
Abstract
Introduction:
Non-medical consultant level roles have been in existence for over 30 years, however the number of allied health professionals (AHPs) working at this level, particularly in critical care, remains relatively small. National guidance highlights the importance of clinicians in these roles to work across the four pillars of practice. However, little research exists regarding the roles undertaken by these consultant-level practitioners, the contributions made to service delivery and their perceived impact on patient and service outcomes. Based on this, the aim of this project was to explore the perceived impact of consultant-level AHPs working within critical care.
Methods:
Qualitative methodology was used involving a combination of interviews and focus groups. Purposeful sampling was used to recruit AHPs in consultant-level positions within critical care. Senior medical and nursing staff were then recruited via the AHPs. Data were analysed thematically using the Braun and Clarke methodology.
Results:
Five consultant-level AHPs were recruited to participate in interviews, with a further 7 participants from senior medical and nursing roles participating in one of two focus groups. The AHPs had been in a consultant-level role for an average of 3.2 years, with all participants reporting over 15 years’ experience within critical care. Four core themes were generated from 105 unique codes and 13 subthemes. Personal characteristics were apparent across all themes and therefore was included as a central element. The core themes were (1) scope; (2) status; (3) supportive leadership and (4) impact.
Discussion:
Through four core themes, this study has highlighted the roles undertaken by consultant-level AHPs working in critical care, their perceived impact on patient and service outcomes, and their contribution to local, regional and national workstreams. Where these roles exist, they appear to be well received by senior medical and nursing staff, reporting the benefits of highly experienced members of clinical staff to improve service delivery, patient outcomes and contribute to strategic planning.
Introduction
Consultant-level (non-medical) clinical practitioner posts were developed in the 1980s in healthcare science and taken up in nursing in late 1990s. This followed a widespread consultation exercise which recognised that the existing nursing career structure was leading to experienced staff leaving direct care roles for careers in management or teaching.1,2 Since then, consultant-level practitioner roles have developed across a range of professions, for example, allied health professionals (AHPs) and pharmacists. 3 However, the number of roles existing within critical care, particularly those roles fulfilled by AHPs, remain extremely low with only six consultant-level AHPs posts identified in a 2021 UK-wide workforce survey.4,5 The reasons for this are likely multifactorial and have not yet been explored.
Consultant-level clinical practitioners are defined as experts in clinical practice, demonstrating innovation, and influential clinical leadership within a specific field, with a clear focus on the benefits for service users. Those in consultant-level roles should exercise the highest degree of professional autonomy and decision making, working strategically across a range of models of service delivery to influence local, regional and national policy.6,7 The Royal College of Nursing highlight consultant-level practice describes a level which can only be delivered by registered staff who have progressed from an advanced level within their field to reach a significantly higher level. 8
Many professions have guidance for consultant-level roles, with NHS Wales and NHS England developing frameworks for expected standards for consultant-level practitioners.3,6 In alignment with all nursing and AHP roles, each guideline recognises that a consultant-level practitioner works across the 4-pillars of practice, namely clinical practice, leadership, research and education. However, those operating at consultant-level are expected to be experts in their clinical field, provide enabling strategic and enabling clinical leadership across traditional professional boundaries, and develop a knowledge rich and research culture. 6 Furthermore, a consultant-level practitioner must exercise the highest degree of professional autonomy and decision making, with the purpose of improving outcomes for service users by enhancing services and quality of care. 3
Despite the presence of national guidance and recommendations, little research exists regarding the roles undertaken by these consultant-level practitioners, the contributions made to service delivery and their perceived impact on patient and service outcomes. Therefore, the aim of this project was to explore the perceived impact of consultant-level AHPs working within critical care. Secondary aims included exploring the roles undertaken, the contributions made and areas for future development.
Methodology
Study design
This study had a qualitative descriptive design. Data were collected via interviews and focus groups, and analyses using inductive descriptive thematic analysis. 9
Participants
Purposeful sampling was used to recruit consultant-level AHPs working within critical care (including therapy-wide roles, dietitians, occupational therapists, physiotherapists and speech and language therapists). Consultant-level AHP participants were identified via direct contact by the research team (via existing professional networks), advertisement with specialist interest groups, and social media (X platform).
