
Abstract
Background:
ICU-survivors are likely to struggle with psychological wellbeing. Providing post-ICU therapeutic interventions is a relatively novel field and little is known about patients’ experiences.
Methods:
Thematic analysis was used to analyze semi-structured interviews with 20 ICU-survivors who had accessed psychological therapy following discharge from an ICU in the Southwest of Britain. Descriptive statistics were used to summarize data to provide service related contextual information.
Results:
Five themes emerged from the data: the impact of critical illness, value of therapy, accessing therapy, process of therapy and role of psychologist. Psychological therapy is viewed as an important part of recovery. Critical illness is a complex experience. Therapy supported sense-making, acceptance and moving forwards. Although therapy could be initially difficult, there were lasting positive effects. There were different challenges to and facilitators of accessing therapy and offering ongoing support provided reassurance. A safe therapeutic relationship and an ICU-specific service was important.
Conclusion:
Psychological therapy, alongside other rehabilitation interventions, can facilitate recovery. Considerations for local and wider service development are discussed.
Keywords
Introduction
Recovering from critical illness can be complex. The estimated psychological morbidity for Intensive Care Unit (ICU) survivors is 55%: with approximately 20%–30% experiencing PTSD; 46% depression, and 44% anxiety.1 –3 Risk factors include psychiatric symptoms during admission, use of benzodiazepines, duration of sedation, frightening ICU experiences and delirium.1,3,4 Delirium is a significant risk factor and research suggests around 50%–80% of ICU patients experience delirium
Despite the recommended need for critical care psychology5,6 provision is patchy, with only 19% of UK ICUs having access to a psychologist. There is a growing interest in the provision of evidence-based critical care psychology interventions. Although guidelines indicate that psychological interventions are important in recovery post-ICU discharge,5,6 it is a relatively novel field. Much literature to date has focused on inpatient interventions to prevent further psychological distress rather than models of outpatient intervention 7 and there is little exploring ICU survivors’ experiences of follow up psychotherapy. The service evaluation was approved by the Trust’s Audit, Assurance and Effectiveness Team to record critical care psychology’s outpatient activity and to explore patients’ experiences of psychological therapy as part of outpatient follow-up care from a 27-bed adult neurological and general ICU in the southwest of Britain.
Methods
Standard practice is to send screening questionnaires to survivors with an ICU admission of 4 days or more6,8 at 3 months post-hospital discharge. The questionnaires include: Post-Traumatic Stress Syndrome 14-Questions Inventory (PTSS-14), a validated measure to screen for acute PTSD after ICU discharge (a score of 45 or more indicates clinically significant distress) 9 ; Generalized Anxiety Disorder-7 Questionnaire (GAD-7), 10 a seven-item, self-report, assessment tool validated for assessing anxiety disorders (a score of 8 or above indicates clinically significant symptoms); Patient Health Questionnaire (PHQ-9), 11 a nine-item, self-report scale used for assessing depression (a score of 11 or above indicates clinically significant symptoms); and EQ-5D-5L, 12 a five-item, self-report measure of health-related quality of life.
Screening questionnaires have been sent since 2014 and the data recorded. A psychologist joined the team in 2017 from which point patients whose scores indicated symptoms in the clinically significant range were offered a psychological assessment. An ICU multidisciplinary (MDT) follow-up clinic started in 2019 and an option to attend included with the screening questionnaires. All follow up clinic attendees are assessed by critical care psychology. Those whose score indicates clinically significant distress and do not opt to attend the clinic continue to be offered a psychological assessment. Patients can also be referred by hospital care teams, GPs and self-referral. Patients identified as experiencing ICU-related psychological distress are offered further assessment and evidenced based therapy including Cognitive Behavioral Therapy (CBT), Acceptance and Commitment Therapy (ACT), and predominately Eye Movement Desensitization and Reprocessing (EMDR) therapy.
