
Abstract
Background:
Understanding the degree to which patients are actively involved, confident and capable of engaging with self-management and rehabilitation could be an initial step in guiding individualised supportive strategies for people after critical illness.
Aims:
To assess the levels of active involvement with self management among ICU survivors using the Patient Activation Measure (PAM), explore associations between patient characteristics and PAM results, and investigate its relationship with patients’ support needs at key transition points during the recovery process.
Methods:
Eligible participants received both the PAM and Support Needs After Critical care (SNAC) questionnaires by post. The return of the completed questionnaires was considered as consent to participate. Ethical approval was obtained (17/NI/0236). Descriptive statistics were used to summarise the data and Pearson’s coefficient for correlations between variables.
Findings:
There were 200 completed PAM and SNAC questionnaires. PAM scores showed that levels of active involvement with self management fell into level 1 (n = 64; disengaged and overwhelmed, low confidence to self manage) and 2 (n = 70; still struggling), with considerably less participants achieving scores in level 3 (n = 51; taking action) and 4 (n = 15; pushing further). Lower patient activation levels were associated with higher support needs (r = −0.16, p = 0.02).
Conclusion:
We found that patient activation levels are low implying low knowledge, skills and confidence to self-manage after critical illness, and also that patients have support needs at various timepoints during recovery. Future research should focus on a longitudinal study to track changes in activation and support needs in the same patients over time and identify effective strategies to optimise recovery after critical illness.
Keywords
Background
Survival following critical illness is associated with a complex interaction of new and long-term physical, psychosocial and cognitive sequelae known as Post Intensive Care Syndrome (PICS).1 –6 Recovery is variable and unpredictable and the societal and economic burden is demonstrated by protracted and incomplete recovery, high rates of early unplanned hospital readmission, late return to work and increased healthcare costs during the year post-hospital discharge.4 –6 A key international research priority is exploring how best to support ICU survivors and their families/carers throughout their recovery trajectory.7,8
Assessment of ICU survivors’ confidence and ability to actively be involved in their self-management and seek out health care support may important when addressing their health needs after ICU and optimising recovery. Patient activation encapsulates the ‘knowledge, skills and confidence a person has in managing their own health and health care’, for example, level of involvement with self-management, health promotion and rehabilitation but has not previously been examined among this patient population. 9 Highly ‘activated’ patients are more informed, engaged and confident and may experience better health outcomes and fewer health crises. Conversely, poorly ‘activated’ patients may feel overwhelmed and/or lack the confidence to make decisions to support their health.9,10
The Patient Activation Measure (PAM) has been extensively validated in various populations (e.g. patients with COVID, COPD, Cancer, Idiopathic Pulmonary Fibrosis) to identify factors associated with patient activation and better understand patients’ capability for self-management.11 –16 Factors associated with low activation have included older age, illness perception, receipt of social support and multimorbidity.16 –20 Thus, insights gained from the PAM can help health care professionals identify patients at risk of poorer self-management and tailor interventions and support strategies accordingly.9,10,21 Assessing patient activation and confidence to engage with self-management (using the PAM) alongside an assessment for supportive care (e.g. social care, health care) may enhance the prediction of high care costs and inform actions to better meet patient needs. 22 To date the PAM has not been used among ICU survivors. Understanding the degree to which patients are activated and capable of engaging with self-management and rehabilitation could be an initial step in guiding strategies to support individuals after critical illness and optimising recovery. Furthermore, understanding patients’ perspectives on the support they need would be invaluable in providing the ‘person-centred’ rehabilitation and support that is widely recommended in UK professional guidance.23,24
Support needs have been defined as ‘the additional help some adults need in order that they can live in the best way they can, despite any illness or disability they might have’. 25 We previously developed a Support Needs Assessment Questionnaire that was based on (i) a systematic review of the qualitative literature on ICU survivors’ experiences of recovery from Post Intensive Care Syndrome, 25 (ii) the Timing it Right framework that has previously been applied among survivors of critical illness and their family members26,27 and (iii) a UK-wide survey among (n = 200) ICU survivors. 28 As such, support needs categories can include informational, emotional, instrumental and appraisal needs; these may vary across the continuum of recovery, with potentially different needs at key transitions points over time.25,29 The transition points have previously been summarised using the Timing it Right (TIR) framework which describes five phases of recovery from the inpatient hospital phase through to the later discharge phases when patients have adapted at home within their community.25 –27 Conducting a needs assessment could aid in triaging care, facilitate actions and decision making, and streamlining patient care by directing patients towards existing services at the appropriate time in their recovery, while also identifying gaps in service provision.28,30
Combining assessment of patient activation (using the PAM) with a needs assessment (using the SNAC questionnaire) holds significant theoretical potential to inform the provision of timely interventions that are tailored to survivors’ readiness to engage in health-related behaviours and their specific needs. We hypothesise that there is a relationship between patient activation and support needs, and exploring this relationship could lead to improved support strategies and outcomes for ICU survivors.
