
Abstract
Background:
Animal-assisted interventions (AAI) can provide psychological support to critical care patients during their intensive care unit (ICU) admission. However, there are currently no data on AAI services across UK ICUs. The current study therefore aims to (i) determine how many ICUs in the UK offer services, (ii) characterise available services and (iii) explore and review local documentation for service oversight.
Methods:
A service evaluation comprising two parts; a national survey of UK ICU’s, analysed using descriptive statistics, and review of local service oversight documents, analysed using a framework approach.
Results:
Responses from 74 sites (/242, 30.6%) were included in survey analysis. AAI services were present at 32 sites (/74, 43.2%), of which 30 offered animal-assisted activity services alone and 2 offered both animal-assisted activity and animal-assisted therapy services. Animal-assisted activity services were typically delivered on a weekly basis, lasting 30–60 min and with dogs the sole animal employed. Concern over infection prevention and control was the most common barrier to service provision, as well as a lack of supporting evidence. Sixteen sites provided 27 oversight documents for analysis, that highlighted unique and shared responsibilities between critical care staff and animal therapy handlers, including aspects of administration, welfare and infection control.
Conclusion:
From a small sample, AAI services were available in less than half of ICUs. Empirical value of interventions is countered by current lack of definitive evidence of effectiveness, which should be addressed before wider implementation of AAI services and the associated resource requirements, is undertaken.
Keywords
Introduction
Critically ill patients in the intensive care unit (ICU) can experience varied psychological sequelae including, but not limited to, anxiety, depression, post-traumatic stress disorder and loneliness.1,2 In recent years, animal-assisted interventions (AAI) - the involvement of trained therapy animals under the supervision of staff and volunteers – have been employed to provide psychological support to patients during their ICU admission, an example of a non-pharmacologic intervention to enhance humanisation and holistic care. 3 Under the overarching AAI term, distinction is made between animal-assisted activity (AAA) where a volunteer handler brings a trained animal to the patient for general interaction (e.g. ‘meet and greet’ style episodes of therapeutic, motivational, or educational benefit), and animal-assisted therapy (AAT) involving use of a trained animal by healthcare professionals to address individualised patient requirements with subsequent measurable goal-directed activities that are documented and evaluated.4,5
The novelty of AAI in the critical care setting is reflected in a recent scoping review; only six studies were identified, all of a feasibility or observational design and with five published since 2019. 6 Notably, only one of these studies was from the UK and focused on the paediatric intensive care setting and population. 7 All other studies included in this scoping review were conducted in North America,8 –12 of which only two were exclusive to the ICU setting8,12 and the remainder were a combination of ICU and other acute or ward settings. Studies demonstrated significant variability in AAI intervention, but were typically meet-and-greet interactions. 6 Summary descriptive synthesis of findings from all studies indicated that outcomes including pain, 11 and anxiety and stress,8,11 were all reduced in patients. Clinician factors including morale and stress were positively impacted, both through direct survey assessment of staff and qualitative observations from therapy animal handlers. 9 Very high levels of support for continuing or expanding AAI services was also identified.7,9,11,12 The prevalence of anecdotal evidence in this scoping review underpinned the main conclusion that further research was required to determine effectiveness of AAI interventions, their acceptability for patients, family members and clinicians, and potential impact for the wider management of patients. 6 One further study published just after this scoping review, found that in a small single group located in acute care, an animal-assisted therapy programme reduced anxiety, heart rate and respiratory rate, and improved subjective measures of comfort and wellbeing. 13 A further, more recent study showed positive safety, acceptability, and clinical outcomes, also adopted an observational design and again focused on paediatric critically ill patients. 14 Nonetheless, national guidance from organisations such as the Intensive Care Society 15 and Royal College of Nursing – highlights the importance of implementing AAI services across adult UK ICUs. However, there are currently no data on provision of AAI services across UK ICUs for adult critically ill patients. Therefore, the aim of this study was to conduct a national service evaluation of current AAI services across UK ICUs, to (i) determine how many ICUs in the UK offer services, (ii) characterise available services including, for example type, format, extent, personnel involved and (iii) explore and review local documentation for oversight of available services.
Methods
Design
This study is a service evaluation comprising two parts16,17; a national survey of UK ICUs, and a review of local service oversight documents. It is reported in keeping with the Checklist for Reporting Results of Internet E-Surveys. 18
Sample
The sample frame for the service evaluation was all hospitals with adult NHS ICUs across the UK (England, Scotland, Wales and Northern Ireland). These were identified via the Intensive Care National Audit and Research Centre (ICNARC) Case Mix Programme, https://www.icnarc.org/Our-Audit/Audits/Cmp/About/Participation) and the Scottish Intensive Care Society Audit Group (https://www.sicsag.scot.nhs.uk/index.html). Individual ICUs were reduced to generate a denominator of unique hospitals (n = 242).