The average number of screening questionnaires sent annually between 2014 and 2022 was 382 with an average response rate of 156 (41%). The number and percentage of returned questionnaires scoring for psychological distress was 61 of 156 (40%) and opting to attend the follow-up clinic was 69 of 156 (44%). The numbers of patients seen for follow up psychological assessment range from 37 (in 2018) to 130 (in 2022). This increase reflects the impact of starting the follow-up clinic and offering remote therapy. Across the three full years (2020–2022) since the start of the follow-up clinic 338 patients have been assessed for critical care related psychological distress, either in the clinic or by psychology alone, and of these 209 (62%) were offered psychological therapy. The number of therapy sessions per intervention ranged from 1 to 30 with a mean number of 6.3. In the same three full year period (2020–2022) 97 people were discharged by critical care psychology. Outcomes measured by questionnaires following discharge were: 34 of 97 (35%) clinically significant change (defined as scores dropping below clinical significance on at least one measure); 43 of 97 (44%) no post therapy measures collected; 18 of 97 (19%) scored below clinically significant distress at the start of therapy, therefore no post therapy measures were collected; and 2 of 97 (2% showed no significant change on post measures).
Participants for the qualitative interviews were recruited via opportunity sampling. A list was generated of patients who had received at least one therapy session as part of their follow up care between 2017 and 2020. The list was checked against hospital records and anyone who had died or was known to be in hospital was removed. The remainder were sent information sheets and a consent form. Patients were invited to a semi-structured interview (see Figure 1) about their lived experience of outpatient ICU-related psychological intervention.
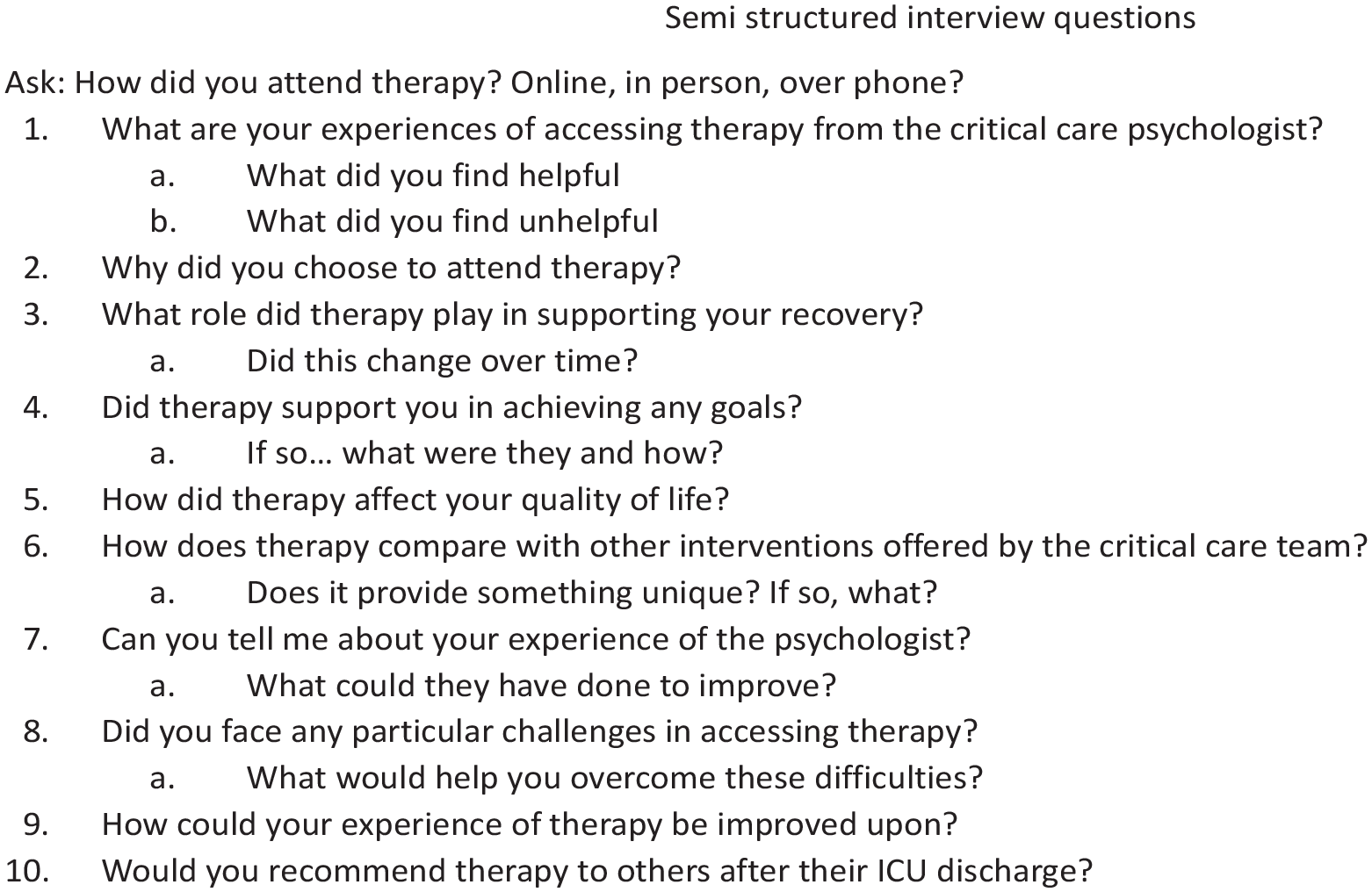
Semi structured interview schedule.
Interviews were conducted by four researchers not directly involved in participants’ care. Interviews were carried out remotely via video call or telephone, lasted 10–60 min, were audio-recorded, transcribed and pseudonymised. Interview data was analyzed using thematic analysis employing Braun and Clarke’s six step framework. 13 Data was read and re-read for familiarization, initial codes developed, including cross coding by different members of the research team and patterns established. These patterns were developed into themes, which were reviewed and defined into a final set of themes and sub-themes. Recruitment ended once data saturation occurred and no new themes emerged.
Results
About 20 patients took part. Participants were aged between 30 and 78, with an average age of 59. Participants had an ICU admission of 5–78 days, with an average of 16 days. The range of psychotherapy sessions undertaken by participants was 1–29; the average was 12. 15 participants had undertaken EMDR therapy and 5 CBT. About 10 attended therapy sessions in person and 10 remotely by phone (2) and online (8).
