
Abstract
Little is known about the effect of alternative patient routes prior to ICU admission on clinical outcomes. Therefore, this study compared patients that were admitted directly from the emergency department into the ICU with those admitted from the wards. Patients admitted from the wards had significantly higher SOFA (6 vs 5, p = 0.038) and APACHE scores (19 vs 16, p = 0.007), as well as a greater need for invasive ventilation (45.5% vs 28.6%, p < 0.001). Hence, this hypothesis-generating study suggests that further work is needed to assess if scoring systems are sensitive enough to assess the need for ICU admission.
Introduction
Patients are admitted to intensive care units (ICU) from different locations within the hospital including the emergency department (ED), inpatient wards and operating theatres. 1 Delays in admission to ICU have previously been associated with poorer patient outcomes including inpatient mortality. 2 Prompt and appropriate ICU admission has the potential to improve endpoints, however delays in recognition of potential ICU patients is observed across healthcare settings. 3
Irrespective of the timeline, patient’s location within the hospital has also been suggested to affect clinical outcomes. 4 Individuals admitted to the ICU from wards have been associated with increased mortality compared to those admitted directly from ED. 4 Due to limited recent literature across the UK on how different pathways into the ICU affect prognosis, this study aimed to investigate if ward-based patients had poorer clinical outcomes and whether they could have been identified earlier.
Methods
This retrospective cohort study was conducted within the ICU at Royal Preston Hospital, Lancashire Teaching Hospitals Trust. Patients that were admitted between July 2022 and December 2023 were divided into two groups – direct from ED to ICU or indirectly from ED to ward to ICU. To control the level of acuity across the cohorts and reduce the impact of hospitalisation, individuals that were either post-operative or admitted into ICU after 48 h of hospital admission were excluded from the study.
Data including patient demographics, background, admission details, clinical scoring systems (National Early Warning Score, Sequential Organ Failure Assessment and Acute Physiology and Chronic Health Evaluation II scores) and patient outcomes (organ support, length of ICU stay and inpatient mortality) were extracted from the MEDICUS database and anonymised into a Microsoft Excel spreadsheet. The data underwent relevant statistical analysis using the Statistical Package for Social Sciences (SPSS (IBM, USA)). Secondary analysis was conducted by reviewing electronic records of ward-based patients to assess if delayed recognition of their clinical deterioration, defined as referral to the ICU team after 4 h of NEWS 7 or more, contributed to their fatal outcome. Conducted as a service evaluation quality improvement project, ethical consideration was taken in accordance with local trust policy and maintained throughout.
Results
A total of 514 patients were recruited onto the study, with 429 individuals being directly admitted from ED and 85 individuals from the wards. Both cohorts had similar demographics and comorbidities, except for a higher prevalence of chronic renal disease amongst patients admitted from the wards (22.4% vs 11.9%, p = 0.034).
On initial arrival to the hospital, patients admitted directly from ED had a higher mean NEWS compared to those transferred to the wards (NEWS 6 vs 4, p < 0.001). There was no longer this difference at the time of ICU admission between the two groups (p = 0.444). Conversely, patients admitted from the wards had higher mean SOFA (6 vs 5, p = 0.038) and APACHE scores (19 vs 16, p = 0.007) than those admitted directly from ED on admission to the ICU (Table 1).
A table comparing the scoring systems of patients admitted to ICU directly from ED versus the ward.
