
Abstract
Background:
Early mobilisation of critically ill patients remains variable across practice. This study set out to determine barriers to and facilitators of early mobilisation for patients diagnosed with delirium in the intensive care unit (ICU).
Methods:
A mixed-methods descriptive systematic review. Electronic databases (AMED, BNI, CINAHL Plus, Cochrane Library, Medline and EMBASE) were searched for publications up to 22nd December 2021. Independent reviewers screened studies and extracted data using Covidence Systematic Review Management software. Data were summarised according to frequency (n/%) of barriers and facilitators. Thematic analysis of qualitative studies was carried out in order to address the secondary aim. Quantitative studies were assessed using the GRADE quality assessment tool. Qualitative studies were analysed according to the GRADE-CERQual quality assessment tool. This study was prospectively registered on PROSPERO (CRD 42021227655).
Results:
Ten studies met the inclusion criteria. Quantitative findings demonstrated the presence of delirium was the most common reported barrier to early mobilisation. The most common facilitator was ICU staff experience of positive outcomes as a result of early mobilisation interventions. Thematic analysis identified six main themes that may describe potential meanings behind these findings: (1) knowledge, (2) personal preferences, (3) perceived burden of delirium, (4) perceived complexity, (5) decision-making and (6) culture.
Conclusion:
These findings highlight the reported need to further understand the impact and value of early mobilisation as a non-pharmacological intervention for patients diagnosed with delirium in ICU. Evaluation of early mobilisation interventions involving key stakeholders may address these concerns and provide effective implementation strategies.
Introduction
Delirium is defined as an acute disturbance in attention and cognition that can develop over a short period of time and fluctuate markedly from day to day. 1 There are a number of diagnostic tools to identify delirium, the most valid and sensitive used in the intensive care unit (ICU) are the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) and the Intensive Care Delirium Screening Checklist (ICDSC). 2 Additionally, the Delirium Motor Subtype Scale classifies delirium into three main subtypes: hyperactive, hypoactive and mixed delirium. 3 Evidence suggests up to one-third of patients admitted to an ICU develop delirium. 4
A systematic review and meta-analysis identified patients diagnosed with ICU-delirium are more likely to die during their hospital admission, have increased length of mechanical ventilation, increased ICU and hospital stay as well as developing poor long-term cognitive outcomes such as executive function and memory impairments. 4 Furthermore, evidence suggests an increased hospital mortality rate (35%) for elderly, frail delirious patients in the ICU versus (10%) for non-frail delirious ICU patients. 5 A systematic review and quality assessment identified delirium is associated with substantial costs to healthcare systems. 6 Findings demonstrated substantial national (U.S., 2019) economic costs (estimated between $6.6 billion to $82.4 billion) associated with delirium. Additionally, the identified estimated costs of dementia as a consequence of delirium may account for 52% of the total costs of delirium.
Best practice guidelines advocate multi-component interventions including pharmacological and non-pharmacological management such as the ABCDEF Bundle (previously known as the ABCDE Bundle).
7
The ABCDEF Bundle comprises of the following management approaches;
Effective implementation of early mobilisation to improve outcomes for patients with ICU-delirium is a high priority. Therefore, a better understanding of the current evidence base exploring early mobilisation interventions for patients with ICU-delirium is required in order to improve implementation measures, guide future research and ultimately improve patient outcomes in ICUs.
The research aims were:
i. What are the barriers to and facilitators of early mobilisation for patients diagnosed with delirium in the ICU?
ii. What are the potential meanings behind the identified barriers and facilitators?
Method
Design
The conduct and reporting of this systematic review were guided by the Cochrane Handbook for Systematic Reviews of Interventions and Preferred Reporting Items for Systematic Reviews and Meta-analysis.18,19 A search of the Cochrane database and Prospero International Prospective Register of systematic reviews confirmed there were no related published or registered systematic reviews. The protocol for this study was registered on the Prospero International Prospective Register of systematic reviews (ID CRD42021227655).
Identification and selection of studies
A comprehensive search using the Boolean search method (see appendices) of the following electronic bibliographic databases was carried out; AMED, BNI, CINAHL Plus, Cochrane Library, Medline and EMBASE. No restrictions were placed upon the search including language and publication period. Translation tools were utilised for non-English texts and a non-professional volunteer translated texts published in Mandarin. The initial search was carried out on 14th of January 2021. The search was re-run on the 22nd of December 2021 prior to final analysis of included studies. The reference list of one meta-synthesis of qualitative evidence 20 was screened for any additional citations.
Covidence systematic review management software was used to store references, complete screening including removal of duplicate studies and data extraction. This allowed the reviewers to work independently. Two reviewers (JB, CM) completed screening of all study titles and abstracts, full texts and data extraction. A third reviewer (SKM) assisted the screening processes where there were any disagreements. A pilot of the screening process for 100 studies was completed by both independent reviewers prior to commencing the initial search.