Aim
The aim of this study was to assess the levels of activation among ICU survivors using the Patient Activation Measure (PAM), explore associations between patient characteristics and PAM results, and investigate its relationship with patients’ support needs at key TIR timepoints during the recovery process.
Study design
This study employed a questionnaire survey approach.
Patient selection
Participants were recruited as part of a wider study exploring patient support needs after ICU. 28 In brief, participants were identified from ICU registers/databases in four hospitals in the UK, as well as from a UK patient support group (ICU Steps, www.ICUsteps.co.uk). The sample included individuals at one of five key timepoints in their recovery trajectory aligned with the Timing it Right (TIR) framework.25,27,28 The TIR timepoints were either on the hospital ward, discharged from hospital within approximately 4–6 weeks, discharged between 7 weeks and 6 months, discharged between 7 and 12 months, or 12–24 months after their ICU stay. We aimed to recruit 200 participants from the four sites.
The study included adults over 18 years old who been admitted to the ICU in the previous 12 months (approximately) and required mechanical ventilation for more than 48 h. Participants were excluded if they required palliative care, had cognitive impairment affecting their ability to understand or complete the questions, experienced neurological events with a planned specialist care pathway (e.g. head injury unit/stroke unit), declined or were unable to provide consent.
Data collection procedure
Eligible participants received the study information (the PAM and SNAC questionnaires) in an envelope either during their hospital admission or via post following discharge. To ensure there was no influence on response rates, the patient took the envelop home to complete and return by post and a stamped addressed envelope for return postage was provided. The return of the completed questionnaires was considered consent to participate. Responses from the questionnaires were kept anonymous, and completed questionnaires were coded to retain confidentiality. A reminder was sent after 1 month to optimise the response rate.
Study questionnaires
The PAM consists of 13 questions and is scored from 0 to 100. Scores are categorised into four levels of activation (Figure 1). Levels 1 (score ⩽ 47.0) and 2 (score ⩾ 47.1 and ⩽55.1) indicate poorer self-management skills and a reduced ability to take care of one’s own health. Levels 3 (score ⩾ 55.2 and ⩽72.4) and 4 (score ⩾ 72.5) indicate higher levels of activation. 9 Increasing scores indicate increased confidence, self-management, and ability to adopt new behaviours. The PAM has been validated for both hospitalised and non-hospitalised patients.9,12,31,32
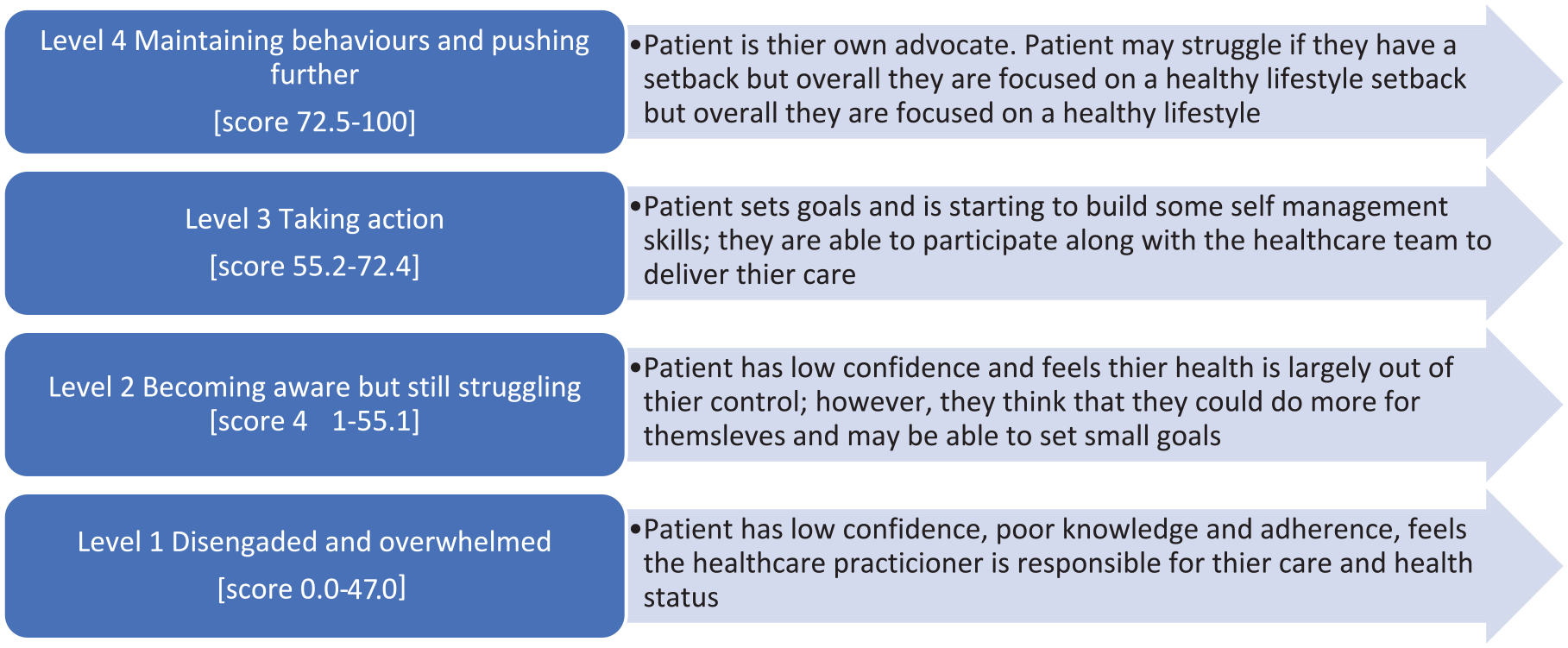
Patient activation measure: levels, scoring and description.