Senior nursing and medical staff were recruited via the AHPs participating in the study. This was completed via an invitation letter or direct contact via email.
Sample size
The planned sample size was 12–16 participants. Consisting of 5–7 consultant-level AHPs and 7–9 senior medical and nursing staff. This sample size was calculated based on an estimation of 8–10 consultant-level AHP posts existing in critical care, and at least one nurse and medical consultant from each organisation hosting an AHP consultant post. A limited inclusion criteria was used to recruit either the consultant-level AHPs or medical/nursing staff working with those AHPs. No limitations were set as to professional background of AHPs.
Methods
Interviews were conducted with consultant-level AHPs (n = 5) via MS Teams between June and July 2024. Two multi-professional focus groups were held (via MS Teams) with medical consultants and senior nursing staff working in a critical care that employed a consultant AHP, in September and October 2024.
To reduce bias of the lead researchers’ preconceptions of consultant-level AHP roles, all interviews and focus groups were conducted by LJ, a female physiotherapist with 7-years’ experience of working in critical care, but not at consultant-level. No other members of the research team were present during the interviews or focus groups. Pre-defined interview and focus group questions, consisted of open-ended questions on the impact of consultant-level AHP practice in critical care, the unique contributions made and the roles and responsibilities (see Supplementary Information). Each interview lasted between 22 and 30 min, and the two focus groups lasted 34 and 43 min.
All recordings were transcribed verbatim using the inbuilt MS Teams transcription tool, downloaded, and corrected for accuracy by the lead researcher by reviewing the video recordings. All transcripts were anonymised using code numbers prior to analysis. A pragmatic decision was made not to return transcripts to participants for comments and corrections.
Analysis
Descriptive thematic analysis was completed, using the method of Braun and Clarke. 9 The lead researcher (PT) analysed all transcripts, with second coding completed by other members of the research team (LJ, GC and ET). PT is a consultant-level therapist (physiotherapist by background), working within critical care.
The potential bias of PT conducting the analysis was the inherent bias of seeking to demonstrate impact of consultant-level AHPs. The researchers used a modified critically reflexive approach to self-consciously critique and evaluate how their biases may have affected the research process and outcome. 10 Whilst utilisation of second coders is not recommended by Braun and Clarke, 11 it ensured a multi-professional approach to the analysis which was appropriate for the participant sample. All disagreements were discussed and resolved by referring to the original statements. Where disagreement remained, consensus was taken across the research group. Themes were identified and agreed through discussion with all members of the research team. The involvement of researchers from varying professional backgrounds and roles including higher education institutes (UJ, GC), ensured a variety of perspectives and allowed open transparent discussions of potential themes including any unique professional traits.
Ethical considerations
The study was approved by the Health Research Authority (HRA) and Health and Care Research Wales (HCRW) on the 9th April 2024 (Ref: 24/HCRW/0007, IRAS 340616).
Results
Demographics
Twelve clinicians participated across five interviews and two focus groups. Consultant-level AHPs included two physiotherapists, two speech and language therapists and one dietitian. One physiotherapist was in a role titled ‘consultant AHP’, whereas all others held consultant-level titles specific to their profession, for example, consultant speech and language therapist. Average time in post was 3.2 years, all participants had >15 years post-graduate experience. Further demographics are shown in Table 1.
Demographics of AHP participants.