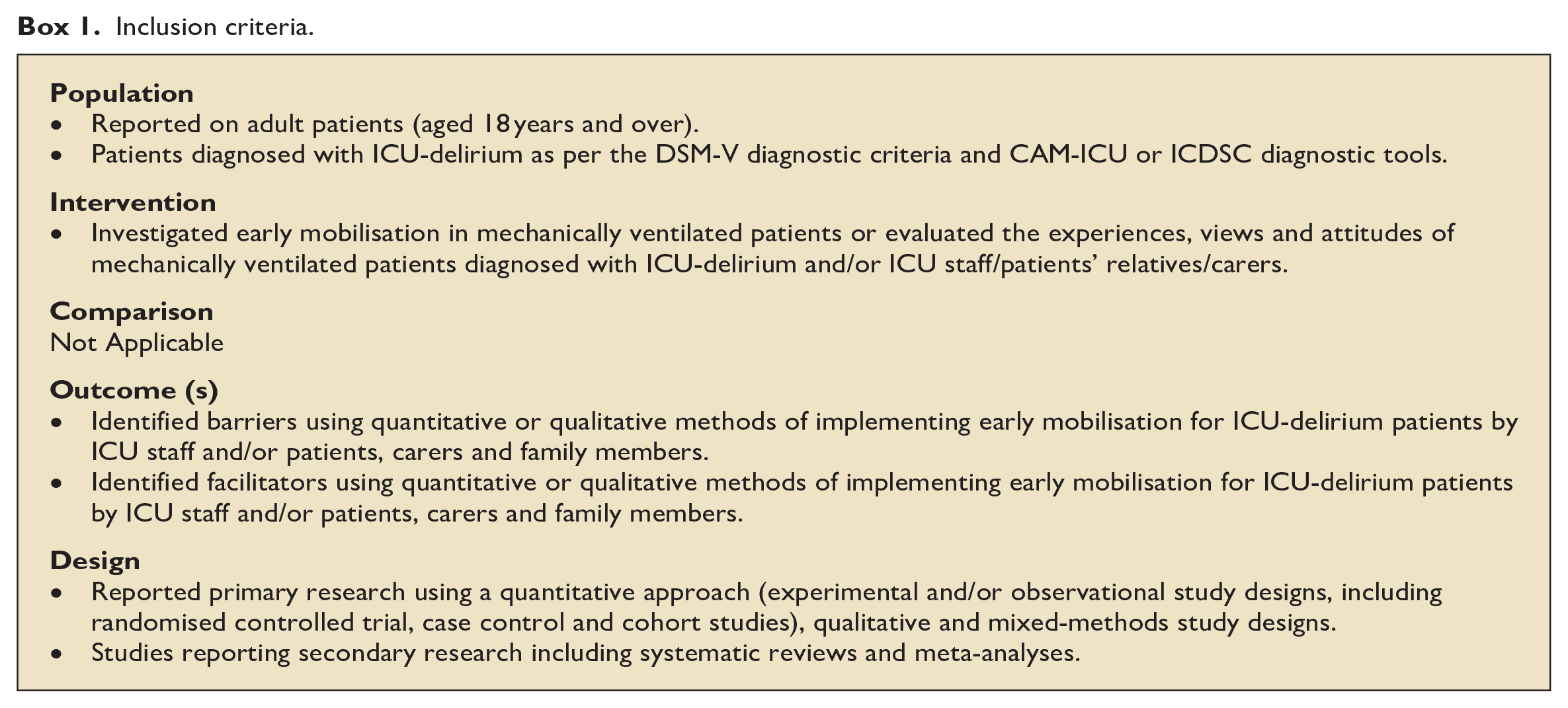
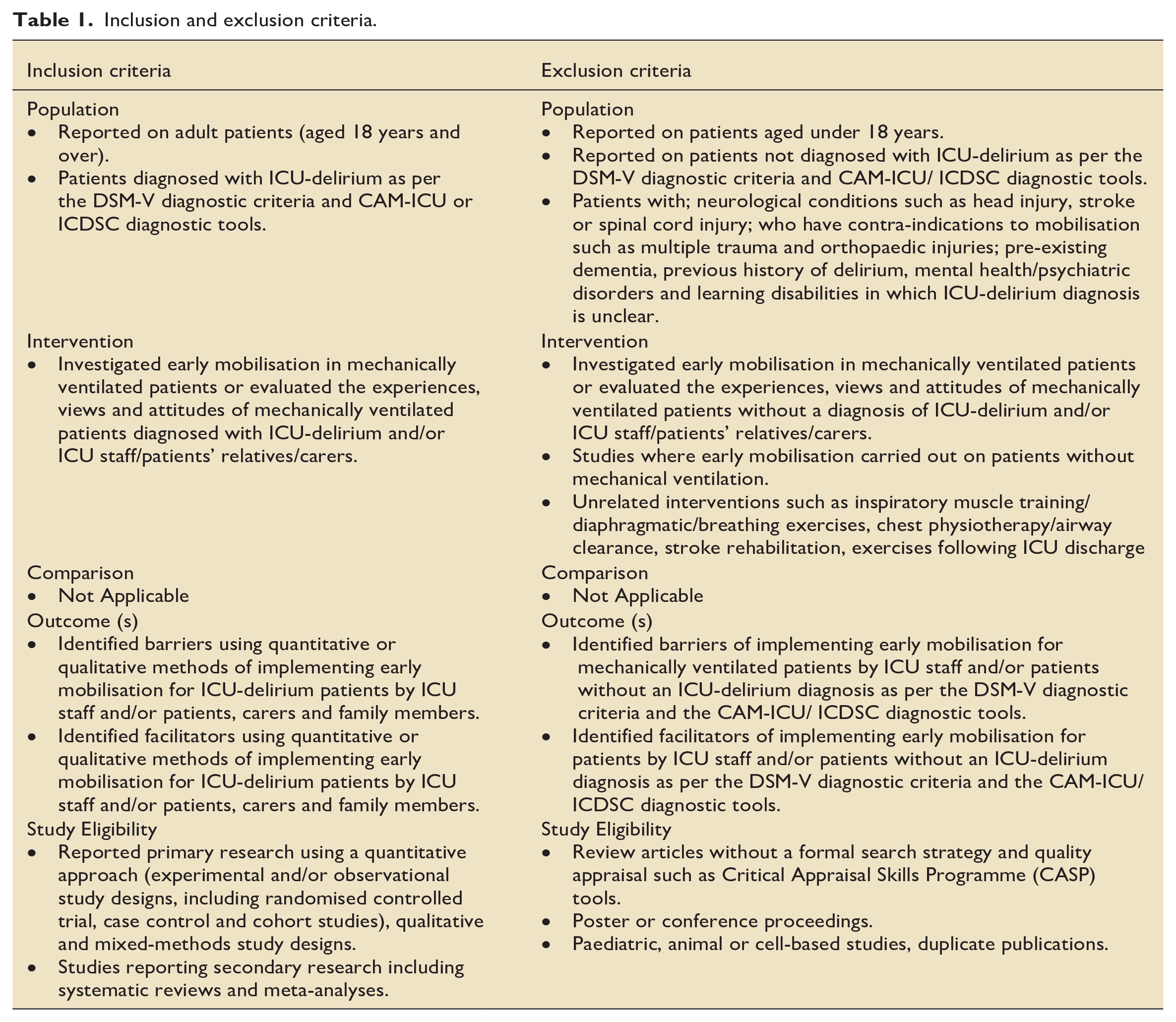
The Population, Intervention, Comparator, Outcome and study design (PICO) format guided study selection criteria (Box 1). 21 There was no comparator for this systematic review in order to address the review question and study aims. Therefore, no effects of intervention were measured. Consequently, this systematic review included a descriptive analysis of the included quantitative and qualitative studies. All study designs were deemed appropriate. See Table 1 for inclusion and exclusion criteria.
Inclusion criteria.
Inclusion and exclusion criteria.
Assessment of study characteristics
Data extraction of study characteristics (see Table 2, appendices) was independently completed by two reviewers (JB, CM). The reviewers (JB, CM) met mid-way and at the final stages of this process to discuss consensus of the data extracted for each study.
Quality Assessment
Quantitative studies were assessed using the Grading of Recommendations Assessment, Development and Evaluation GRADE Handbook. 22 Qualitative studies were assessed according to the Confidence in the Evidence from Reviews of Qualitative Research GRADE-CERQual tool. 23 The methodological limitations component of the GRADE-CERQual was assessed using the Critical Appraisal Skills Programme (CASP) checklist for qualitative research. 24 The CASP tool has been identified as the most common quality appraisal tool used for this component of the GRADE-CERQual. 25
Precision of intervention was not assessed because there was no comparator to determine the effectiveness of interventions. Quality assessment of included studies was completed by one reviewer (JB) using Microsoft Excel, discussed and checked for accuracy by a second reviewer (CM) and a member of the research team (RA).