The SNAC questionnaire consists of thirty-two statements that assess a range of theoretically derived social support needs. It includes four categories: informational needs (12 statements: maximum score 60), emotional needs (nine statements: maximum score 45), instrumental needs (six statements: maximum score 30), and appraisal needs (four statements: maximum score 20), with an additional item capturing spiritual needs (one statement: maximum score 5). 28 Participants were requested to indicate their level of agreement with each statement on a 5-point scale (Strongly Disagree = 1, Disagree = 2, Undecided = 3, Agree = 4, Strongly Agree = 5). Scores were then calculated for each needs category as well as a total score, by summating the score for responses to each question where ‘strongly disagree’ = 1 indicating low need and ‘strongly agree’ = 5 indicating a high need. Total scores range from 32 to 160. SNAC has been validated in patients after ICU. 28
Ethical approval
Ethical approval was obtained from the Office for Research Ethics Committees Northern Ireland (ORECNI) 17/NI/0236, and relevant research governance from collaborating sites (Edinburgh, Bristol, Cambridge and the five HSC Trusts in Northern Ireland). As approved by ORECNI, patients were provided with a Participant Information Sheet which clearly indicated that return of completed questionnaires would assume consent had been given: ‘By completing and returning the questionnaires, we will understand that you have given consent to take part in the study’. Additionally, permission was granted by Insignia Health to use the PAM-13 questionnaire for the purposes of this study (License #: 1559221854-1590844254).
Data analysis
Data analysis was performed using IBM SPSS version 25 by the research team’s statistical expert (ML). The number of questionnaires distributed and returned was recorded. Descriptive statistics such as sum, percentage, mean and standard deviation were used to summarise the data. Furthermore, Pearson’s coefficient was used to explore correlations between PAM and patient characteristics at each TIR timepoint, and between PAM and SNAC at each TIR timepoint. Independent t-tests were used to explore differences between patient characteristics at each timepoint on PAM scores.
Results
Recruitment began 14th Dec 2018 and ended 29th April 2019. From 375 eligible participants, 200 (54%) PAM questionnaires and SNAC questionnaires were completed and returned. We recruited participants within each of the five transition time points (in hospital n = 19, <6 weeks n = 33, 7-weeks to 6-months n = 71, 7–12 months n = 51, 1–2 years n = 26). The average age was 57.3 years (SD 14.3); 57.5% were male; 77% lived with family or had other support; 39.5% were still working; and 95% were white.
PAM results
Figure 2 provides the PAM scores at the TIR timepoints after ICU discharge. The average PAM scores are below level 2 at all time points up to 1 year, and then level 3 at 1–2 years. Also, from hospital to 1–2 years there is a very small change in average PAM score (53.1–55.2). These scores classified patients as level 1 (n = 64) or level 2 (n = 70); level 1 and 2 imply poorer self-management skills and poorer ability to take care of one’s own health (Table 1). A smaller number of patients scored level 3 (n = 51), and level 4 (n = 15) implying confidence to take action and maintain healthy behaviours (Table 1). The percentage distribution of participants with scores at each PAM level at the various TIR time points after ICU discharge are shown in Figure 3; at each TIR timepoint smaller proportions of patients scored level 3 (18.2%–34.6%), and level 4 (3.9%–9.9%) compared to Level 1 (26.3%–39.4%) and level 2 (26.9%–47.4%).
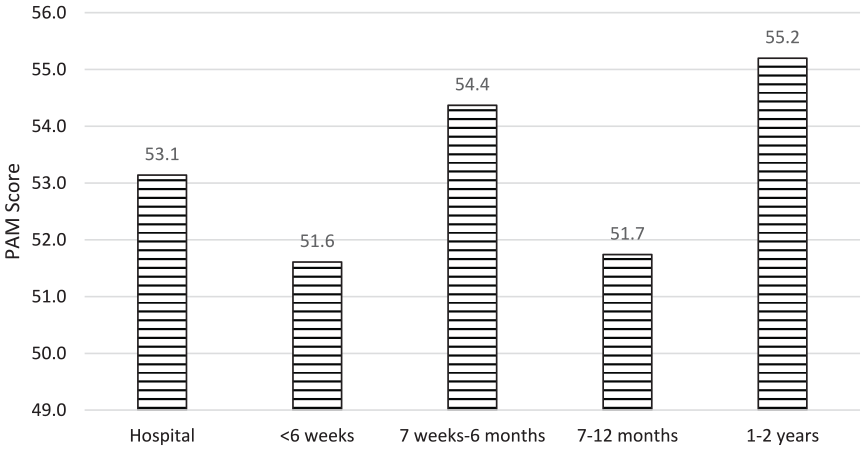
Participants average PAM scores of across various time points after ICU discharge.