Five superordinate themes and 12 subthemes were identified (Table 1). Illustrative quotes are from the data, names are pseudonyms.
Themes and subthemes from analysis.
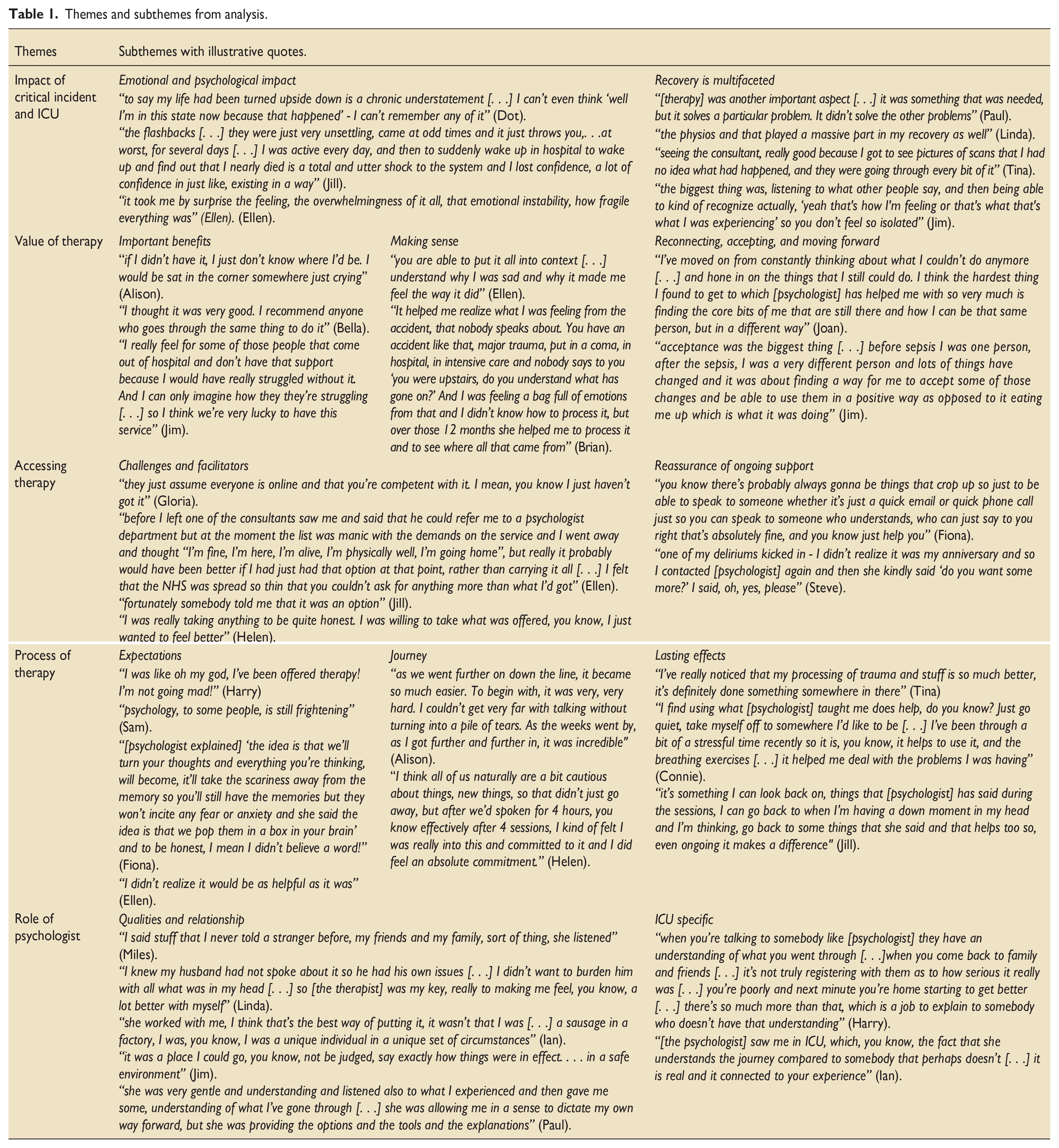
The impact of critical illness
The significant and complex impact of critical illness was core to participants’ experiences and included both physical and psychological challenges. Although the physical challenges were anticipated, the emotional impact was often unexpected. Memory of what happened is often absent or fragmented: “it was such a big thing and the awful thing about it was that I don’t actually remember what happened”; and further complicated by delirium “some of the places that you visit in your head while you’re under, is difficult. They’re real places, but you’re not there.” ICU experiences and related psychological trauma symptoms could lead to a sense of loss and a changed sense of self, which at times felt overwhelming. Some participants voiced feeling alone in recovery. Due to the complex nature of critical illness, support and recovery was multifaceted. Psychological therapy was needed in tandem with other interventions. The MDT Clinic provided the opportunity to make sense of experiences with different professionals and the unit’s Expert by Experience group provided valuable space to connect. There were also perceived gaps in care: “I wasn’t being offered any kind of what I call follow up and I thought well at least that’s one lot of follow up I can have.”