Data analysis
Findings from the included studies were summarised according to frequency (n/%) of barriers and facilitators. To address the secondary aim, thematic analysis was carried out for the included qualitative studies. 26 Thematic analysis involved three stages of synthesis: coding context, developing descriptive themes and generating analytical themes (figure 1, appendices). Data analysis of the included quantitative and qualitative studies were completed using Microsoft Excel. These processes were completed by a reviewer (JB) and checked by the second reviewer (CM). Furthermore, a public advisory group and a public member of the research team (RG) reviewed the thematic analysis to ensure rigour and trustworthiness.
Results
Flow of studies through the review
The initial search identified 11,142 records. Following removal of duplicates (2943), 336 records were identified as eligible for full-text screening. The reference list of one meta-synthesis of qualitative evidence was screened resulting in retrieval of one study. 20 The reviewers demonstrated a 95% agreement for the abstract screening stage and 75% agreement for the full-text screening stage. A total of 10 studies published between 2010 and 2021 were included in this review. The PRISMA flow diagram is shown in (figure 2, appendices).
Study characteristics
Five quantitative studies were included.12,27 –30 These comprised of a survey study (1), a case report (1), feasibility studies (2) and a multi-centre cohort study. The five qualitative studies20,31 –34 included focus group studies (2), semi-structured interview studies (2) and a qualitative synthesis (1). The most common reason for excluding studies was insufficient study outcomes for example, lack of barriers and/or facilitators identified. Only four studies defined early mobilisation.12,28 –30 None of the studies meeting the inclusion criteria reported type of activities involved in early mobilisation interventions. See Tables 3 and 4 for study characteristics.
Study characteristics.
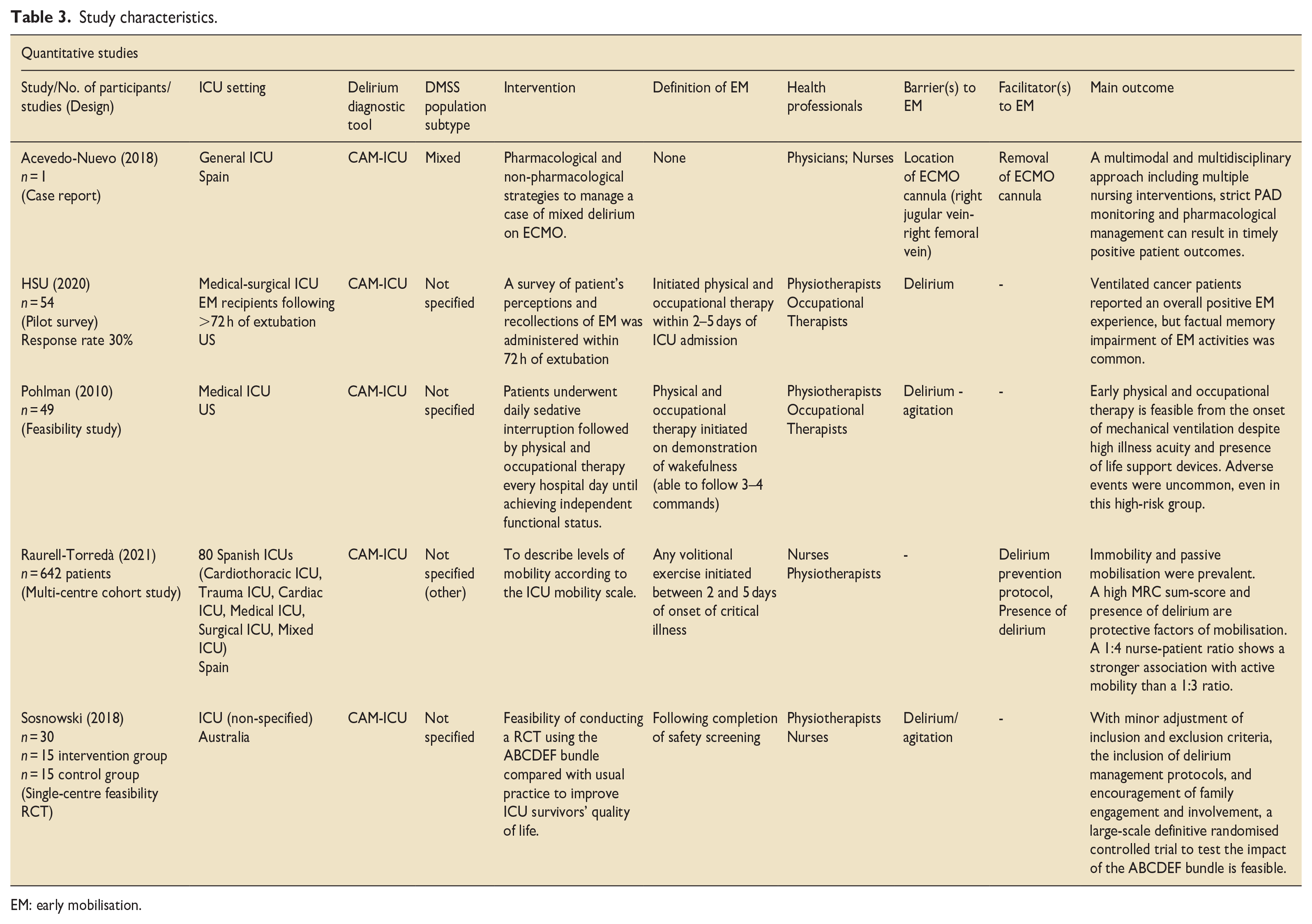
EM: early mobilisation.
Study characteristics.