Development of national survey
A predominantly closed-question, online survey was designed in Microsoft Forms with questions generated from experience and expertise of the research team as well as informed by available evidence related to AAI in critical care (see Supplemental File 1). Survey questions were sequentially ordered with single or multiple response options, and inclusion of free-text options for further detail where applicable. Filtering functionality ensured respondents were presented with appropriately ordered questions based on preceding responses. Pilot testing, to ensure content, construct, and face validity, and sensibility, was undertaken internally within the research team, and externally by a group of multiprofessional critical care clinicians with interest and knowledge of the topic; this ensured (i) comprehension and interpretation of questions, (ii), flow, salience, acceptability, and ease of completion, (iii) missing items of response options and (iv) time required to complete. 19 This process mirrors previous surveys conducted in the same sample. 20 Survey questions were then refined and finalised. Survey domains included demographics of AAI services, detail of service delivery and supporting oversight documentation.
Survey dissemination
An invitation email containing the link to the online survey and accompanying Participant Information Sheet was circulated via (1) the Intensive Care Society membership, (2) national and regional critical care networks and (3) social media, to achieve a snowballing approach to dissemination. The survey was open for a period of 8 weeks (February–April 2024), with repeated circulation and targeted approaches to maximise response during the interim timeframe.
Review of local service oversight documents
Survey respondents who indicated that they delivered AAI services in their ICU were additionally asked what local oversight documents were in place (e.g. a policy, protocol, guideline, or other similar document) to support service delivery, and to send a copy of these documents to the research team. A reminder email was sent if no response was received after 2 weeks.
Data analysis
Survey data were downloaded from the survey platform into Microsoft Excel (Microsoft Corp, Redmond, WA, USA). Multiple responses for any individual hospital site were de-duplicated and amalgamated into single response sets. Where discrepancies were identified between response sets, the most complete and/or first-received response set was used as the final response option. 20 Respondents providing contact details were contacted to confirm or clarify any queries with regards responses. Descriptive statistics were used to analyse quantitative responses including normality testing, mean (SD) or median (IQR) scores, frequencies, proportions. Summative content analysis was used to analyse any free text comments. 21 Analyses were performed using Microsoft Excel.
Oversight documents were analysed by two researchers (SW, cross-checked by BC) using a framework analysis approach broadly adopting the following stages22 –24:
(i) Familiarisation: This involved organising the number and type of documents received from sites according to categories defined by survey question response options. This served as a foundational step in gaining content familiarity.
(ii) Developing a framework: Themes and topics, based on key aspects of content reported in documents and generated through familiarisation, were used to generate initial frameworks
(iii) Coding/indexing: Systematic application of codes from the agreed analytical framework to the whole dataset.
(iv) Charting the data: entering summarised data into the framework matrix.
(v) Mapping and interpretation with any coding refinements: Interpretation of findings, mapping similarities and differences across the data, exploration of patterns or explanatory themes.
Ethical considerations
The study was approved by Queen’s University Belfast Medicine, Health, and Life Sciences REC (MHLS 23_155). Participation in the service evaluation was voluntary and participants could withdraw at any time up until the point of submitting their responses. A Participant Information Sheet was available, and the opening introduction page of the survey also included all relevant information regarding participation. Participants were asked to confirm reading of several consent statements, and survey completion was considered indicative of informed consent. Surveys were completed anonymously, unless indicating availability of an AAI service and agreement to provide any local oversight document; in which case, these participants were asked to provide email address for the purposes of follow-up contact. Further provision of contact details was voluntary. All service evaluation data, including participant email addresses, were held in secure, password-protected institutional servers, only accessible by members of the research team from that institution (Queen’s University Belfast).
Results
Survey response rate and availability of AAI services
In total, 88 site responses were received (/242, 36.4%), of which 14 were identified as duplicates and removed from the dataset resulting in a total of 74 responses included in analysis (/242, 30.6%). Across the UK, the breakdown of survey response was as follows: England (n = 59/195, 30.3%), Scotland (n = 7/23, 30.4%), Northern Ireland (n = 5/9, 55.6%), and Wales (n = 3/15, 20%). Thirty-two sites (/74, 43.2%) reported that they currently have AAI services available for critically ill patients, including 31 based in England and 1 based in Wales. Most services commenced in the last 5 years (n = 19, 2019 onwards), 5 were uncertain with regards start date, and the remainder (n = 8) commenced > 5 years ago. Of the sites with services available, these were AAA services alone for nearly all (30/32, 93.8%), and with two sites (6.3%) reporting both AAA and AAT services available. No site had AAT services alone.