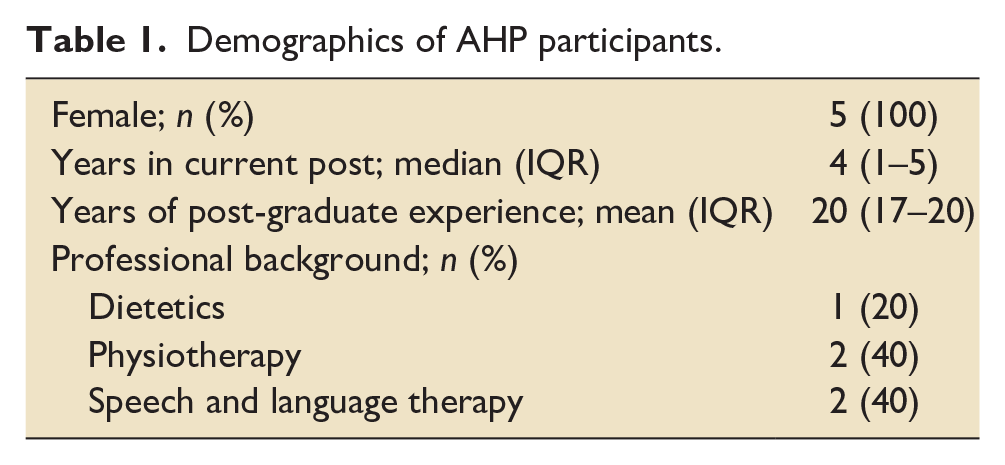
All consultant-level AHPs worked in organisations across NHS England and no organisation was represented more than once. The seven participants involved in the multi-professional focus groups were from four-different institutions and included three consultants in intensive care medicine and four senior nurses, all had over 15 years of experience in critical care.
Overarching themes
A total of 105 unique codes were created, categorised into 13 subthemes, see Supplementary Material. These potential sub-themes were then referenced back to the original codes and consensus was reached across all researchers for four core themes. Themes were: (1) scope; (2) supportive leadership; (3) impact and (4) status. The perceived personal characteristics of those in consultant-level roles were apparent across all themes and considered as a central element (see Figure 1).
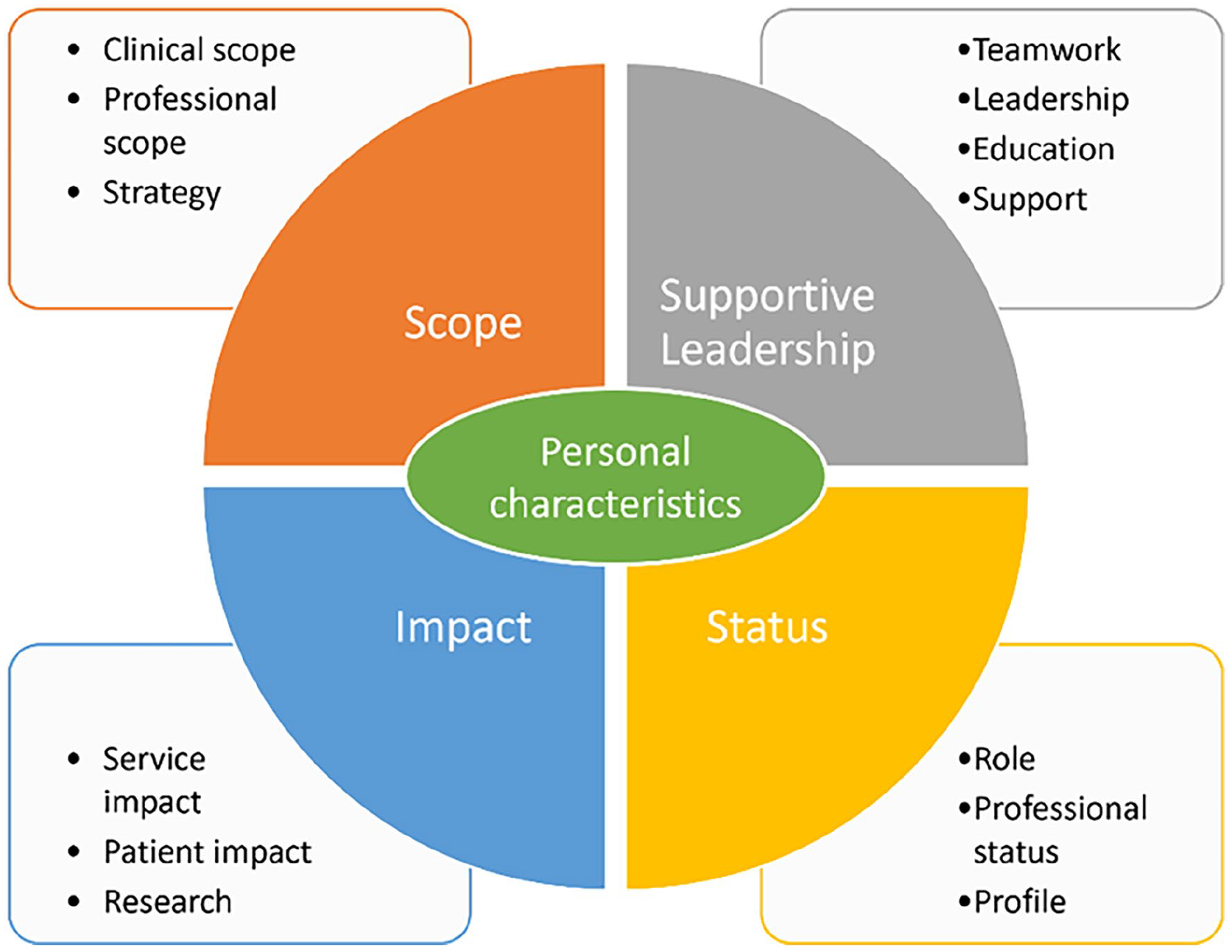
Combined themes from interviews and focus groups.