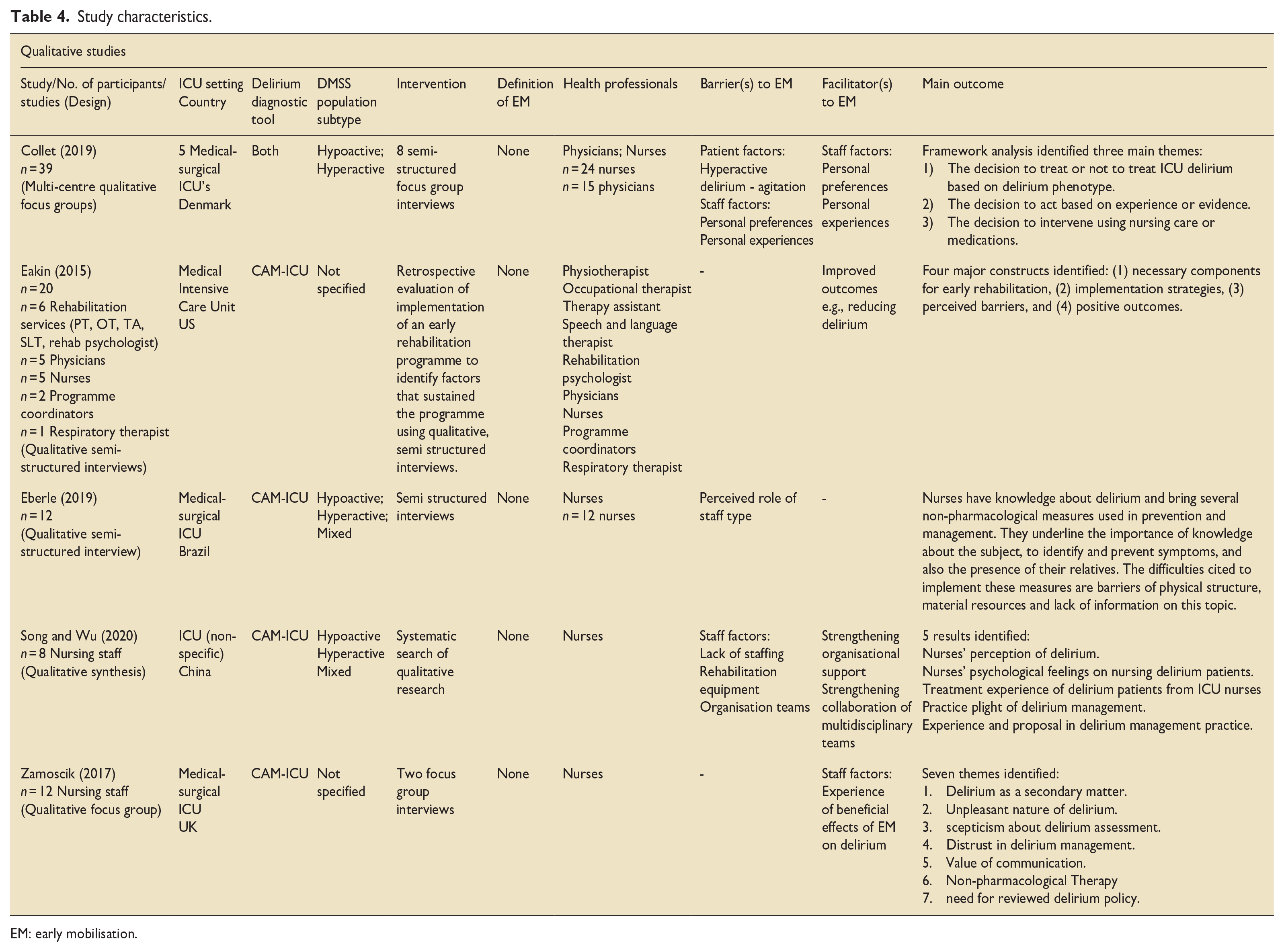
EM: early mobilisation.
Quality assessment
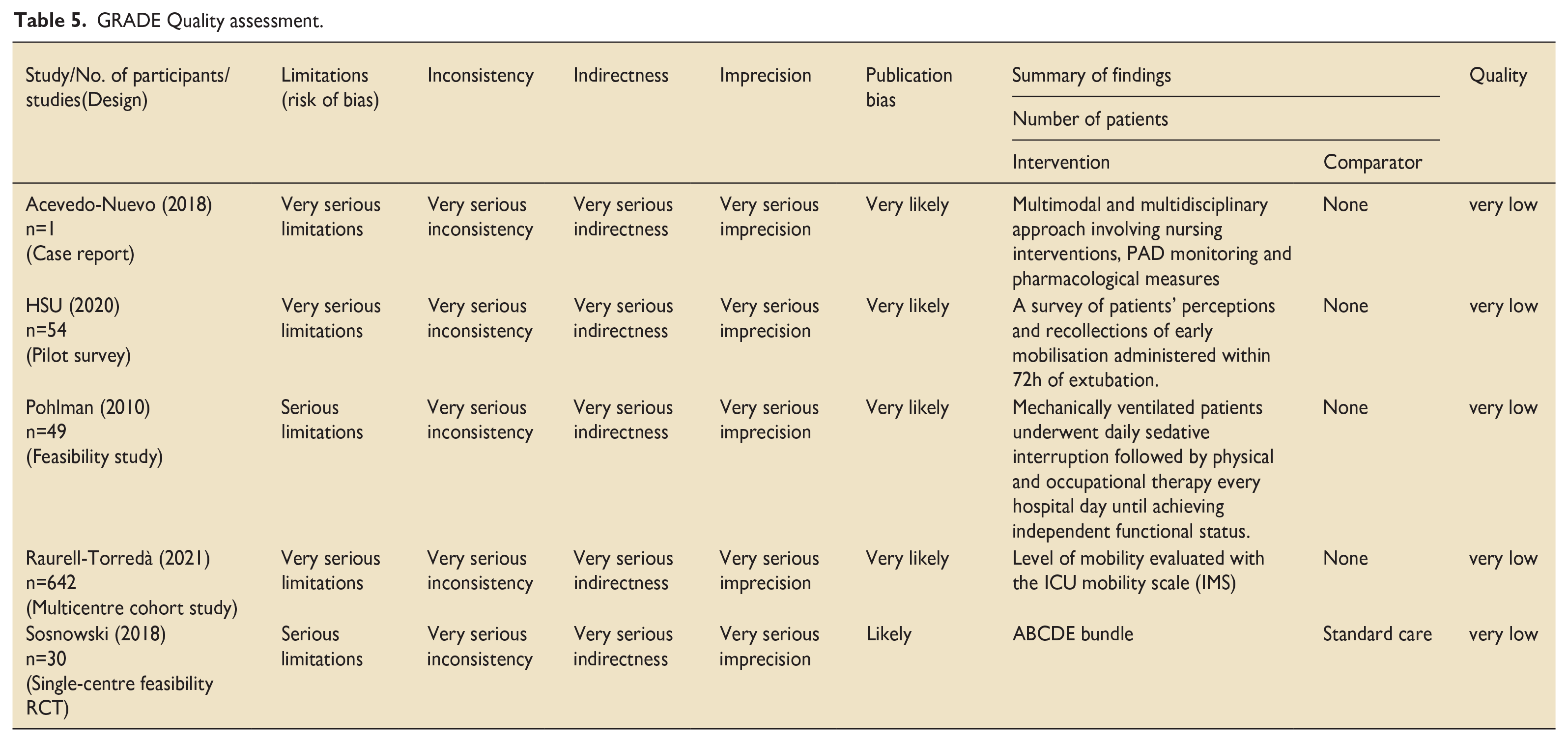
The five included quantitative studies consisted of non-randomised descriptive quantitative or observational studies. Therefore, these studies were graded as low (−1 or −2) at their start point of the GRADE quality assessment due to their study design. See Table 5 for the GRADE quality assessment.