Animal-assisted activity services
Just over half of sites with AAA services (18/32, 56.3%) reported having a designated coordinator/champion who identified patients and arranged visits. Similarly, most sites (19/32, 59.4%) also reported that services were available to all patients, but infection management and/or immunocompromise was the main reason for patient exclusion. All services involved dogs, with the most common breeds including golden retriever, cockapoo and labrador; no other animals were reported. Sessions typically lasted 30–60 min (14/32, 43.8%), on a weekly basis (11/32, 32.4%), with 1 handler present (29/32, 90.6%). Handlers were external/independent volunteers from registered animal organisations in most services (23/32, 71.9%). All sites reported that AAA sessions involved patients talking to/engaging with the animal, and thereafter the most common activity was participation in animal cares (13/32, 40.6%). Most sites (27/32, 84.4%) reported they did not collect any feedback from either patients or staff on their enjoyment and/or potential benefit from AAA session. No site reported any episode of patient harm during an animal visit; one site reported an episode of animal harm (consumption of prohibited food item). Further detail of characteristics of AAA services is reported in Table 1. Free text responses provided by sites with AAA services are outlined in Supplemental File 2 (Table E1).
Characteristics of animal-assisted activity services.
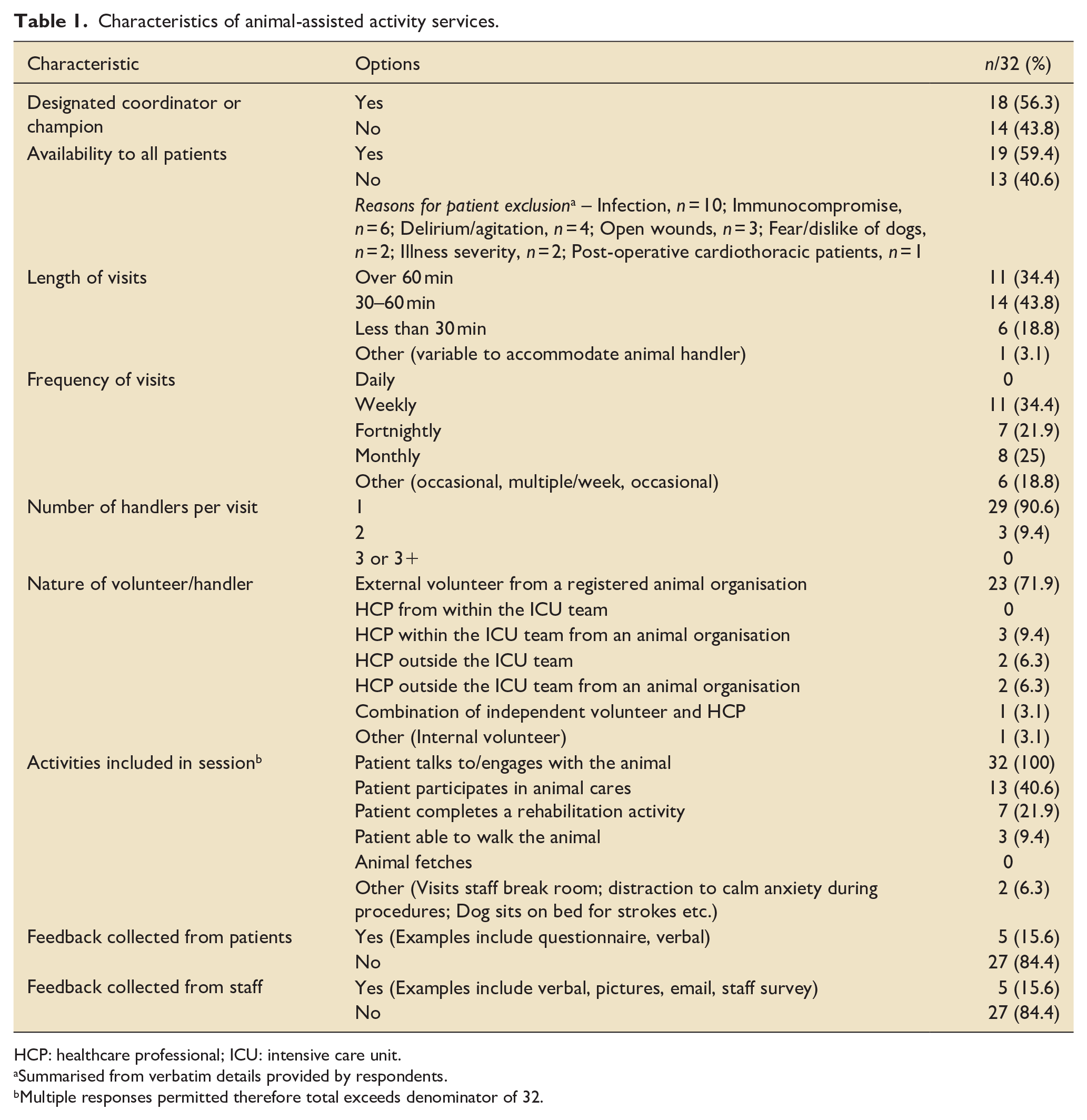
HCP: healthcare professional; ICU: intensive care unit.