Scope
The theme ‘Scope’ encapsulated clinical scope, professional scope, and strategy, and were present in both interviews and focus groups.
Clinical scope referred to specific activities undertaken by those working at consultant level, as well as referring to expected ‘expert’ level of practice. This included undertaking of activities traditionally undertaken by medical staff (e.g. bronchoscopy, tracheostomy tube changes), other extended scope roles (e.g. ventilator weaning strategies, arterial blood gas sampling), and being responsible for oversight of aspects of clinical service delivery, for example, delivery of a fibreoptic endoscopic evaluation of swallowing (FEES) service for critical care or provision of critical care recovery clinics, including all associated aspects of quality, safety and experience.
I01: I also oversee but don’t run or don’t participate in the post ICU Recovery clinic
A number of specific activities (e.g. FEES) were also reported by the focus group participants, with comments suggesting that the completion of such tasks had impacted positively on patient care.
FG01: They have been offering FEES with ENT (ear, nose and throat) and doing that independently. . . of and that’s that has proved extremely useful, especially for our patient cohort
Professional scope was particularly highlighted by AHPs, including discussions on the nuanced nature of the consultant-level roles but the need for clear job planning.
I01: . . .it is a mix of, or it’s meant to be a mix of all of the four pillars of practice working at that consultant level
This was further reinforced in statements recognising the need for these roles to incorporate the four pillars of practice, but with flexibility for the contribution to each pillar to vary based on needs of the organisation and service.
I01: You know, I’m still doing A, B and C clinically, I can go and do research and stuff, and I’ve got this flexibility of that. . . the focus will be skewed on each of the pillars depending on which service that you work for
Challenges associated with the wide professional scope of the roles were also reported, including time pressures, prioritisation of activities and the self-imposed expectations of the role.
I05: So it is a challenging role in terms of juggling a lot of different work streams.
These challenges were not highlighted in the focus groups, with participants reporting a lack of understanding of the scope of the roles and no real clarity on how the roles are created or job planned.
FG02: I admit to not really understanding how one gets appointed to that grade for allied professionals.
Involvement of consultant-level AHPs within organisational strategy was reported by all participants, with senior nursing staff in particular reporting the value of AHPs contributing to strategic planning. This included involvement in patient pathway planning and service development, with AHPs providing a unique insight based on understanding of services outside of critical care and patient trajectory on discharge.
FG03: Because they will see things that other specialties involved in that planning or managers won’t see. So, I think that has taken us to a different level as well.
Supportive leadership
The theme ‘supportive leadership’ encapsulated teamwork, leadership, education and support. This encapsulated the support provided by the consultant level AHP, for example, supportive leadership for colleagues both locally and nationally for ongoing development; and the support provided to the consultant-level AHP, for example, organisational, management and senior clinical leader support.
All participants referred to leadership as a key aspect of the consultant-level AHP role. This included discussions around people development, influencing and empowering others. AHP participants often considered this to be within AHP teams or AHP services, whereas nursing and medical colleagues highlighted the influence on the wider multi-disciplinary team.