GRADE Quality assessment.
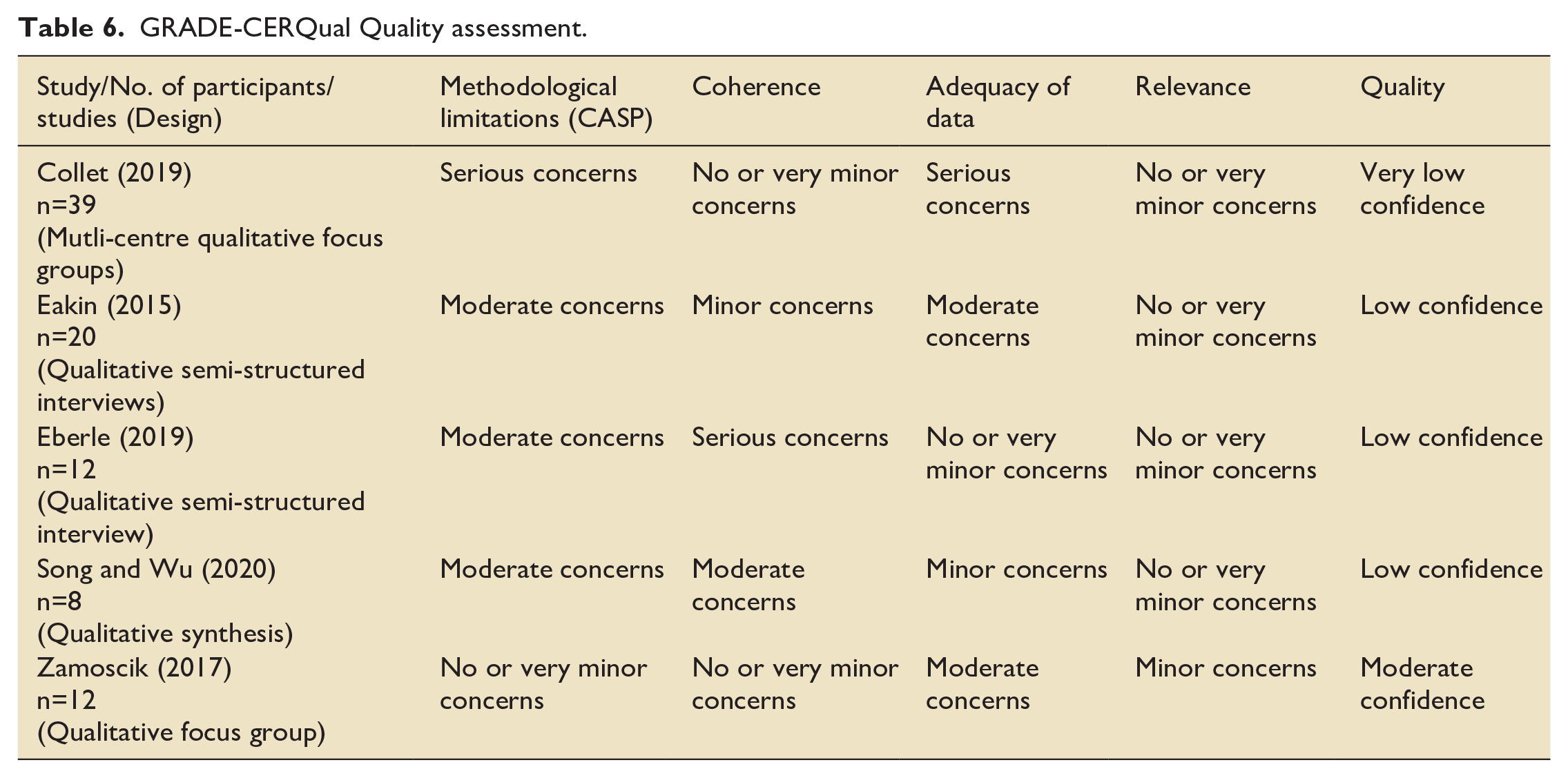
The GRADE-CERQual quality assessment (Table 6) was carried out for the five qualitative studies. These comprised of phenomenological qualitative designs. Studies were graded as high confidence (0), moderate confidence (1), low confidence (3) and very low confidence (1). The sample sizes for example, small focus groups and variation of reporting data saturation limited the quality of the included studies.
GRADE-CERQual Quality assessment.
Research question 1
The identified barriers to, and facilitators of, early mobilisation for patients with ICU-delirium are presented in Figures 3 and 4. Barriers to early mobilisation were more commonly reported (seven studies)12,20,27,28,30,31,33 compared to facilitators (five studies).27,29,31 –33 Two studies reported both facilitators and barriers to early mobilisation.27,31 There were no studies that reported the views of ICU patients and/or relatives.
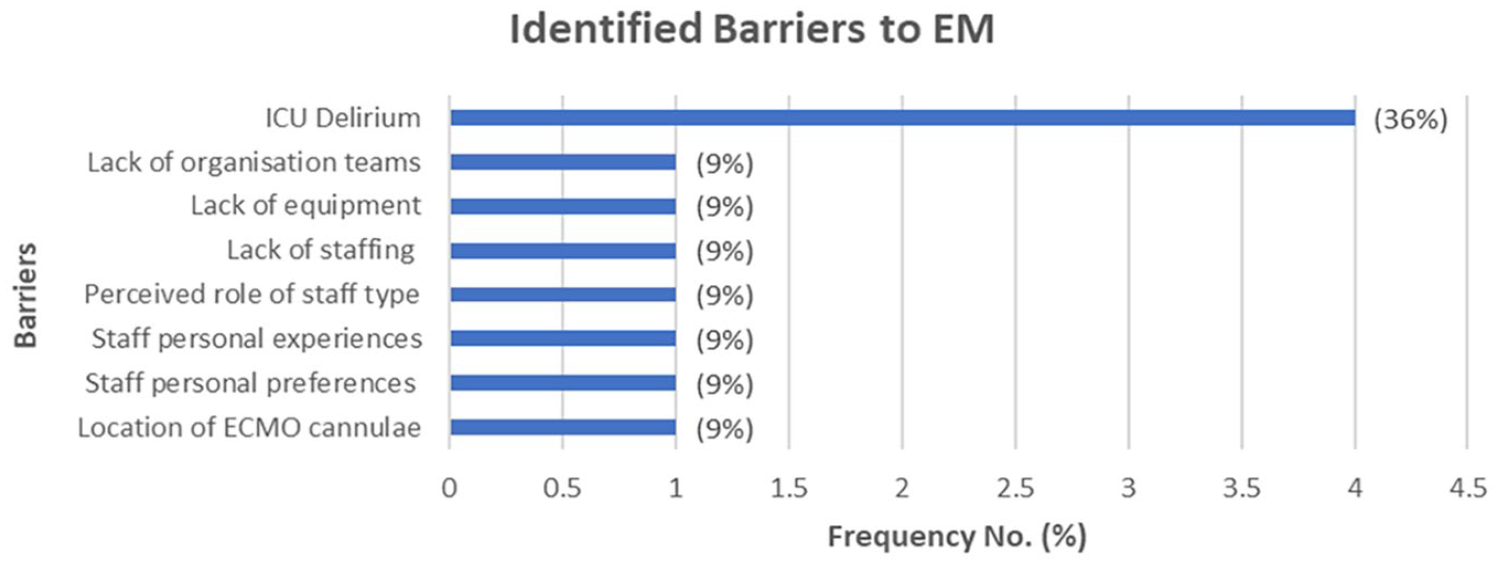
Reported barriers.