Summarised from verbatim details provided by respondents.
Multiple responses permitted therefore total exceeds denominator of 32.
Animal-assisted therapy services
Of the 2 sites that offered AAT services, 1 was based in England and the other was based in Wales. Both sites reported that AAT services were limited to critically ill patients without infection risk, allergies to dogs (the specific animal used by each) or located in particular clinical areas for example, long-term ventilation/complex care ICU. Therapy dog/handler pairs were external volunteers from a registered animal organisation. Patients were selected for therapy sessions for a variety of reasons – family/care partner request, referral by ICU staff member (including physiotherapy and psychology), or directly by the handler (where at one site, the handler was a staff member). Whilst each site varied in terms of typical length of therapy session (<30 min and 30–60 min), both sites reported that the number of sessions available to individual patients was at individual clinician discretion according to patient need. Healthcare professionals delivering therapy sessions were reported as nurses, physiotherapists and pharmacists. Both sites selected ‘all of the above’ in response to a multiple-choice question about the reasons patients received AAT; these reasons were low mood, anxiety, depression, pain and the need to improve interaction or engagement with different aspects of care (e.g. nursing, medical, rehabilitation). Subjective patient feedback was the only measure reported by either site for monitoring progress and/or evaluating outcomes. Neither site reported that they collected any feedback from patients or staff on the potential benefit of therapy sessions. No patients had ever been harmed during an AAT session; one site reported an episode of animal harm (consumption of prohibited food item).
Oversight of AAI services
At the 32 sites with available AAI services, oversight approach was reported as follows: Self-drafted hospital/Trust policy/guidance/SOP (or equivalent document), 17 (53.1%); Adoption of independent professional organisation policy/guidance/SOP with local modifications, 8 (25.0%); and Adoption of independent professional organisation policy/guidance/SOP (or equivalent document), 2 (6.3%). The remaining 5 (15.6%) sites reported none of these options applied to them; two provided qualitative responses indicating delivery of services via local charity organisations (where those organisational policies would apply). As part of service oversight, most sites (26/32, 81.3%) reported the same documents reflected local Infection Prevention and Control measures to support service delivery. Twenty-seven individual oversight documents were provided for analysis from 16 sites. Table 2 summarises details of these documents; 20 were governance-related – Trust standard operating procedures (n = 8), policies (n = 7), or guidelines (n = 1), or professional organisation documents (n = 4); the remaining 7 documents related to logistical aspects of AAI service delivery for example, information leaflets, animal registration forms. Subsequent analysis focused on the 20 governance-related oversight documents. A framework was developed based around two core themes of oversight of AAI services that emerged through familiarisation with the documents: ‘Critical care staff responsibilities’ and ‘Animal handler responsibilities’. In many cases, these two themes reflected the original structure and
Summary of oversight documents provided for analysis.