IO4: strong ability to lead the team where perhaps you’re the only person with that expert knowledge FG7: sort of extending outside of critical care and again helping move patients on, but actually helping services in the rest of the hospital
Challenges of leadership were also highlighted, with some AHPs reporting a need to act as a line manager for staff which placed additional demand on them and shifting the relationship in accountability. They also reported challenges around seeking peer support for themselves within the role, including the need to identify willing medical consultant colleagues to provide that support.
I01: Sadly, at the moment I also have a line management role. Which we are trying to disentangle from the consultant post because I think once you have a line management role, it does take away a lot from that kind of clinical role.
Aligned with leadership, the subtheme of support focused more on acceptance and support provided by the organisation and individual critical care area. It was highlighted that consistency of staffing over prolonged periods of time was important in raising the profile of the individual within an organisation and in the development of consultant-level roles.
I04: It takes time to breakdown those misconceptions of roles and allow yourself to be seen as a valued member of the team.
The importance of teamwork and multi-professional working was highlighted by all participants, as well as the need for collaboration. Collaboration was particularly referenced by the AHPs, with the need to link with local higher education institutions (HEIs), professional bodies, for example, chartered society of physiotherapy and relevant specialist interest groups.
However, it was also highlighted that multi-professional working with AHPs, and wider allied health professionals was not exclusive to those in consultant-level posts, and that this teamworking exists at all levels of practice and was present prior to the development of the consultant therapy post.
FG02: . . .we have always had, since we started doing MDTs (multi-disciplinary team) meetings, physios, OT, Speech and language present. And they are not necessarily consultants.
Discussions around the role of consultant-level AHPs in education was only identified by AHPs, who highlighted the importance of involvement in both local and national education. This included working with HEIs to deliver undergraduate and postgraduate education, and the provision of education through national training programmes, study days and informal teaching. Involvement in teaching was often linked to job planning and expectation of evidence of the 4-pillars of practice, opposed to a definitive aspect of the role or a priority for those in the roles.
I01: education is part of the process. . .working across the four pillars, so clinical, leadership, education, research
Impact
The theme ‘impact’ included service impact, patient impact and research. Research was included in this theme due to the number of unique codes discussing consultant-level AHPs’ increasing research activity, with evidence of leading studies and promoting other therapy staff to be involved in research, for example, via associate principal investigator programmes. There was recognition of the impact of consultant-level AHPs driving evidence informed practice, and where evidence did not exist, to use research to fill the gap. One participant also raised the potential financial benefits of involvement in research trials, with the opportunity for the consultant-level AHP role to bring income to the organisation and create future roles.
I02: . . .but that’s increasing research capability and then it’s income generation. . .So, it’s (the post) paying for itself if you like, and at the same time your staff are becoming more skilled through research
Patient and service impact was highlighted in both interviews and focus groups. This subtheme focused on improved patient experiences and outcomes. This was less attributed to the individual AHP in the consultant-level role, but the wider impact these roles may have on therapy service and indeed the overall critical care service. Medical and nurse participants also highlighted how the presence of consultant-level roles could benefit the recruitment and retention of AHPs at all levels of practice, with clearer career development pathways for staff to progress through agenda for change banding to a high level. It was suggested that teams with a AHP working at consultant level, also had improved numbers of therapy staff, compared to services with no consultant-level post. This was seen as creating inequity across trusts or health boards.
FG08: . . .as the role comes with a higher banding and actually that is something perhaps to help recruitment and retention. . .having another grade and pay grade that people can advance to, I think is extremely helpful
Overall, participants reported the positive impact of the consultant-level therapy role, but there was also recognition that caution was needed given the limited number of the posts across the UK and the lack of standardised job plans. Focus group participants highlighted that whilst their experiences were positive, there was potential, particularly if role numbers increase, for the impact to be dampened or become more uncertain. This was suggested as a possibility if the post holder were more focused on strategic elements opposed to maintaining a clinical focus.
FG02: . . . (The consultant-level AHP) definitely puts in an enormous amount of clinical work. But I can imagine there might be some people who would be less inclined to do that and be more inclined to sit making strategic decisions. . .that perhaps could have a negative impact on the service provision to patients.
All participants were unsure if having multiple consultant-level AHPs within a single service would be of benefit or could cause conflict or a lack of clear leadership.