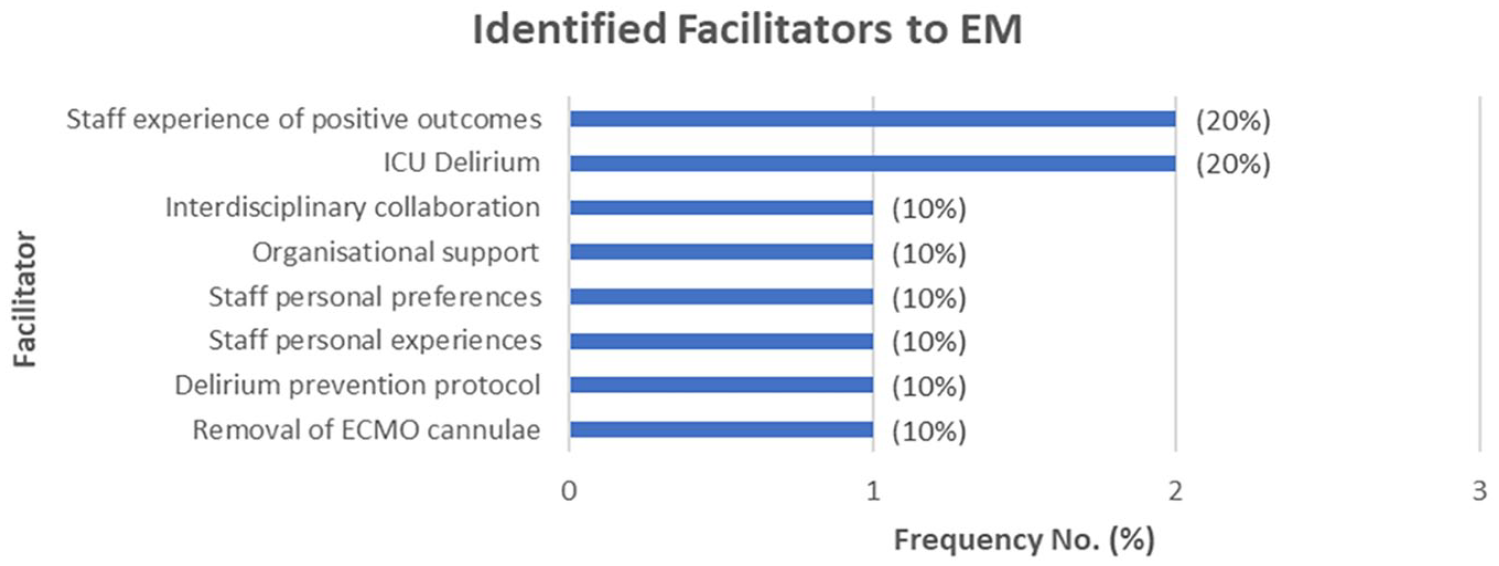
Reported facilitators.
The most common reported barrier to implementing early mobilisation for patients with ICU-delirium was the presence of delirium itself.28,30,31 However, one study reported hyperactive delirium and the presence of delirium were facilitators for carrying out early mobilisation interventions. 29 Other common barriers reported were lack of staff, lack of equipment and lack of team organisation. 20
The most common facilitator identified was ICU staff experience of positive outcomes resulting from early mobilisation such as reducing delirium.31,32,34 Interestingly, a survey found ICU staffs’ anxiety about the potential risks of early mobilisation such as patient safety was reduced following experience of the positive outcomes of early mobilisation for patients diagnosed with delirium. 27
Research question 2
Completion of stages 1 and 2 of thematic analysis identified 22 descriptive main themes. The final stage of analysis resulted in a total of six main themes and 12 sub-themes (Table 7). Quotations alongside each theme were included to illustrate study findings and support dependability of the data.
Main themes and sub-themes of thematic analysis.