PAM score and level at each recovery timepoint after ICU discharge.
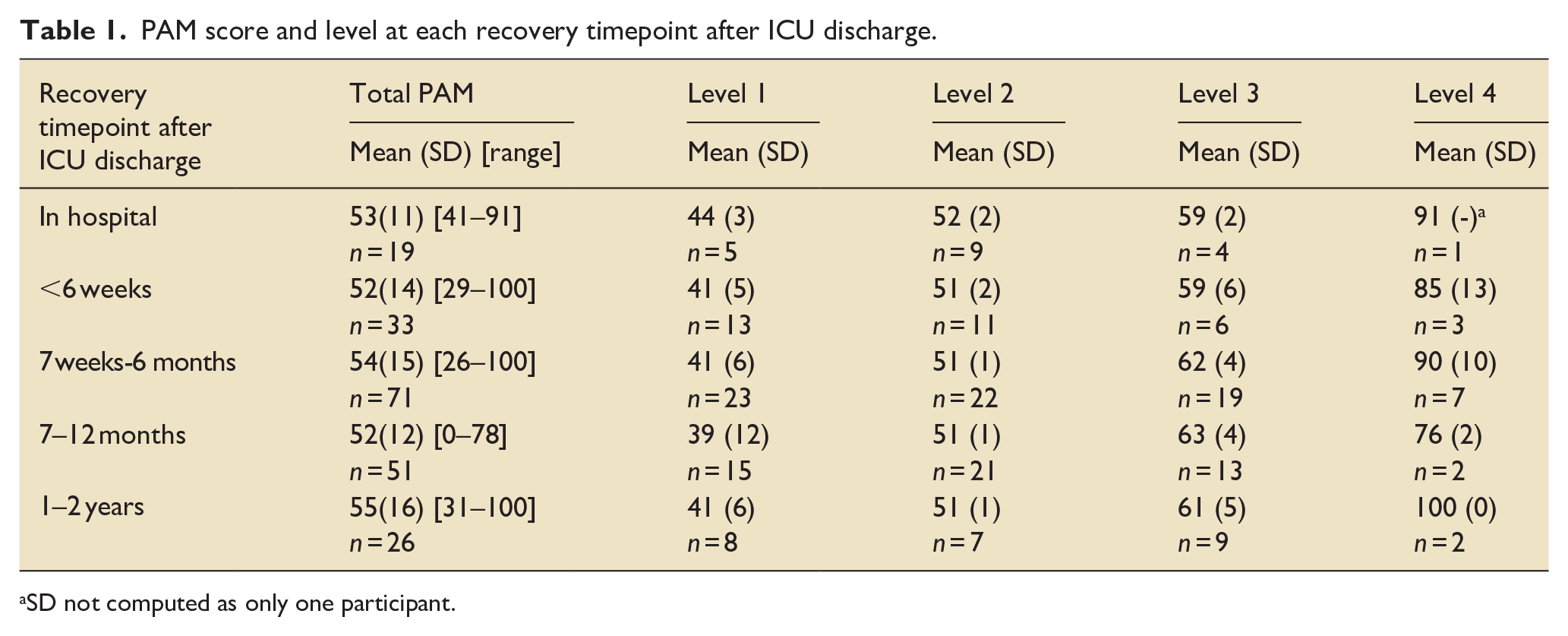
SD not computed as only one participant.
