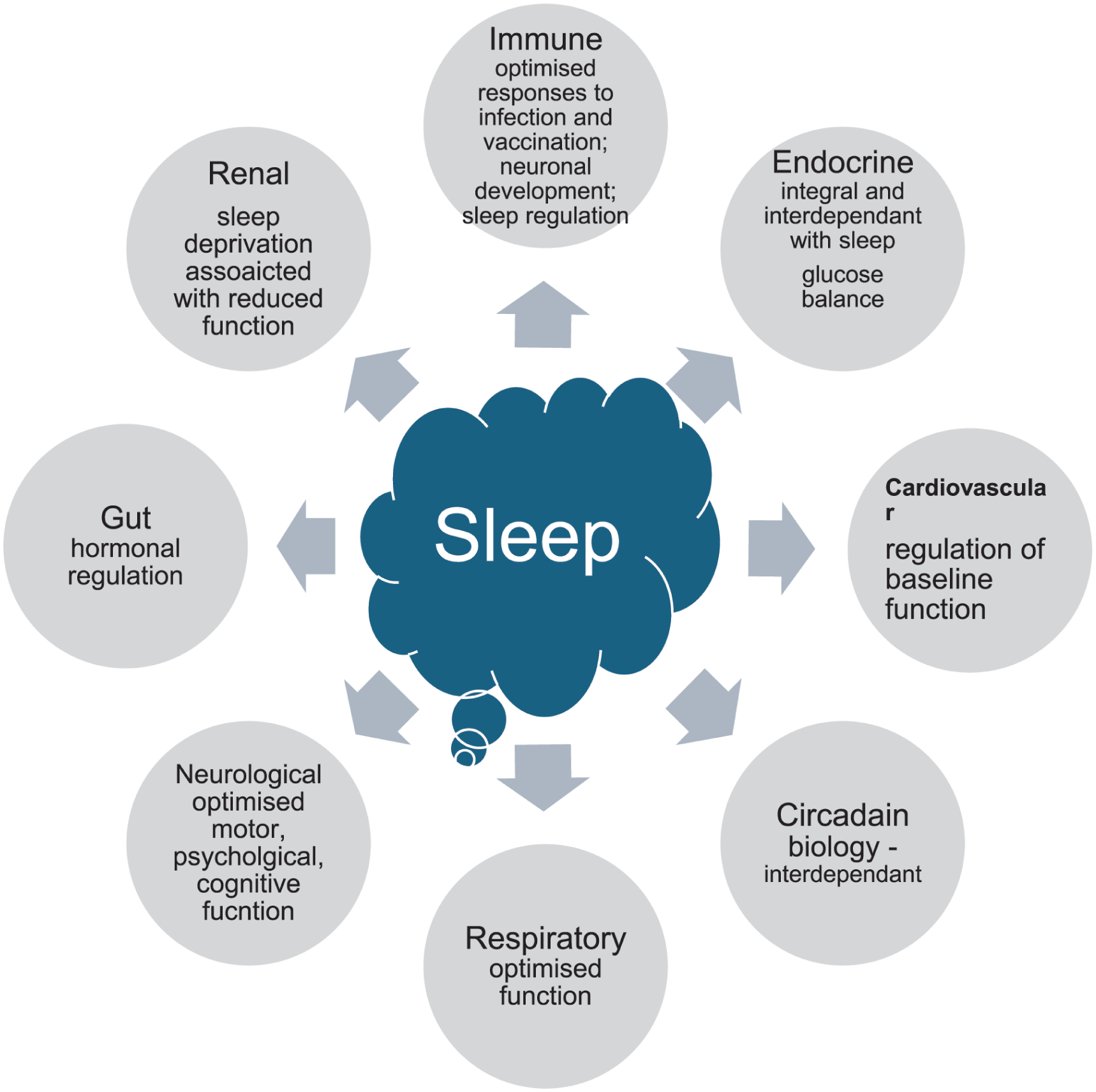
Sleep and organ system function
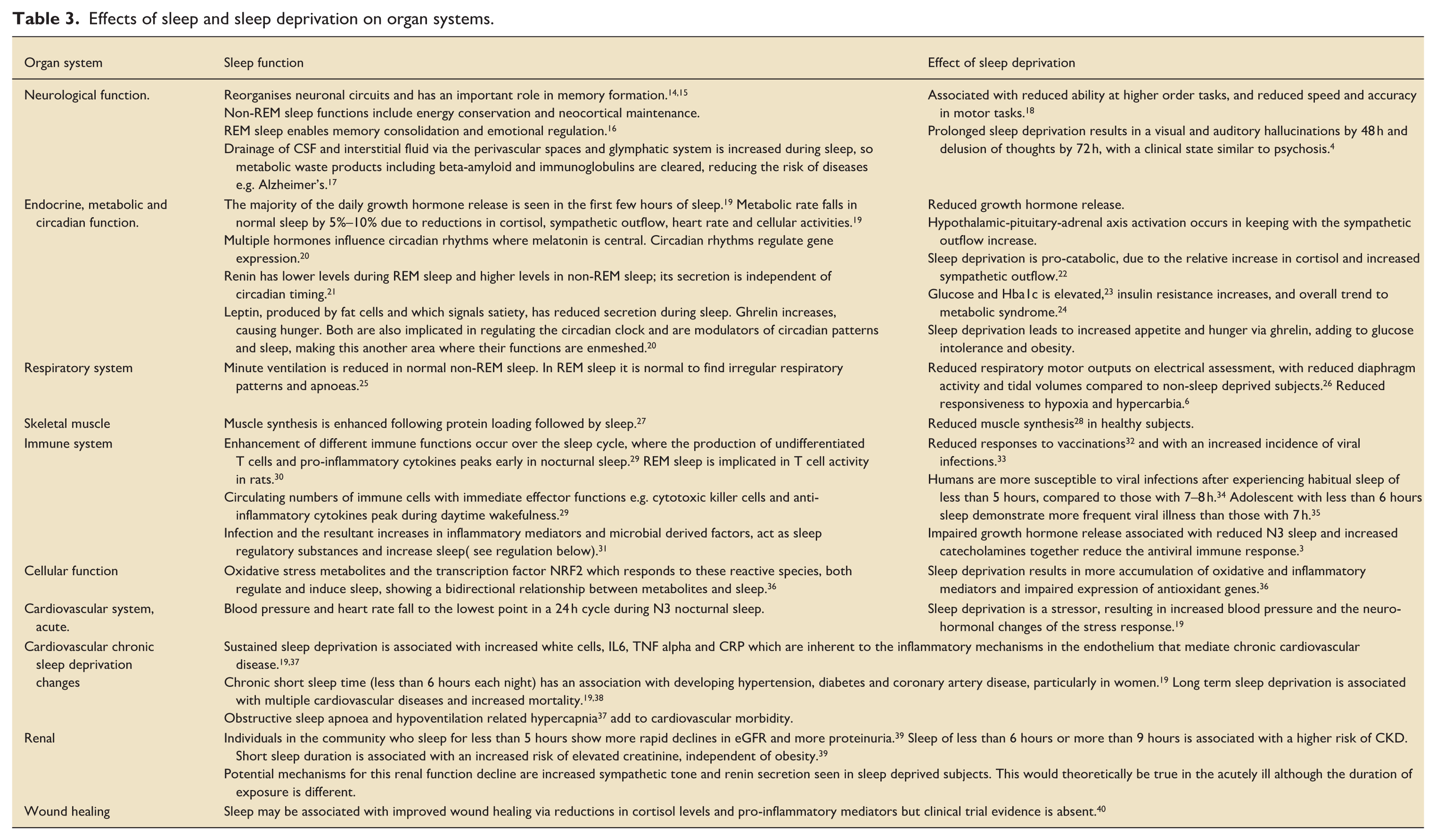
All organ systems are affected by and influence sleep. A summary of the key effects of sleep and sleep deprivation on each system is in Table 3 and summarised in Figure 2. While there are multiple effects on all organ systems, some are of particular significance to the critically ill. Sleep deprivation is associated with a delay in higher cortical functions which is compounded by delirium and hallucinations. It is associated with reduced muscle synthesis, reduced motor inputs to the respiratory system and blunted responses to hypoxia and hypercarbia, all of which may impair weaning from mechanical ventilatory support. The associated impairment of immune function compounds the risk of secondary infection, all of which may contribute to an increase length of ICU stay and prolonged rehabilitation time following sleep deprivation.
Effects of sleep and sleep deprivation on organ systems.
Effects of sleep on organ function.
Regulation of sleep
The circadian clock and sleep homeostatic processes both influence the sleep-wake cycle, which in turn reinforces both these mechanisms.