Value of therapy
Many participants felt that therapy was an important aspect of their recovery, it helped overcome some of the challenges, and some found it hard to imagine recovery without it; “it saved me.” Many recommended therapy to other ICU survivors, some were aware that similar critical care psychology services were not available everywhere and also that some people who might have benefited had not accessed the service. Therapy provided a safe space with a knowledgeable psychologist to integrate and make sense of complicated experiences; “the first thing that I found particularly helpful is just being able to talk to somebody and understand, first of all, what had happened to me, but secondly . . . . . . that I’d gone through delirium, but that wasn’t unusual. . . what I had experienced was quite normal, even though. . .it was a very strange experience.” Therapy facilitated a greater understanding of the impact of psychological trauma, reduced the intensity of related symptoms, and integrated experiences. Participants described ICU-related experiences as difficult to understand, with often little opportunity to speak about. Therapy facilitated accepting and moving forwards; “I was struggling with certain things that would trigger difficulty breathing and a sense of anxiety and panic and the therapy actually helped me to address that and to almost eliminate it so that I was able to sort of come back to normal again.” Critical illness and ICU often shook participants sense of self and the world. A transformative aspect of therapy was being able to reconnect with their core values and who they wanted to be within the new circumstances in which they found themselves. All participants described changes which were difficult to come to terms with. Therapy supported a move toward acceptance and provided avenues for the future.
Accessing therapy
Challenges and facilitators were unique to each participant. Some discussed logistical difficulties, such as location of the hospital, parking, getting time off work. The hospital environment could be a trigger in itself and remote appointments were welcomed. However, others faced technical difficulties: “I’m no good with technology it annoys me.” Some would have preferred being offered therapy earlier, although others reflected that they may not have been ready had they been invited earlier. Some had accessed the service via other professionals and guilt and worry about overstretching services could be a barrier. A key shared motivator was the need to feel better; “I kind of just took it up just on the off chance that maybe it might have helped me in some way.” The psychology service offers an open-door policy of additional support if needed following discharge. Many participants described this as an important feature and often this reassurance offered containment: “it’s there if you need it again, it does help, it’s something that you can fall back on.” For participants who had accessed this ad-hoc support, a quick response was helpful to restabilise and support ongoing recovery.
Process of therapy
Participants described different expectations of therapy and often being unsure what to expect. Some participants had previous therapy experience whilst for others therapy held stigma. Many described finding the concept of EMDR strange and being unsure: “I was very open to it, I mean I was like, I gave myself to the therapy.” For some therapy was better than they had anticipated: “I didn’t realize it would be as helpful as it was.” Many described the journey of therapy as initially difficult, but with often surprisingly quick changes with lasting effects. Some participants shared that the process of EMDR was preferable to other therapies: “I preferred EMDR, it’s less intrusive in that sense, but it doesn’t want you to relive your experience from talking directly about it. It leaves a lot of it up to your own inner thoughts.” Participants described learning new ways of coping and feeling empowered to adapt and use these as needed. Many described an internalized psychologist’s voice and the strength this gave them to overcome challenges.
Role of psychologist
Participants described aspects that they found helpful: a trusting relationship; the chance to speak with someone outside of close relationships and not feel like a burden on loved ones: a safe space to connect with difficult emotions; and feeling supported by someone with skills and knowledge, whilst being empowered to go at their own pace. Many participants described the additional benefit of having a psychologist who was based within ICU. This added an additional layer of expertise and understanding: “it was good to speak to somebody . . . . who’s dealing with patients’ all the time, kind of probably seeing similar patterns that I don’t get to see.” Some participants had met the psychologist whilst an inpatient allowing for a more integrated experience.
Discussion
The service evaluation explored the lived experiences of critical care psychology follow up interventions which included EMDR, CBT and ACT. Although there is no National Institute for Health and Care Excellence (NICE) recommendation for psychotherapy related to post-intensive care syndrome there are guidelines for anxiety 14 and depression 15 which can be adapted to the ICU-survivor population. EMDR is a recommended therapy for PTSD 16 which facilitates processing of traumatic memories or memory fragments. 17 Clinically EMDR lends itself to critical care experiences where survivors do not have a chronological narrative of what happened and are most traumatized by delirium experiences. 18 EMDR can be utilized to process traumatic images and memories which underpin a range of presentations from adjustment disorder to PTSD. Interventions from the third wave of CBT were utilized such as behavioral activation, a recommended intervention for depression, CBT protocols for generalized anxiety,19–21 and ACT therapy which has a strong evidence base in physical health settings.22–25 ACT sits under the overarching cluster of therapies defined as CBT; whereby thinking processes are incorporated into functional analysis of behavior. 26 The shared features for third wave CBT interventions include mindfulness, learning to let go of unhelpful thinking processes, values based activity, and sitting with difficult thoughts and feelings.