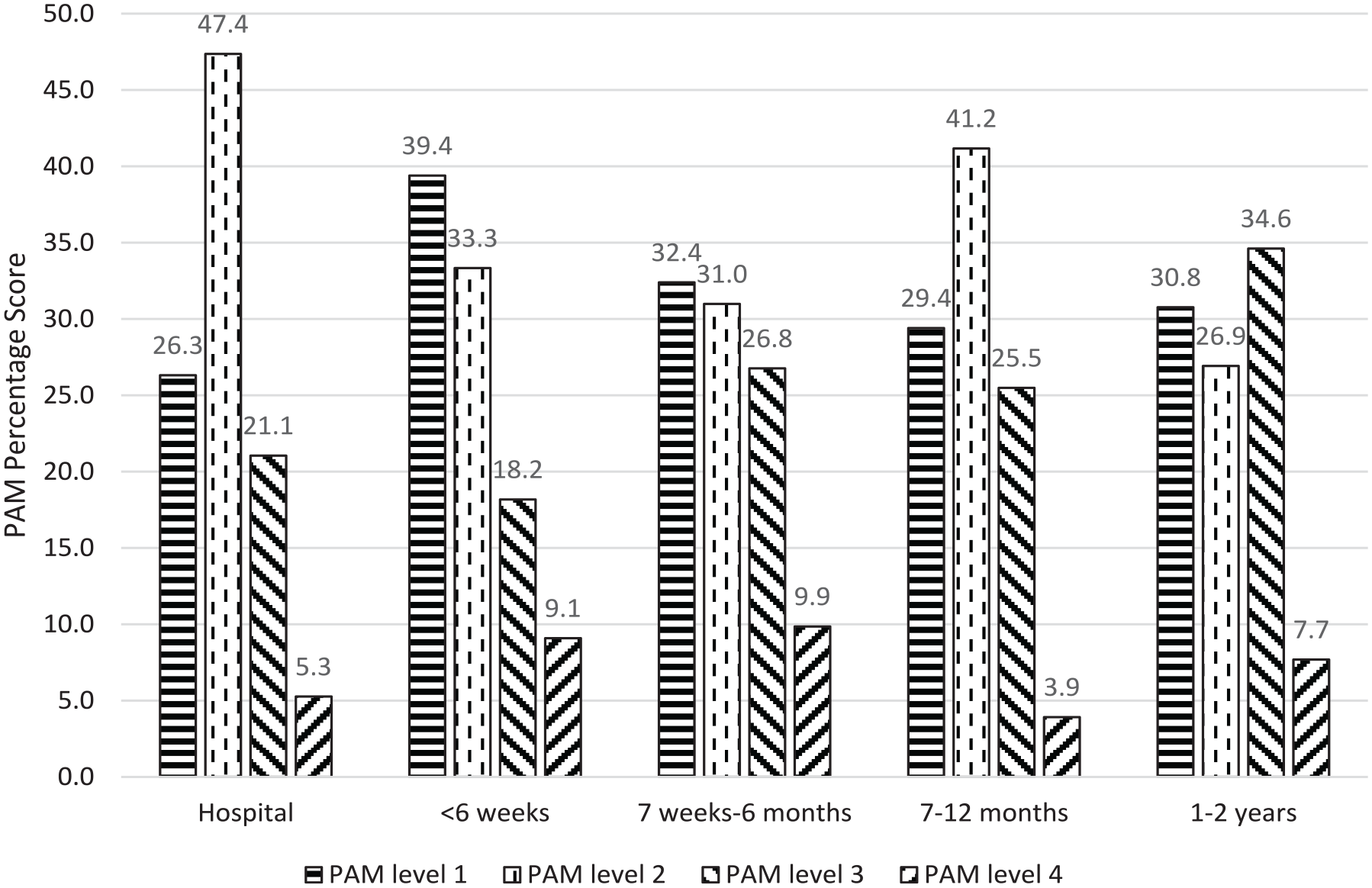
Percentage distribution of participants’ PAM scores across various time points after ICU discharge. 9
There were no correlations between PAM and age, living arrangements, or employment status at any TIR timepoint (Supplemental Material 1).
When differences were explored between patient characteristics and timepoints with PAM score there was a statistically significant difference for males compared to females at one timepoint that is, between 7 weeks and 6 months recovery (males (mean 58.24) had more needs than females (Mean 49.36) at this time point; p = 0.014).
SNAC results
Patients at each of the TIR timepoints identified needs in each of the 4 support needs categories, and some identified spiritual needs at each timepoint (Figure 4). The highest scores per category were: information needs 36/60 when in hospital; 32/45 emotional needs at 7 weeks–12 months post discharge; instrumental (physical help) needs 18/30 in hospital; 13/20 appraisal (feedback) needs at < 6 weeks post discharge and spiritual needs 3/5 in hospital. There was no significant difference between the support needs for each category (Information, Emotional, Instrumental, Appraisal) and any specific time point of recovery. There was no significant difference between the total score of the questionnaire and any specific timepoint of recovery (p = 0.116).