The homeostatic drive to sleep, or sleep pressure, acts in an additive fashion to circadian fluctuations. Cellular metabolites and immune mediators influence homeostatic processes. Social timing also influences sleep timing, which may be in conflict with physiological sleep mechanisms. 14 This relationship is summarised in Figure 3.

Summary of sleep regulation.
The circadian clock
This reinforces daytime wakefulness, responding to external signals principally photic stimulation of retinal receptors. 15 Co-ordinated in the suprachiasmatic nucleus, it acts via the pineal gland and regulates the secretion of melatonin which initiates sleep, influences gene expression and also influences the secretion of cortisol, prolactin and growth hormone and body temperature fluctuations. 15 Serotonin is a precursor of melatonin synthesis and acts to potentiate melatonin secretion. Environmental factors of social interaction, activity and eating with a resultant change in hormones, also entrain the circadian rhythm. 16
The homeostatic sleep process (or sleep debt, or sleep pressure)
This is driven by depletion in glycogen and accumulation of adenosine in the forebrain, which disinhibits the ventrolateral preoptic nucleus and inhibits the reticular activating system, and so causes sleep. 17 The accumulation of adenosine acts also on Adenosine 2a receptor agonists on sleep-active neurones, as well as inhibiting Hcrt/Ox neurones (hypocretin/orexin). 18 Oxidative cellular stress products (NRF2) also add to sleep pressure and enhance the drive to sleep. 19
Infection (acts via homeostatic sleep processes)
The resultant increases in inflammatory mediators and microbial derived factors, act as sleep regulatory substances and increase sleep. 20 Injection of low dose IL-1beta or TNF alpha promotes NREM sleep and inhibition of these mediators inhibits sleep. 21 In addition, TNF alpha has a role in brain plasticity making it a central mediator in neuronal activity, connectivity and sleep. In patients with rheumatological disease and inflammation who take TNF alpha antagonist agents, nocturnal sleep quality is improved.21,22
Critical illness and its impact on sleep
Critical illness results from a heterogenous range of diagnoses, in patients with variable age, comorbidities, duration of illness and treatments. However, the critically ill are unified by being cared for in a shared environment (the Intensive Care Unit, ICU), with common treatments and common pathophysiological responses to critical illness.
Environment
Nocturnal sound
Delivering high level care in ICU is associated with sound levels that disrupt sleep. 23 Multiple observational studies have demonstrated that sound and light levels in ICU environments are greater both day and night than WHO recommended limits for health care environments.24–26 Sound measurements in 5 UK ICUs demonstrated that average sound levels in 24 h were over 51 dBA, significantly above the WHO recommended maximum of 35 dBA, with the lowest sound levels at 4 am. The highest number of sound peaks over 100 dBA (about the same volume as a pneumatic drill) coincided with handover and ward rounds, being 2 peaks per hour. 27 The WHO recommendation of 40–45 dBA at night is under the 55 dBA volume of normal conversation. In a single centre observational study, the impact of staff voices and activities was found to account for more than half of the acoustic energy, with alarms and device operation noise being a lesser contributor to both the acoustic energy and the predicted loudness peaks. 28
Nocturnal light
Levels are commonly high, and a high illness severity (SOFA score) correlates with more light exposure. 25 Simple measures to reduce light and sound exposure in the critically ill (e.g. eye masks and ear plugs) have been demonstrated to have a positive impact on PSG sleep measurements, however most work is from small single centre studies of less unwell patients. 29 Nocturnal sound and light events, as well as physically stimulating experiences (tracheal suctioning, turning, assessments) fragment sleep architecture, leading to sleep deprivation and incomplete sleep cycles. 23
Common treatments
Mechanical ventilation
Interactions with the ventilator and the effects of different modes of ventilation on sleep have been studied, but a unifying pattern in the effects on sleep separate to that of critical illness is not clear. 12 In a prospective randomised study of 35 patients, assist control ventilation was associated in more nocturnal sleep with improved sleep architecture compared to pressure support ventilation, 30 supporting the concept of nocturnal ventilator ‘rest’ being beneficial. However, research to demonstrate benefit from adaptive ventilator modes at night on sleep are currently absent. In patients who are judged to be ready to wean from the ventilator, those with atypical sleep, lack of REM or slow wave sleep were more likely to fail than those with normal sleep patterns. 31 Non-invasive ventilation may provide a benefit to patients with delayed rehabilitation that show persistent poor sleep quality, daytime somnolence and type 2 respiratory failure. 32
Drugs and their effect on sleep
To tolerate endotracheal tubes, invasive procedures and painful conditions, sedation and analgesia are used. Propofol, benzodiazepines and other GABAergic drugs are associated with increase N2 sleep, decrease N1, N3 and REM sleep and more delirium, 33 which increases the risk of more disordered sleep. 34 High dose steroids are used in a wide range of pathologies and these directly impair circadian regulation and sleep architecture. 35 Opioids reduce N3 and REM sleep, 36 and induce sleep disordered breathing 37 which may lead to hypoventilation and poor progression in weaning or rehabilitation.