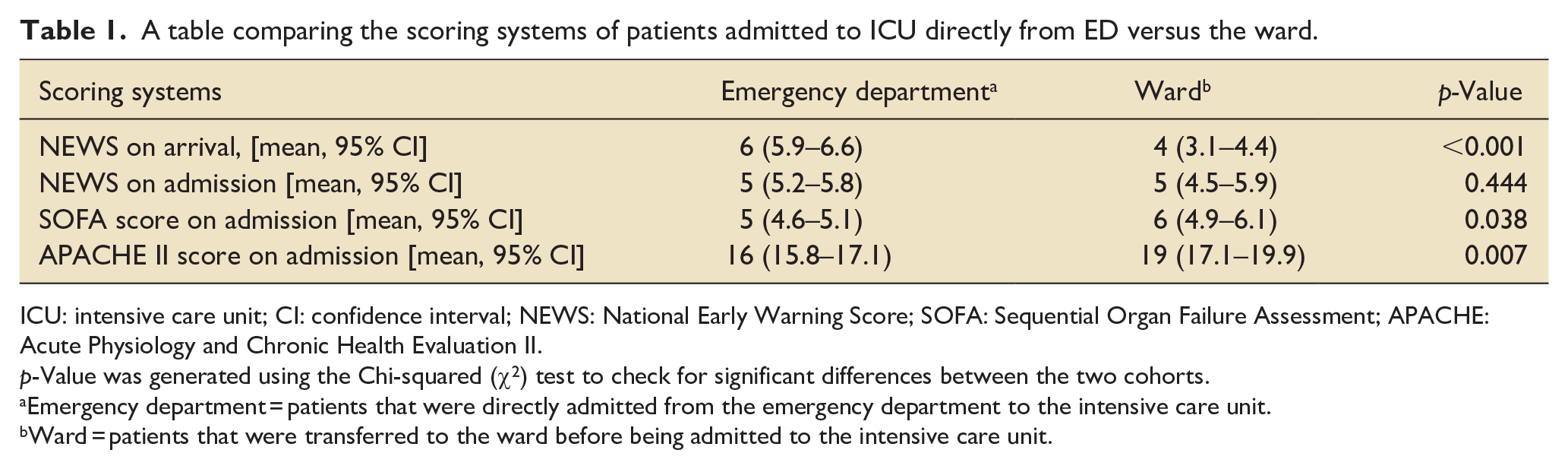
ICU: intensive care unit; CI: confidence interval; NEWS: National Early Warning Score; SOFA: Sequential Organ Failure Assessment; APACHE: Acute Physiology and Chronic Health Evaluation II.
p-Value was generated using the Chi-squared (χ2) test to check for significant differences between the two cohorts.
Emergency department = patients that were directly admitted from the emergency department to the intensive care unit.
Ward = patients that were transferred to the ward before being admitted to the intensive care unit.
Respiratory support was the commonest form of organ support across both groups, followed by cardiovascular and renal support subsequently (Table 2). Greater use of invasive ventilation amongst the ward patients (45.5% v 28.6%, p < 0.001) was the only difference in clinical endpoint observed between the two groups.
A table demonstrating the rates of organ support by system, mortality and ICU length of stay of patients admitted to ICU directly from ED versus the ward.
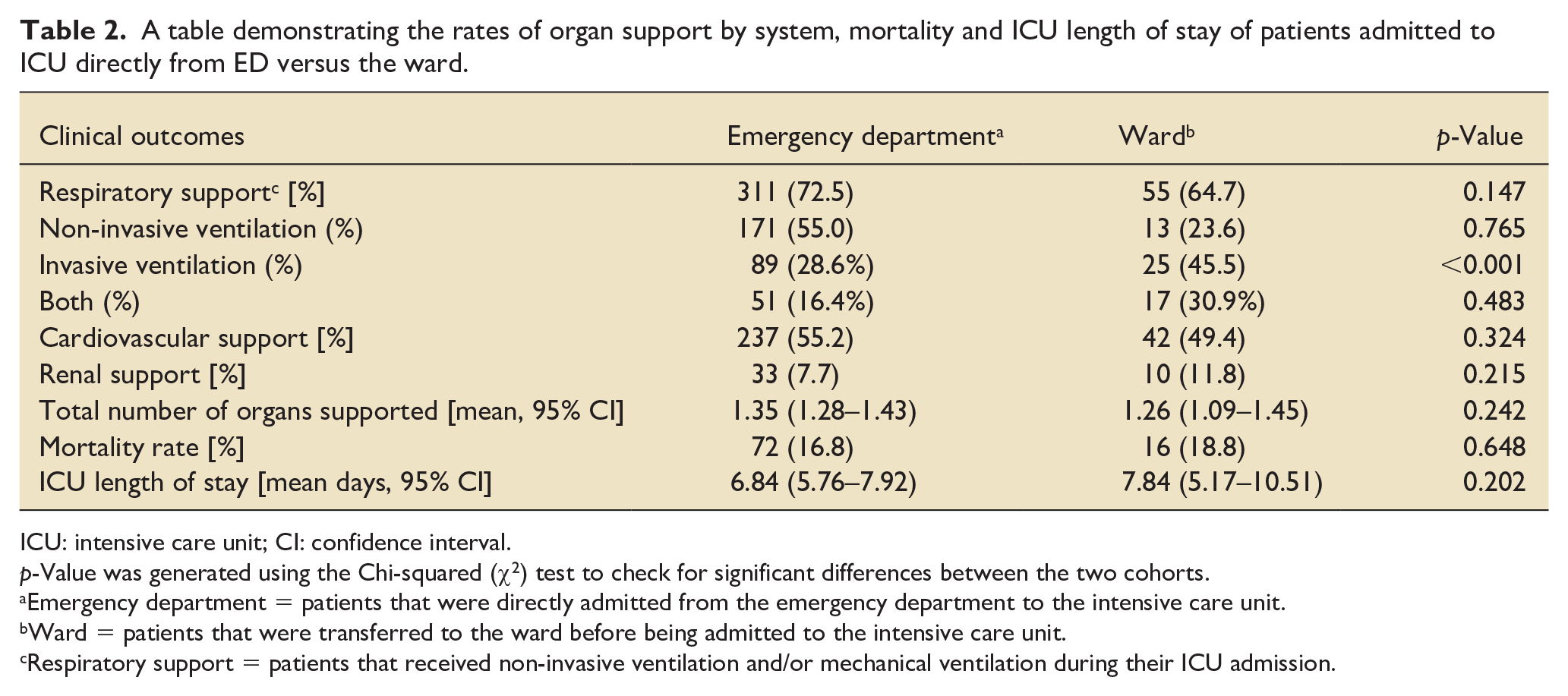
ICU: intensive care unit; CI: confidence interval.
p-Value was generated using the Chi-squared (χ2) test to check for significant differences between the two cohorts.
Emergency department = patients that were directly admitted from the emergency department to the intensive care unit.
Ward = patients that were transferred to the ward before being admitted to the intensive care unit.
Respiratory support = patients that received non-invasive ventilation and/or mechanical ventilation during their ICU admission.
Secondary analysis of the 16 fatalities within the unit that were admitted from the wards showed 7 (44%) individuals had delayed ICU admission, with 5 of them (71%) being treated for sepsis of various sources.
Discussion
The study suggested that although the NEWS is a good prognostic marker, 5 the SOFA and APACHE scores could be better discriminators of the need for ICU admission earlier in the patient journey, as observed in previous literature.6,7 Considering the limitations of basing clinical judgements on scoring systems, they could be used alongside other patient factors when assessing the need for ICU admission.
The study showed conflicting findings to previous evidence,8,9 as it highlighted greater proportion of patients admitted from the ward required invasive ventilation whilst no difference in mortality rate and ICU length of stay was observed between the two groups. Being a single-centre study and hypothesis generating, the study suggested further research is needed to explore the relationship between alternative patient pathways leading to delayed admission and ICU outcomes.
Secondary analysis of the ward group showed delayed recognition was common across all of the fatalities, however similar findings have been observed amongst ED patients. 2 Therefore, in an overstretched health system with limited supervision of each patient, delayed recognition could have a greater impact on poorer clinical outcomes than the patient’s journey to the ICU. Hence, the focus should also turn to developing integrated electronic patient records and enhanced outreach services to promptly recognise patients developing critical illness.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.