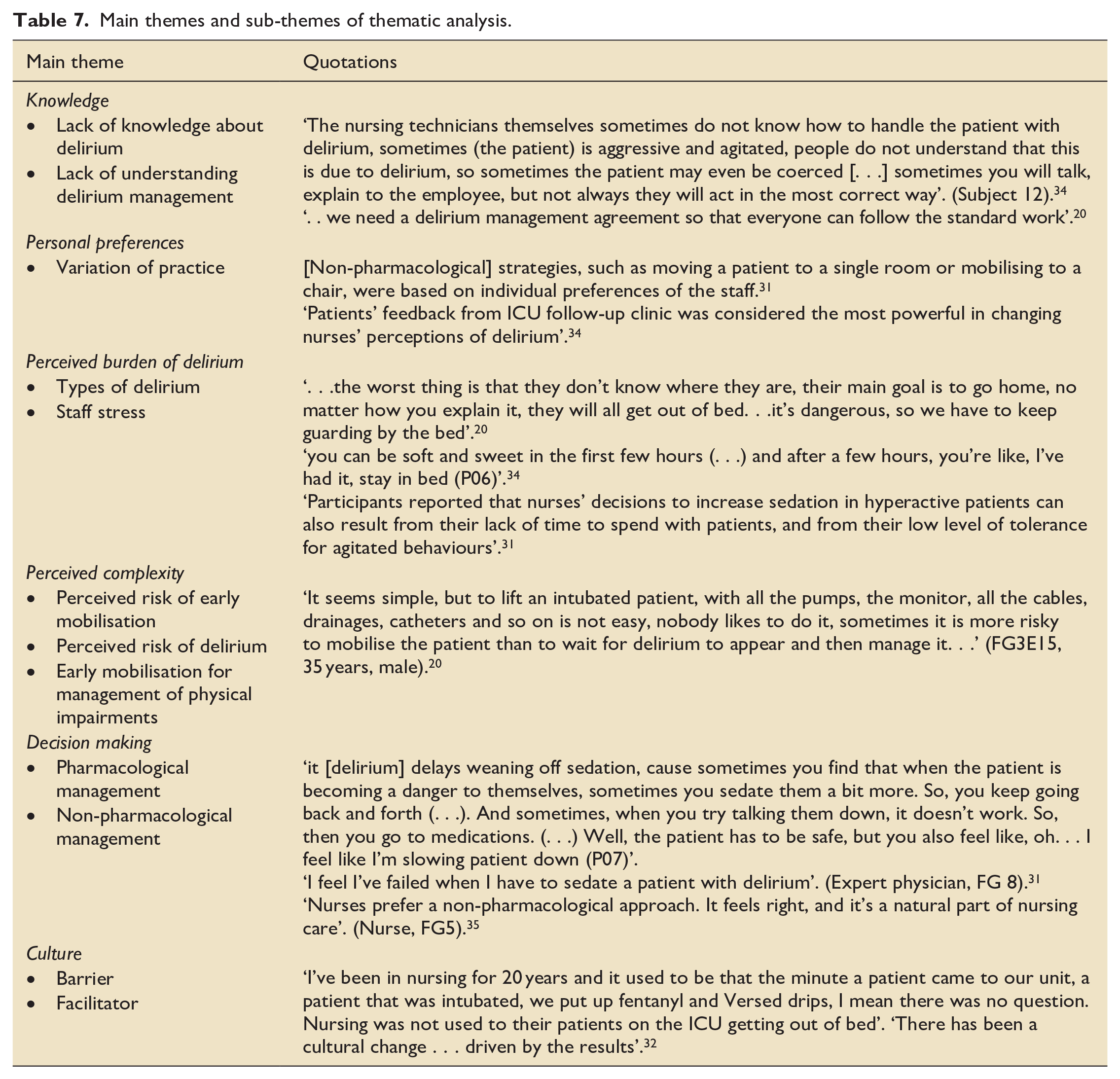
Knowledge
ICU staff knowledge related to delirium and early mobilisation was a prominent theme that appeared to influence the remaining five themes. ICU staff felt early mobilisation interventions were not fully understood due to lack of, or weak, evidence concerning timing, dosage, outcomes and standardised processes.20,33 Consequently, staff felt unconfident and lacked ownership of implementing early mobilisation interventions. 31 Staff relied upon personal preferences and individual experiential knowledge due to weak, or lack of, evidence within protocols. 31 Therefore, the lack of clinicians’ knowledge concerning delirium and how to respond to delirium on presentation resulted in patients often being misunderstood and under prioritised for early mobilisation interventions.33,34
ICU staff highlighted additional types of knowledge were needed such as shared experiential knowledge and interdisciplinary education to help them further understand delirium and early mobilisation.20,32,34 For example, shared patient’s stories.
Hyperactive and mixed delirium were perceived as barriers to early mobilisation. 31 This may be explained by their reports of not fully understanding delirium and early mobilisation as well as a need for further prescriptive information. 33
Personal preferences
The individual ICU staff member’s preference of delirium management influenced the application of non-pharmacological interventions such as early mobilisation.31,33 This was due to variation of sedation practice and staff reliability upon sedation to maintain the safety of delirious patients as well as lack of confidence to manage delirium on presentation.33,34 Furthermore, some staff showed an unawareness of the available best practice guidance regarding the management of delirium in the ICU. 34
Continuing education, collaborative team working and standardised documentation for each patient were methods discussed to potentially impact upon staff preferences and facilitate their understanding of early mobilisation and the patient’s recovery.20,34 Furthermore, patients’ stories were found to effectively change staff perceptions of delirium. 34
Perceived burden of delirium
Delirium itself was identified as burdensome for ICU staff.31,34 Staff associated delirium with frustration and an increased workload.20,31,34 Consequently, immobility and increased sedation were considered more convenient methods of delirium management.
Interestingly, patients experiencing hyperactive or mixed delirium were perceived as a greater burden than the hypoactive subtype which was perceived as the ‘ideal ICU patient’.20,31
Perceived complexity
Immobility was perceived as safer even if it led to the development of delirium due to the risk and complexity staff associated with early mobilisation.20,31 Therefore, staff were more likely to implement early mobilisation interventions for patients without delirium. 31 For example, ICU staff reported experiencing fear and anxiety of causing harm or further suffering to the delirious patient. 33 Moreover, staff often felt their efforts were not enough. 34 This may be explained by the reported lack of confidence in the available knowledge concerning application of early mobilisation versus experiential knowledge.20,34
Decision making
ICU staff reported conflict in their decision-making regarding sedation practice and non-pharmacological interventions such as early mobilisation.33,34 Poor staff satisfaction and low confidence were associated with increased sedation practices.31,34 Furthermore, fragmented decision making seemed to be influenced by the subtype of delirium (hyperactive) and individual staff preferences.31,33 Staff experience of the positive outcomes of early mobilisation for patients experiencing delirium including hyperactive patients was a motivating factor for ongoing implementation of early mobilisation. 34 ICU staff described positive outcomes such as improved sleep, reduced agitation and therefore improved staff workload. Consequently, ICU staff described improved confidence and staff satisfaction.20,31
Culture
The ICU culture was described to impact upon sedation and mobility practices for example, ‘active’ or ‘cautious’ ICU.32,34 Experience of the positive outcomes for patients and relatives as well as staff satisfaction contributed towards the development of an active ICU culture.20,32
Discussion
The findings of this systematic review are that delirium itself is a common barrier to staff implementing early mobilisation interventions in the ICU. The most common facilitator identified was staff experiences of positive outcomes as a consequence of early mobilisation. Thematic analysis highlighted the prominent theme of knowledge. Lack of knowledge and ICU staff understanding about delirium provided insight into the meaning behind the main reported barrier, delirium.
A previous systematic review of 49 included quantitative and qualitative studies investigated the barriers to implementing the multi-component ABCDE Bundle to minimise poor outcomes of mechanically ventilated patients. 16 One hundred seven barriers were identified from 49 included studies. Thematic content analysis using the Consolidated Framework for Implementation Research (CFIR) described four main barriers; patient-related (e.g. patient confusion/agitation); staff-related (e.g. lack of knowledge and confidence, preference for autonomy); protocol-related (e.g. unclear protocol criteria and agreement/discomfort with guidelines) and ICU contextual barriers (e.g. culture). These findings offer similarities to the identified themes of this systematic review such as the ICU culture. However, ICU staff knowledge was linked to knowledge and awareness of the ABCDE protocol. The number of barriers highlighted by Costa et al. 16 may suggest the complexity of the Bundle. The identified barriers were not explored according to each ABCDE component. This may have limited findings with consideration of the complexity of the Bundle. Therefore, the results of this systematic review may differ due to the focus upon a single component (early mobilisation) of the Bundle of interventions.