Antidepressants commonly reduced REM sleep, the exceptions to this being agomelatine (a melatonin agonist), bupropion, trazodone (insomnia is an off-label indication for its use), and the more commonly used mirtazapine 38 which increases somnolence in lower doses where the antihistamine effect is greatest.
Pathophysiological responses to critical illness
The stress response
Increase systemic effects of catecholamines and cortisol, leading to increased glucose levels, decreased insulin secretion, insulin resistance and a pro-catabolic state are all common with critical illness. 39 These changes will affect sleep regulation and prevent sleep initiation. Many of the damage associated or pathogen associated molecular patterns that are involved in the pathophysiology of sepsis or systemic infection, are markers that are also fundamental to sleep modulation, for example, TNF alpha, IL1, IL8. This means systemic infection will impair sleep regulation and cause sleep deprivation, which in turn adds to more of the stress response. 12 Sleep deprivation impairs innate and adaptive immunity, making sleep deprivation a risk factor for hospital acquired infection, prolonged inflammation and catabolism.
Delirium
Delirium is common during critical illness with multiple risk factors, notably increased illness severity, age, use of opiates and sedative, presence of infection, APACHE-II score and urea concertation. 40 The relationship between delirium and sleep appears to be bidirectional, and it may be that delirium is an extension of disordered sleep given the frequent association of the two and the difficulties in demonstrating a causative relationship. 41 Given that sleep deprivation leads to a psychosis like state in healthy subjects, and sleep is known to be fragmented and atypical in the critically ill, it is likely that impaired sleep contributes to the aetiology of delirium. Key risk factors for delirium are the sedative and analgesic drugs used in critical care, which all effect sleep by changing the ratio of N2 to N3/REM sleep. Abnormal sleep may be the key mechanism by which sedatives and analgesics are implicated in delirium.
Sleep during critical illness
It is common for the critically ill to be sleep deprived, with more sleep fragmentation, loss of REM and N3 sleep.31,42 The total sleep time may be preserved, with an increased in daytime sleeping. 41 Patients with a disappearance of REM sleep are more likely to require reintubation or prolonged weaning than those who demonstrate persistent REM sleep . 6 Patient identified factors that disrupt sleep are multiple, where noise, light, pain, discomfort, anxiety, nocturnal interventions including repositioning, procedures, assessments and out of hours admissions are common factors.7,41
Long term effects following critical illness
Patients in the recovery periods after critical illness may exhibit a persistent inflammation, immunosuppression and catabolism syndrome, which contribute to adverse long term outcomes. The cause of inflammation-immunosuppression and catabolism syndrome is unclear, with evidence that altered myelopoiesis, reduced T cell function and expanded immature myeloid derived suppressor cells are contributory. 43 Sleep deprivation is recognised to be associated with all of these features, making it a likely contributor to post critical illness morbidity.
Proposed sleep mediated methods of changing critical illness outcomes
Using the known effects of sleep on organ function and the specific disruptors of sleep in the critical care environment, logical physiological targets for enhancing the inherent benefits of sleep can be identified. This is summarised in Figure 4. physiological targets for improving sleep in the critically ill.