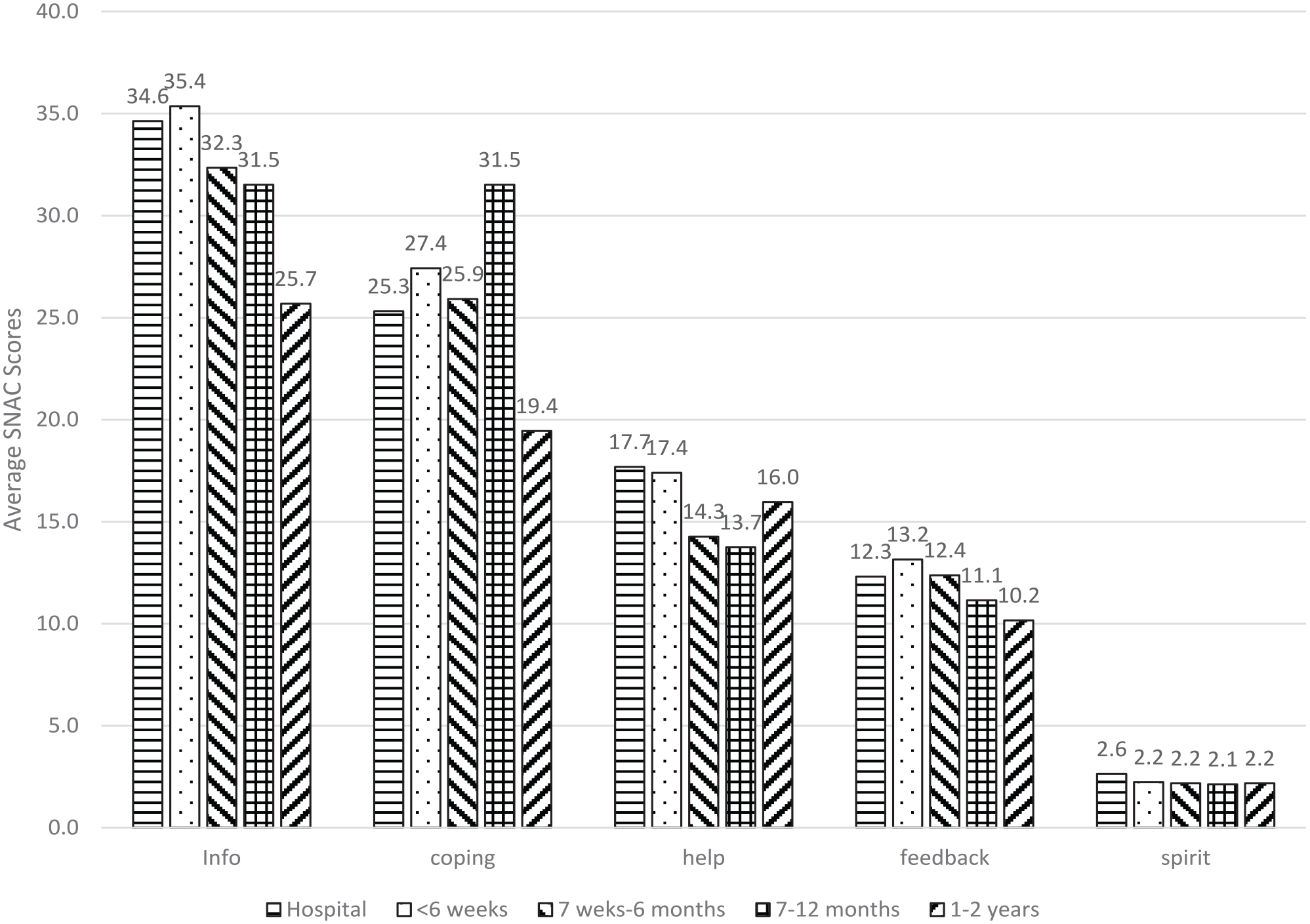
Participants’ average scores within each SNAC category across various time points after ICU discharge.
Correlation between PAM and SNAC
Lower PAM scores were associated with higher support needs and in particular, significantly higher emotional needs (r = − 0.15, p = 0.04), instrumental needs (r = −0.23, p = 0.001), and total SNAC score (r = −0.16, p = 0.02). In the <6-week cohort, lower PAM scores were significantly associated with higher informational (r = −0.36, p = 0.04) and emotional support (r = −0.41, p = 0.02). In the 7–12 months cohort, lower PAM scores were significantly associated with higher SNAC total score (r = −0.24, p = 0.04); and in the 1–2 year cohort lower PAM scores were significantly associated with higher instrumental needs (r = −0.60, p = 0.001).
Discussion
This study aimed to assess the levels of activation among ICU survivors using the Patient Activation Measure (PAM), explore associations between patient characteristics and PAM results, and investigate its relationship with patients’ support needs at key TIR timepoints during the recovery process. Using the PAM, we found that patients have low confidence and self-management abilities after hospital discharge, and this result has the potential to significantly influence the design of supportive healthcare for this population. Our study has also revealed that support needs occur at various key time points throughout the ICU recovery process, extending up to 1–2 years after hospital discharge. Identifying patient activation levels as well as their support needs could enhance patient care by directing patients towards specific services at the appropriate stages of their recovery.