FG01: Sometimes you have, like too many chiefs, so if everyone is a consultant level and then you got 100 consultants, and the team is just so huge. Who makes those decisions in the end?
Status
The ‘status’ theme and associated subthemes were much more prominent across AHPs rather than medical and nursing participants. Consultant-level AHPs regularly discussed the importance of such posts on a local, regional and national (and at times international) scale. Indeed, four of the five AHPs involved felt that this high-level profile was an essential requisite of the consultant-level of practice, and that it should be expected that consultants should influence at a national level. This included the development of national guidelines, input to major projects and being a spokesperson for their profession and wider AHPs.
I04: So, it’s trying to as a consultant trying to influence national practice, national policies and national procedures, as well as ensuring that we are ticking the right boxes locally.
However, this view was not reflected by one AHP, and nor was it apparent within the focus groups. Indeed, one AHP felt that this should not be the case and only resulted in increase pressure on that individual.
I03: we are very level obsessed. . .and the expectation that we create puts so many obstacles in the way of people that want to aspire to get into these roles, which is neither kind, nor is it, you know, the reality of a lot of other things.
AHPs and medics and nurses involved in the focus groups suggested that those in consultant-level roles are likely to be AHP experts and therefore represent the voice for all AHPs working within critical care. This was the case whether the consultant-level role was uni-professional (e.g. dietitian) or multi-professional (e.g. consultant therapist).
In contrast, there was significant variance between the AHPs and medical and nursing participants for the ‘role’ sub-theme. As expected, AHPs had a clearer understanding of the purpose of the role and how they were developed. However, nursing, and medical participants, admitted a lack of understanding of the of the roles. This included lack of clarity over remit, and how roles are created, particularly whether roles are created for specific individuals as opposed to service or organisational need. Indeed, one participant suggested that education is needed for the wider multi-professional team around these roles, which in turn may aid future development and opportunity.
FG02: . . .perhaps there needs to be a bit of education on the role really. Perhaps coming from not those people, but you know the colleges or regulators.
Furthermore, the use of the ‘consultant’ title was highlighted by both participant groups. This included concerns regarding misrepresentation of the use of ‘consultant’, and potential confusion for patients regarding job role and professional background.
FG07: I think the idea of having consultant nurses and consultant therapists (AHPs) is an excellent one. But I wonder. . .going back to what we’ve said already on this topic, when the public hears consultant, they probably think consultant doctor, incorrectly, of course
Personal characteristics
The personal characteristics required for people undertaking consultant-level AHP roles were reported by the AHPs themselves with less recognition from the wider multi-professional team in the focus groups.
Consultant-level AHPs highlighted the need for those undertaking these roles to display certain characteristics, some of which are included within job descriptions and specifications. These include level of experience of the individual and their existing knowledge base. However, other characteristics focused more on values and behaviours, including the need to demonstrate vulnerability in the role and have high levels of personal accountability.
I04: You’ve got to be vulnerable. We have got to answer questions, defend our practice.
The personal challenges of the role were also highlighted with pressure to deliver and need for sacrifice in terms of availability outside of working hours to provide support clinical and non-clinical activity.
I05: . . .it is like, well actually that was on the day when I do not work. Do I get that time back or do I just suck it up? And you know, sometimes it is just suck it up.
The importance of AHPs in consultant-level roles to be visible on the ‘shop floor’ was highlighted by all participants. This visibility was reported as enhancing the relationship between the therapy role and those in senior medical and nursing roles, as well as demonstrating the direct impact of input on patient care. This visibility extended to increasing the wider recognition of input by therapy staff of all levels, with promotion of work that they are doing through relevant local and regional forums.
I04: You’ve got to be present. You’ve got to be part of the conversations that are happening on a daily basis.
Trust, and the need to be trusted, was reported by all participants, and that trust was earned through years of experience and the impact on patient care. This consistency of staffing over prolonged periods of time was highlighted as important in raising the profile of the individual and achieving the required level of developmental support to be effective in the role.