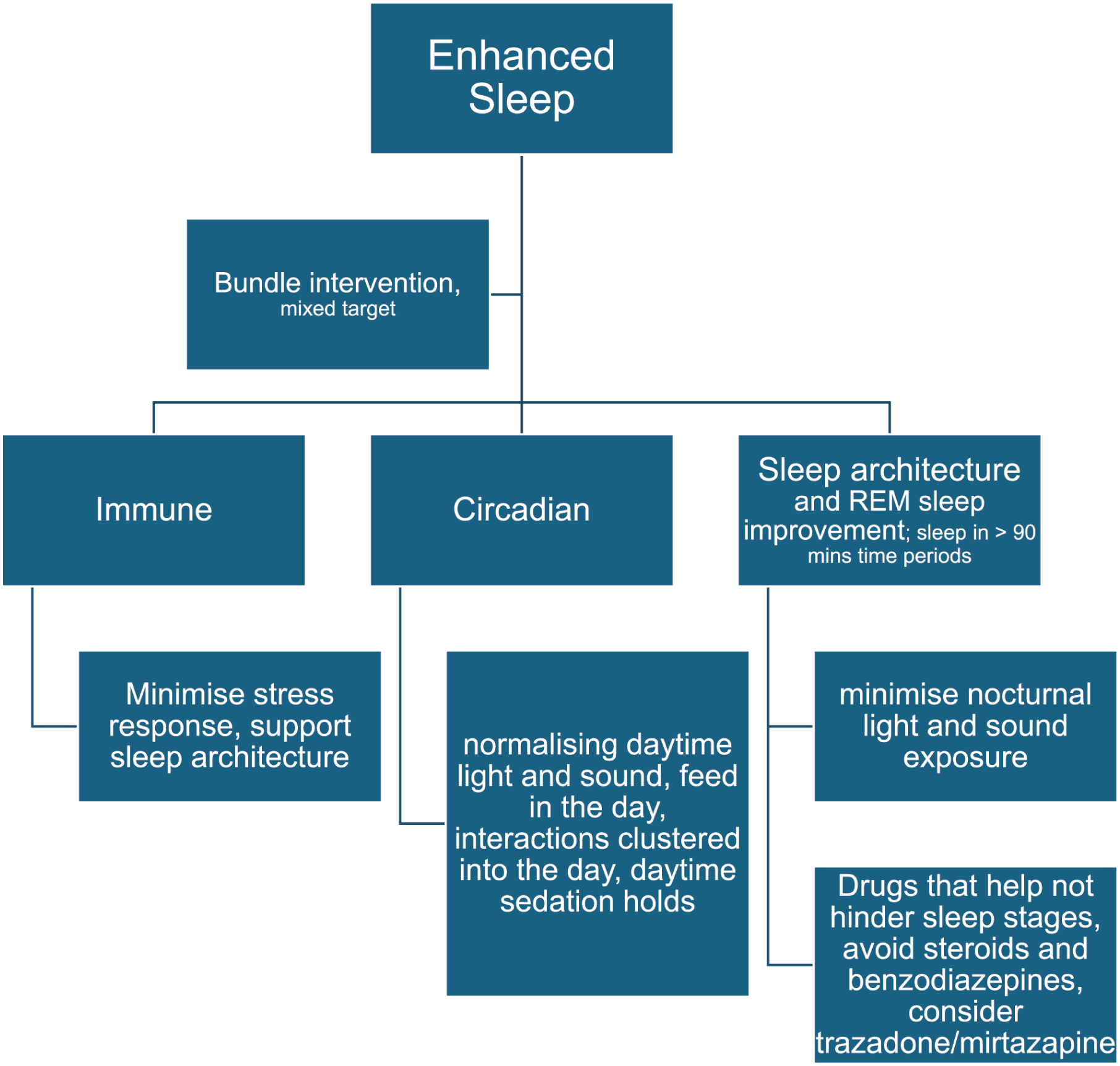
Physiological targets for improving sleep during critical illness.
Minimising disruption to sleep architecture
Theoretically, allowing uninterrupted progress through all stages of sleep (e.g. minimum 90 min with no interruption) would improve immune function, endocrine function and potentially limit muscle wasting. In this time period, a squeaky wheel every 30 min preventing adequate N3 and REM sleep is theoretically an immunosuppressant and hence a health hazard.
Enhancing REM sleep
The heightened loss of REM sleep in this cohort has implications specifically for memory formation, emotional regulation and T cell function.44,45 REM sleep is distinctive in that observational healthy volunteer work implies that it may only be regained if sufficient equivalent time is spent in REM sleep during recovery.46,47
Nocturnal sound exposure minimisation
White noise or specific sounds (ocean waves) have been assessed with improved initiation of sleep 48 ; earplugs and eye masks are associated with inconsistent results across studies with poor quality evidence to support their use. 34 These interventions were not found to be universally acceptable to ICU patients. Sound reduction interventions including soft-close bins and doors have been implemented in the critically ill, with some evidence to support improved sleep. 29
Clustering care
Methods of performing care activities clustered together overnight, are theoretically beneficial but strong evidence on its effects on sleep is not available.34,49
Drug choice
Minimising the use of sedatives that interfere with N3 and REM sleep would be beneficial. The introduction of new agents may hold promise. Steroids, particularly in high doses and given nocturnally are counter to normal sleep physiology and are disruptive to sleep regulation, sleep architecture and endocrine regulation of other organ function. They remain in clinical use until alternative agents are identified.