A high number (134/200, 67%) of participants exhibited low PAM scores, indicating feelings of being overwhelmed and lacking confidence in self-management or seeking necessary help and healthcare. Health professionals can play a crucial role in assisting these patients to feel less overwhelmed and become more engaged in their recovery and rehabilitation interventions. The specific PAM level attained by a patient can guide healthcare professionals in the selection of the most appropriate approach to delivering interventions. Research in patients after thoracic and abdominal surgery has shown that low patient activation measured at one timepoint that is, hospital discharge was associated with higher healthcare costs and readmissions, 33 and there is also some evidence that changes in activation levels are associated with improvements in health behaviours. 34 Therefore, monitoring patient activation at hospital discharge and/or across the recovery trajectory could be useful for this critical care population who have high morbidity and high re-admission rates (1–6). Furthermore, even a small increase in PAM scores for example, 3–4 points, (with or without changing the PAM level) can indicate a significant change in patient engagement and behaviour, emphasising the potential for healthcare interventions to positively impact patient activation.9,10,21,35,36,39
Several studies have attempted to investigate the causal mechanisms of patient activation, suggesting that emotional state influences an individual’s level of activation. For example, in COPD patients, anxiety levels, disease severity, and comorbidities play crucial roles in determining activation levels and should be considered when designing self-management interventions for this population. 12 Similarly in our study, a substantial proportion of patients reported emotional support needs, particularly at 7–12 months after hospital discharge, and lower PAM scores were significantly associated with higher emotional needs, especially in the cohort discharged within 6-weeks. Emotional and mental health sequelae often emerge later in the post ICU recovery trajectory.1 –3 As such, future post-ICU self-management or rehabilitation interventions should include strategies to support patients in coping better during their return to daily life.
Research in other health care populations and settings support the use of needs assessment tools, enabling patients to explicitly identify support needs that may otherwise go unnoticed. These assessments empower health care professionals to recognise and provide appropriate care and rehabilitation for each patient.13,15,26,36 –39 For example, our study identified information needs at each of the five time points. While resources are available to address these needs, access might be problematic, and the timing of when the patients feel confident and ready to receive specific information must be considered, along with the volume of information and health literacy levels.
In this study, we observed that poorer self-management, as indicated by lower PAM scores, was associated with higher support needs, as reflected in higher SNAC scores. By combining PAM and SNAC, theoretically there is potential for health care professionals to identify patients who have high needs and who are at risk of poorer self-management, and tailor interventions accordingly by aligning them with individual patient activation levels (Figure 5). For example, strategies to address low confidence and self management could include for example, peer support, individual goal setting, skills development. Even though this was not a longitudinal study, support needs were evident at each stage of the TIR timepoint, even up to 1–2 years after discharge from hospital, although PAM scores seemed to improve slightly at this stage. Future research should explore factors and patient characteristics that contribute to improved confidence and activation during late stages of recovery, in addition to exploring interventions that enhance confidence early in the recovery process.
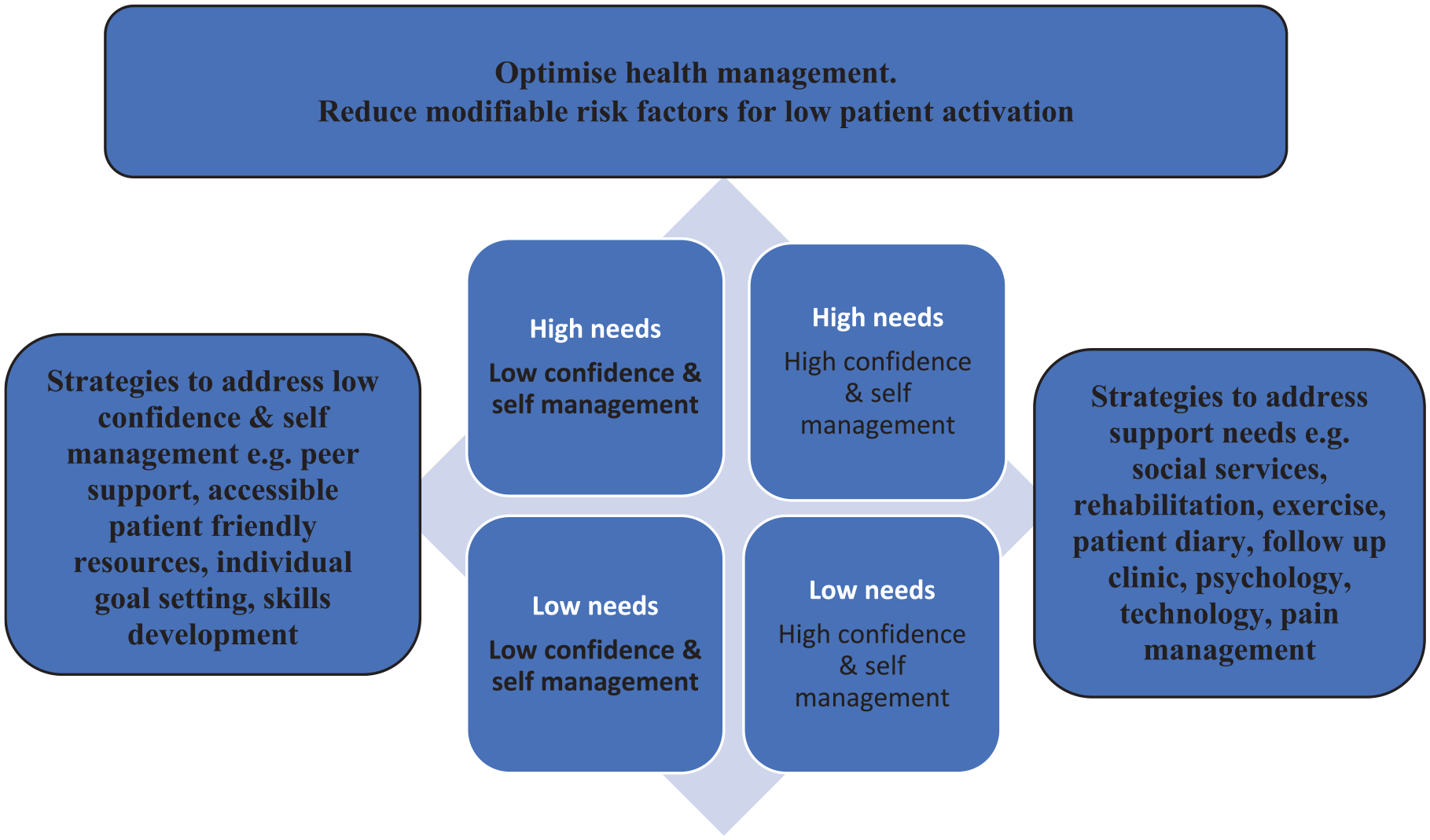
Proposed example of a hypothetical support and rehabilitation model combining patient activation (self-confidence) and support needs.