Findings indicate that therapy was a positive experience helpful in recovery for many reasons. Echoing previous literature,27,28 all participants were significantly impacted by their critical illness and these experiences were often difficult to come to terms with. Many patients struggled to consider what life would be like without therapy, and for several, therapy had been lifesaving. Many participants were unsure of what to expect and most described the start of therapy as difficult. Most had undertaken EMDR, the process of EMDR with ICU survivors has been described in publications and there is an emerging evidence base.29–32 Generally EMDR is an effective and efficient therapy with a growing evidence base for remotely delivered EMDR.33–37 Many participants were referred for therapy via the follow up clinic, whilst others accessed it through other professionals, highlighting the importance of joined up care. “Survivors” guilt’ has been identified post-ICU 7 and for some it led to delay accessing treatment. The role of the psychologist was important for multiple reasons, including providing a safe space where participants could be vulnerable and understood, echoing the importance of the therapeutic relationship within effective therapy. 38 Many participants expressed the value of the psychologists’ knowledge and understanding of ICU, which was felt to be an additional lens of understanding. For some participants who had met the psychologist as an inpatient, outpatient support felt like a smoother transition. This adds evidence for psychological provision embedded across critical care services.
Several patients who attended the follow up clinic did not score for clinically significant distress but were nevertheless assessed as experiencing post-ICU psychological distress and offered related interventions, a presentation probably best understood as adjustment disorder or sub-clinical PTSD symptoms. Where pre and post measures were completed there were indications that post-ICU evidence based psychotherapy can achieve clinically significant recovery for a significant proportion of patients despite often experiencing ongoing physical health difficulties, which may be life-altering or life limiting in nature. This process has highlighted the need to ensure more consistent use of post therapy outcome measures.
Psychological morbidity has a significant impact on quality-of-life post ICU39,40 The psychological impact of COVID-19 is an area for further research. Despite the evidence of post-ICU psychological morbidity and national policy around the need for psychological assessment and intervention,6,8 benchmarking indicates that the majority of UK ICUs do not have access to a psychologist 41 and very few offer post-ICU evidence based psychotherapeutic interventions. The findings of this service evaluation indicates the potential value of doing so.
Strengths and limitations
The data is limited; therefore the sample of participants may not be representative of all those seen by the psychologist and it may be that people who had positive experiences were more likely to participate. There is currently a paucity of research regarding psychological intervention following critical illness, including research seeking to understand and explore the lived experience of such interventions. The service evaluation adds valuable information to the currently limited field and gives important insights as to why therapy is significant within recovery.
Recommendations
There is limited evidence that psychologically informed interventions whilst in intensive care prevents the development of ICU related PTSD.42,43 Despite this most research focuses on the prevention of PTSD; therefore, there is an absence of guidelines on delivering therapy with the ICU survivor population. 7 Research is needed to evaluate post-ICU evidence-based interventions, and explore cost-effectiveness including possible enhanced ability to manage ongoing physical health. This paper reflects one unit’s experience which may facilitate other ICUs to conceptualize their potential critical care psychology service development options. It is important to ensure optimal access for people experiencing post-ICU psychological distress, providing different routes into the service. Offering follow-up, validating experiences, and encouraging accessing therapy helps ensure early treatment and prevention of challenges becoming entrenched. As services adapt to hybrid models of working, providing accessible options is important, as is ensuring that patient choice is held at the center of therapeutic work. Recovery following critical illness is multifaceted; therefore, intervention needs to target the multiple areas of patient’s lives which have been affected. Integrating psychologists within critical care rehabilitation teams including follow up can ensure patients receive vital treatment from experienced clinicians who understand the context of such a specialist environment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.