Drugs to enhance sleep
No known drug can initiate and maintain normal sleep. Zolpidem and zopiclone (‘z’ drugs) or anti histamines may have a place in the critically ill for short term relief of insomnia. 50
Melatonin and Ramelteon, which may induce circadian phase shift, have been extensively studied in the critically ill with outcomes of both sleep and delirium, where some single centre studies show benefits on subjective sleep, but with no compelling evidence for benefit.49,51 The sleep effects of Melatonin are likely negated through environmental and physiological impediments to good quality sleep in ICU, but there is theoretical benefit to its antioxidant and anti-inflammatory properties. The optimal dose for sleep in the critically ill warrants further investigation and it remains a drug recommended in ‘Prevention and Management of Pain, Anxiety, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU’ (PADIS) guidelines. 52
Dexmedetomidine has been studied in the critically ill, with outcomes of delirium and sleep. It produces a state that preserves N2 and N3 sleep, and it remains a drug of interest. 36
In community populations, Mirtazapine reduces insomnia, although its effects wane over time, and withdrawal from the drug after long term use may induce insomnia. 53 Its use has not been studied in the critically ill.
Circadian interventions
Nocturnal light and sound exposure minimisation
Daytime light exposure is normal and important for circadian health, where nighttime light exposure will be disruptive to both sleep architecture and circadian health. Interventions to reduced nocturnal light exposure in the critically ill have been studied, but there is no strong evidence as to its efficacy in improving sleep or circadian patterns. 54 Reductions in the frequency of high decibel sound events would also aid circadian health in addition to allowing normal sleep architecture.
Feeding
Providing daytime only feeding has been studied in the critically ill, 55 but its effect on sleep related health outcomes is not known.
Touch and social interactions
Theoretically physical examination, physical care and having visitors are also circadian influencers and so should be kept to daytime as much as is possible.
Immune interactions
Improving sleep, so enhancing immune pathways may result in reduced secondary or hospital acquired infections and reduced morbidity and mortality. Immunomodulation in the critically ill is far from simple with no single target. Enhancing sleep may be significantly more effective, with less adverse effects and cost than attempting to enhance aspects of the immune response with drugs.
Bundle interventions
A grouped sleep intervention or bundle, that addresses multiple aspects of care that affect sleep, has potential for benefit. Interventions of interest are light and sound exposure, feed timings, care timing and drug selection to enhance sleep. 49 A lack of strong evidence for each aspect, with methodological and implementation challenges for bundle studies limits this approach.
Research
There is a striking similarity in the physiological responses to critical illness and sleep deprivation. Studies that compare outcomes between patients with and without sleep deprivation would aid in understanding how much commonly experienced critical illness morbidity during and after the acute phase is in fact due to sleep deprivation.
Evidence for what interventions to use are limited by lack of high quality studies with patient-based outcomes. Important research questions are
What measurements of aspects of sleep are both acceptable to patients and provide accurate information?
How should sleep deprivation in the critically ill be defined?
What are effective, pragmatic methods of improving sleep quality and quantity during critical illness?
Does improving sleep lead to specific health outcomes? For example, reduced infection, wound healing, renal function, reduced sequalae of delirium, time to wean from the ventilator or improved recovery and muscle strength.
What is the most appropriate method of dosing nocturnal melatonin for the critically ill in relation to sleep quality and quantity? (as supported by PADIS guidelines.) 52
Appropriated methods of evaluating the efficacy of interventions for sleep may include innovative methodologies and multivariate analysis of multiple endpoints. Observational work that has previously been form single centres may be improved on by future collaborations within research networks.
Conclusions
Normal sleep physiology enables multiple inherent health functions that are of theoretical benefit to the critically ill. Specific health benefits of value are improved immune function and hence reduced secondary infection, potential reduction in the sequalae of delirium, reducing loss of muscle mass with benefits for rehabilitation, reductions in stress response hormones and so less cardiovascular and immune complications. This makes sleep optimisation a target for improving outcomes from critical illness. Studies of effective interventions to enhance sleep with primary outcomes that are of value to patients are awaited.
Footnotes
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: I am the deputy editor in chief. Other members of the editorial team handled this submission and I am blinded to the reviewers identification and review process.