Strengths and limitations
This is the first study to provide data on the PAM in this population and we have been able to been able to show that low activation and low confidence to self manage is common after critical illness. However, the study’s main limitation lies in the inability to follow the same patients longitudinally over time to assess any changes in activation levels or support needs across the recovery continum. 28 Although we recruited participants at each TIR time-point there were unequal numbers of respondents at each group, and this may have influenced our results and interpretation; also, when the numbers when broken down into groups they were then too small for meaningful statistical analysis. Regarding the SNAC questionnaire, we established that support needs exist at each of five time points in each cohort and a recent review of qualitative studies reported changes in social support needs among ICU survivors change as they transition from ICU to living at home again. 25 Therefore, a future longitudinal study also employing the SNAC questionnaire could identify evolving patient needs, factors influencing any resolution of needs (e.g. patient activation), and the timeframe required for resolution.
A further limitation is that post ICU care could have changed since the administration of our study. A survey capturing the time period of our survey has shown that although the number of follow up clinics have increased across the UK, the provision of post ICU rehabilitation is still low (31/176, 18%) giving confidence that our results are still relevant. 40
Our survey achieved an overall response rate of 54% demonstrating moderate effectiveness and efficiency of postal distribution with one postal reminder. Future research should employ additional strategies to enhance response rates such as online completion, telephone reminders, additional recruitment sites, and home visits, as well as proactive strategies to optimise recruitment from a more ethnicity diverse population guided by the INCLUDE Ethnicity Framework. 41
Conclusion
We found that patient activation levels are low implying low knowledge, skills and confidence to self-manage after critical illness. Also, lower patient activation levels were associated with higher support needs (informational, emotional, instrumental, appraisal, spiritual needs) in these patients. Understanding and addressing patient activation and support needs are critical steps in supporting ICU survivors’ recovery and improving their long-term outcomes. By combining the insights gained from the PAM and SNAC questionnaires, healthcare professionals have the potential to implement personalised and targeted interventions that foster patient engagement, self-management, and overall well-being. Future research should focus on longitudinal studies to track changes in activation and support needs over time and identify and test effective strategies to optimise recovery after critical illness.
Supplemental Material
sj-docx-1-inc-10.1177_17511437241305266 – Supplemental material for Patient activation and support needs in patients after ICU discharge: A UK survey of critical illness survivors
Supplemental material, sj-docx-1-inc-10.1177_17511437241305266 for Patient activation and support needs in patients after ICU discharge: A UK survey of critical illness survivors by Brenda O’Neill, Mark A Linden, Pam Ramsay, Alia Darweish Medniuk, Joanne Outtrim, Judy King and Bronagh Blackwood in Journal of the Intensive Care Society
Footnotes
Acknowledgements
It was supported by the Northern Ireland Clinical Research Network-Critical Care [Altnagelvin: A Campbell (PI), S O’Kane); Antrim: P Johnston (PI), E McKay, O O’Neill; Royal Group of Hospitals: J McNamee (PI), A O’Neill, K Ward, JMcCann; Craigavon Hospital: C Shevlin (PI) D McFarland; Ulster Hospital: J Trinder (PI) S Hagan. Also, C McCulloch, D Hope, NHS Lothian; and A Ramesh and A Timpson, Southmead Hospital Bristol. Thank you to all patients who participated.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Intensive Care Foundation Research Priority Award, UK.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.