Trogrlić et al. explored implementation strategies for the assessment, prevention and management of ICU-delirium. 17 The systematic review included 21 quantitative studies comparing the effectiveness of implementation strategies upon clinical outcomes using meta-analysis. The results suggested multi-component implementation programmes including a higher number of strategies integrated with the pain, agitation, delirium guidelines (PAD) or ABCDE Bundle may improve clinical outcomes. However, these findings were limited by poor reporting and heterogeneity of delirium outcomes across the included studies.
A recent secondary analysis of an international point prevalence survey study including 135 ICUs across 33 countries found 90% of mechanically ventilated patients did not receive mobilisation or rehabilitation. 14 Interestingly, this finding was not associated with service pressures during the COVID-19 pandemic. For example, immobilisation did not differ between patients without or with a diagnosis of COVID-19 (7% vs 9%, p = 0.564). The survey results highlighted ICU clinician reported barriers to mobilisation and rehabilitation practice were: prone positioning, neuromuscular blockades, sedation, delirium, presence of devices, infection control measures and deranged circulation factors. Clinician reported facilitators were the presence of a specific mobility protocol and targeted/goal for mobility. The authors suggested the practice of mobilisation in ICU was particularly influenced by the ICU culture towards mobilising mechanically ventilated patients. These clinician reported barriers are similar to the findings of this systematic review such as, ICU culture, delirium and devices.
A systematic review and meta-analysis investigated the effectiveness of early mobilisation as an individual intervention or part of a bundle of interventions, upon the prevention and reduction of ICU-delirium. 36 Analysis of the 13 included studies showed a high level of uncertainty due to the wide variation across ICU populations and early mobilisation interventions. Moreover, the included studies demonstrated a low to moderate risk of bias. The authors recommended future research is needed in order to identify the effectiveness of early mobilisation on the prevention and treatment of ICU-delirium. These findings are comparable with the results of our systematic review. The lack of evidence may explain the staff reported barriers such as lack of knowledge about the impact of early mobilisation for this vulnerable patient population. Further evidence is needed in order to determine the most effective implementation strategies for the prevention and management of ICU-delirium and therefore support staff carrying out this complex intervention. Moreover, inclusion of qualitative evaluation of trials investigating complex interventions such as early mobilisation in the ICU may help to identify instrumental implementation programmes and strategies addressing both barriers and facilitators. 37
The majority of the included studies comprised of ICU staff’s perspectives of early mobilisation and delirium in the ICU. Understanding the patients’ and their relatives’ perspectives may support ICU staff to understand the role and value of early mobilisation for patients with ICU-delirium. Therefore, this may limit the findings of this systematic review. However, thematic analysis was reviewed by a public advisory group and a public member on our research team. All public members reported they were able to relate their experiences in ICU to the themes outlined in this systematic review. A systematic integrative review of definitions and activities for early mobilisation of mechanically ventilated patients identified that a standardised definition is currently absent. 10 The characteristics of the included studies for this systematic review (Tables 3 and 4), highlighted the variability of studies reporting a definition of early mobilisation. This may have impacted upon the inclusion of relevant studies and the interpretation of study findings.
The inclusion of delirium within the search strategy may have potentially influenced the findings of this study because other barriers may have been missed. However, the search strategy ensured that the results were not limited to the individual study key words. Moreover, the use of the PICO method identified findings that were specific to an ICU-delirium population according to the aims of this study. The barriers and facilitators highlighted in this review were indirectly reported in all studies because the evidence to date did not include delirium as a primary outcome measure for studies investigating early mobilisation interventions. Consequently, the quality of the included studies were low. Moreover, some barriers and/or facilitators may have been discounted due to lack of association with ICU-delirium patients. This may have impacted the inclusion of high-quality studies.
There is a need for future high-quality trials investigating delirium as a primary outcome measure for early mobilisation interventions.
Conclusion
This systematic review provides insight into the ICU staffs’ reported need to further understand the impact and value of early mobilisation upon delirium in the ICU. Future studies evaluating early mobilisation interventions involving the key stakeholders may highlight effective implementation strategies and support staff carrying out this complex intervention. This may aid translation of evidence into practice in order to improve and sustain implementation of early mobilisation interventions.
Amendments to the protocol
As a consequence of the COVID-19 pandemic, one member of the research team had to withdraw their involvement as the second reviewer. Mr. Christopher Manning kindly accepted the position in order for the work to continue.
Patient and Public Involvement
Patient and Public involvement (PPI) was guided by the National Institute for Health Research UK Standards for Public Involvement in research. 35 This systematic review was co-produced with a public member and previous ICU patient diagnosed with delirium on our research team (RG). Our public advisory group comprised of three (male) previous ICU patients diagnosed with delirium and one (female) relative. The members of the advisory group reviewed the thematic analysis and provided feedback via email. This ensured the relevance, rigour and effectiveness of the systematic review.
Supplemental Material
sj-doc-1-inc-10.1177_17511437231216610 – Supplemental material for The barriers to and facilitators of implementing early mobilisation for patients with delirium on intensive care units: A systematic review
Supplemental material, sj-doc-1-inc-10.1177_17511437231216610 for The barriers to and facilitators of implementing early mobilisation for patients with delirium on intensive care units: A systematic review by Jacqueline Bennion, Christopher Manning, Stephanie K Mansell, Roger Garrett and Daniel Martin in Journal of the Intensive Care Society
Footnotes
Acknowledgements
We would like to thank Professor Richard Atkinson, Population Health Research Institute, St. George’s, University of London, for his support to ensure methodological rigor; Ms Anna El-Jouzi, Liaison Librarian, Faculty of Health and Social Care, St. George’s University of London for providing the peer-review for the search strategy; St. George’s University of London library services and the Royal Free London library services for providing support to identify unpublished studies and full texts of included studies; the public advisory group and public member on our research team (RG) who gave support to ensure the relevance and rigor of this systematic review; Mr Robert Sun (a non-medical unfunded volunteer) supported the translation of texts published in Mandarin. Mr Sun is not responsible for any inaccuracies or misinterpretation.
Authors and contributors
JB: conceptualisation, methodology, software, investigation, formal analysis, data curation, writing – original draft, visualisation; CM: formal analysis, validation; SKM: resolved disagreements, writing – review and editing, supervision; RG: validation, writing – review and editing; DM: writing – review and editing, supervision, project administration.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This systematic review is independent research supported by the National Institute for Health Research HEE/NIHR ICA Programme Pre-doctoral Clinical Academic Fellowship, Miss Jacqueline Bennion, NIHR301174. The views expressed in this publication are those of the authors and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health and Social Care.
Ethics approval
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.