I05: And it does take time because trust generally takes time to build. . .if you can be a trustworthy member of staff and you know you’ve got some credentials, people have seen you, that you don’t come and go. . . my impact can be quite big because they trust me
Discussion
This study is the first exploration of consultant-level therapy practice within critical care in the United Kingdom. Whilst a very niche focus, this study has provided insight into the roles undertaken by the therapists working at this level and starts to demonstrate some of the potential impacts on patient and service outcomes, as well as the wider contributions to research, education and strategy. Importantly, the study also demonstrated that these suggested benefits are seen by the wider multi-professional team, specifically those in senior medical and nursing roles.
National guidance outlines different levels of practice undertaken by non-medical healthcare professionals from supportive to consultant-level,12,13 with additional guidance focusing specifically on consultant-level.3,6 Consultant-level practice is formed around 4-pillars of practice 3 (5-pillars within NHS Wales with ‘strategy / strategic service development’ being identified as an independent pillar opposed to integrated into the other pillars 6 ). Recent capability programmes have suggested the potential scope of consultant-level roles across these pillars practice.14,15 However, this study has provided further evidence of key themes of practice that are essential to consultant-level working and given valuable insight for future service planning and role development within critical care.
The overarching ethos of the national guidelines and capability programmes were reflected through the findings of this study, with all 4-pillars suggested as being central to the role within critical care. However, the composition and time commitment to each of these pillars appears varied. Expert clinical practice was recognised by both AHPs and medical and nursing participants, however the involvement in education and research was more nuanced. Research was of particular interest, with a clear difference across AHPs as to whether there was a need to be leading research. This was then reflected in the focus group with some reporting the clear benefits of the role in increasing research activity, but less apparent for others. Interestingly, contribution to education was only reported by the AHPs, which is potentially a reflection of the unseen nature of this element but also suggests an opportunity for greater involvement in multi-professional education for all levels of staff from newly qualified to most senior.
The nuanced nature of consultant-level practice has been identified by other healthcare professions. In an exploration of nurse consultant roles, three domains of impact were identified: clinical significance; professional significance; and organizational significance. 16 Whilst all nurse consultants recruited reported some evidence of impact in all three domains, the primary focus varied across the different nurse consultants depending on organisational demand and personal preference. Similar findings were also reported by Stevenson et al. 2 In their qualitative exploration of consultant-level practice, which including five nurses, a physiotherapist, and a pharmacist. The authors reported four domains of discussion: (1) role interpretation; (2) role implementation; (3) role impact and (4) challenges including lack of organisational and administrative support. Again, the focus towards each of these domains was varied, as well as the bias across the 4-pillars of practice. Of note, the final domain, ‘challenges including lack of support’, deviates from the findings of the current study, which suggests high levels of reported organisational support. However, this may be due to participant selection. In the current study, senior medical and nursing staff were only recruited from organisations with consultant-level AHP posts, and therefore were inherently more likely to be supportive.
Providing role clarity, even with a degree of nuance, is essential for ongoing development. As highlighted in the findings. the use of the title ‘consultant’ has potential for misrepresentation or misunderstanding. For non-medical roles, the use of the term consultant, reflects the level of practice in which the role operates (hence the use of ‘consultant-level’ throughout this study). Definitions exist for this level of practice [6–8], however, further work is clearly needed to highlight this and provide greater understanding of such roles to both the wider multi-professional team, service users and the wider public.
As with many areas of practice, non-medical consultant roles are few in numbers, but the potential impact is becoming more apparent.2,17 The current study has supported these findings but also highlighted the challenges to these roles including the perceived demands on the individual, that is, low numbers of roles trying to maintain local, regional, national and international profiles. This also poses several different questions, including creating an understanding of the potential number of roles needed within specific areas like critical care, or indeed numbers needed across a healthcare organisation to ensure the impact is maintained.
Through the focus groups and interviews, it was suggested that those organisations with consultant-level AHPs had better levels of AHP workforce that those without. Confirming this suggestion would require further exploration beyond the previous workforce surveys4,5 but would be beneficial. If this is the case, then the reasons for this impact would be of interest. Particularly is it a case of greater organisational support or financial support for AHP roles, or do the consultant-level AHPs raise the profile of AHPs in general and hence create more roles? The latter also being suggested through the findings of this study, with a clear focus of consultant-level AHPs on supportive leadership and the development of others. With these roles providing aspiration and opportunity for ongoing development, whilst acknowledging that the barriers of expectation may be unrealistic or over exaggerated.
This study identified four core themes, with personal characteristics as a central element. These personal characteristics were apparent across all aspects of discussion, particularly the importance of experience and the need to be highly visible within the critical care environment to have the desired impact. During the focus groups with medical and nursing participants, questions were raised as to how these consultant-level posts are created. Particularly, whether they are created for specific individuals to maximise their potential or purely in response to service need. This becomes a key factor in defining the roles undertaken and the nature of impact, as the individual, and the individual’s interests and motivations becomes a major influencer. This was also reflected in the ‘scope’ theme, with perceived focus on local, regional and national profiles of these posts. In this context, these roles may be hosted by a healthcare institution but there must be an acceptance that there will likely be requirement for working outside of the organisation for the potential wider benefit of AHPs working in critical care. This need has also been highlighted in literature exploring consultant-level roles outside of critical care.17,18 The challenges of the above were also highlighted, including the time pressures and need for prioritisation to ensure achieving the requirements of the employing organisation whilst being ‘available’ to lead and influence national workstreams. Further work is clearly needed to provide the wider multi-professional team with an understanding of the purpose of consultant-level therapy roles and the role development.
Limitations of this study are recognised. The number of participants was small, however to our best knowledge, recruitment of five consultant-level AHPs working in critical care accounts for 75% of those that were eligible for recruitment in the United Kingdom, with only dietetics, physiotherapy and speech and language therapists currently represented at this level of practice. Furthermore, we believe we achieved theoretical sufficiency, with ample richness, depth and diversity of findings.11,19 However, we recognise the number of participants in the focus group was also relatively small and below the proposed sample size. As such it may not have reached the same level of theoretical sufficiency. This was a result of unexpected recruitment challenges. It is also recognised that those involved in the focus group were recruited via the AHPs themselves. The potential bias of this was reduced by inviting multiple staff to be involved however it is likely that those attending had the most interaction with the consultant-level AHP or may have been involved in the development of the post, and as such may have been more positive in the discussions. We also recognise potential bias during the interview and focus group process with all being conducted by LJ. This decision was made to ensure the lead research did not influence the discussions within their role as a consultant-level practitioner, but in doing so, other biases may be present including a desire to demonstrate the benefits of consultant-level roles and hence increase these roles in the future. However, if bias present, the use of the interview and focus groups should have reduced the impact.
Future research should focus on determining the impact of these consultant-level AHPs on other members of the multi-disciplinary team including AHPs working at the various levels of practice. Additionally, findings of this study should be compared to the perceived role of consultant-level AHPs working in other areas of practice, particularly outpatient and community settings, as well as comparing to consultant-level posts held by other professions such as nursing. The findings could then be used to support development of future national guidance and job planning across multiple sectors of healthcare.
Conclusion
This is the first study in the UK to explore consultant-level therapy practice in critical care. Through four core themes and a central element focused on personal characteristics, this study highlighted perceived impacts of consultant-level AHPs working in critical care, their roles and responsibilities, and their contribution to local, regional and national workstreams. The findings support the 4-pillar approach to practice, with expert level clinical knowledge and research involvement particularly highlighted. Where these roles exist, they are well received by senior medical and nursing staff, reporting the benefits of highly experienced members of clinical staff to improve service delivery. This study, in conjunction national guidance and frameworks can be used to promote the development of future consultant-level AHP roles, including the importance of nuanced job planning designed to meet patient and service needs within the host organisation.
Supplemental Material
sj-docx-1-inc-10.1177_17511437251326776 – Supplemental material for Qualitative exploration of consultant level therapy practice in critical care
Supplemental material, sj-docx-1-inc-10.1177_17511437251326776 for Qualitative exploration of consultant level therapy practice in critical care by Paul Twose, Ella Terblanche, Laura Jones, Gabriella Cork and Una Jones in Journal of the Intensive Care Society
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
The study was approved by the Health Research Authority (HRA) and Health and Care Research Wales (HCRW) on the 9th of April 2024 (Ref: 24/HCRW/0007, IRAS 340616). Research ethics committee (REC) approvals were not required as only NHS staff were recruited.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.