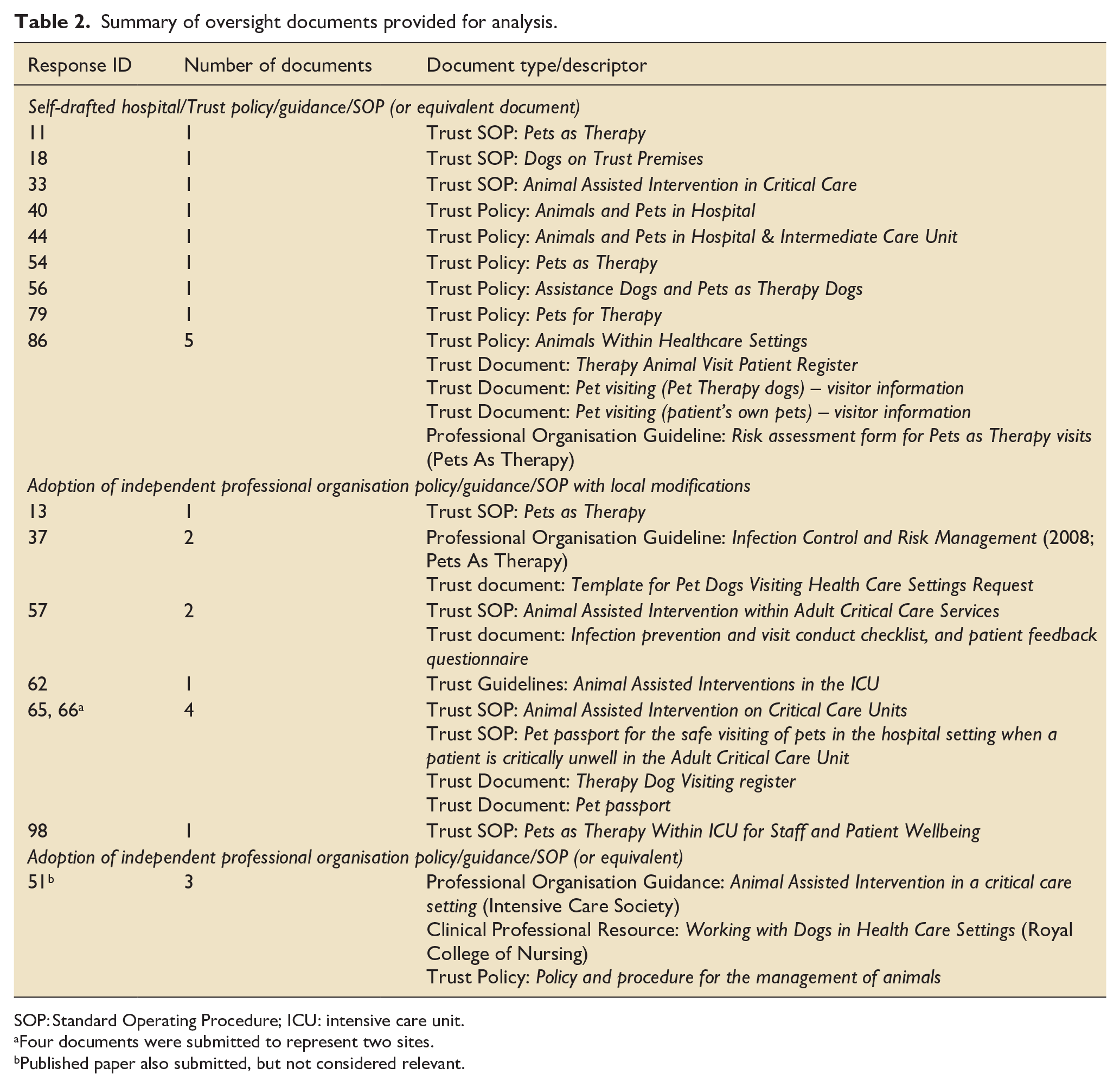
SOP: Standard Operating Procedure; ICU: intensive care unit.
Four documents were submitted to represent two sites.
Published paper also submitted, but not considered relevant.
organisation responsibilities’. In many cases, these two themes reflected the original structure and organisation of documents for example, Intensive Care Society Guidance for Animal Assisted Intervention in a Critical Care Setting; even where this structure was not used, content reported within documents naturally aligned to them. Each core theme had several sub-themes related to it reflecting different aspects of oversight for example, documentation and security. Some sub-themes were common across the two core themes for example, welfare and infection control. However, data charting highlighted that distinct information was evident relating to how these sub-themes reflected each of the core themes such that maintaining replication was necessary for example, critical care staff were identified to be responsible for handler and patient welfare, whereas animal welfare was the remit of the animal handler.
A full description of the two core themes and their sub-themes, with accompanying exemplar text taken from source documents, is provided in Table 3. Codes used to develop core and sub-themes are reported in Supplemental File 2 (Table E2). Figure 1 presents an overview summary depicting the relationship between core and sub-themes. There were no discernible differences observed when analysing oversight documents depending on category that is, whether the document was self-drafted, locally modified from an independent professional organisation, or wholly adopted from an independent professional organisation.
Core themes, sub-themes, description and exemplar text from documents related to oversight of animal-assisted intervention services.
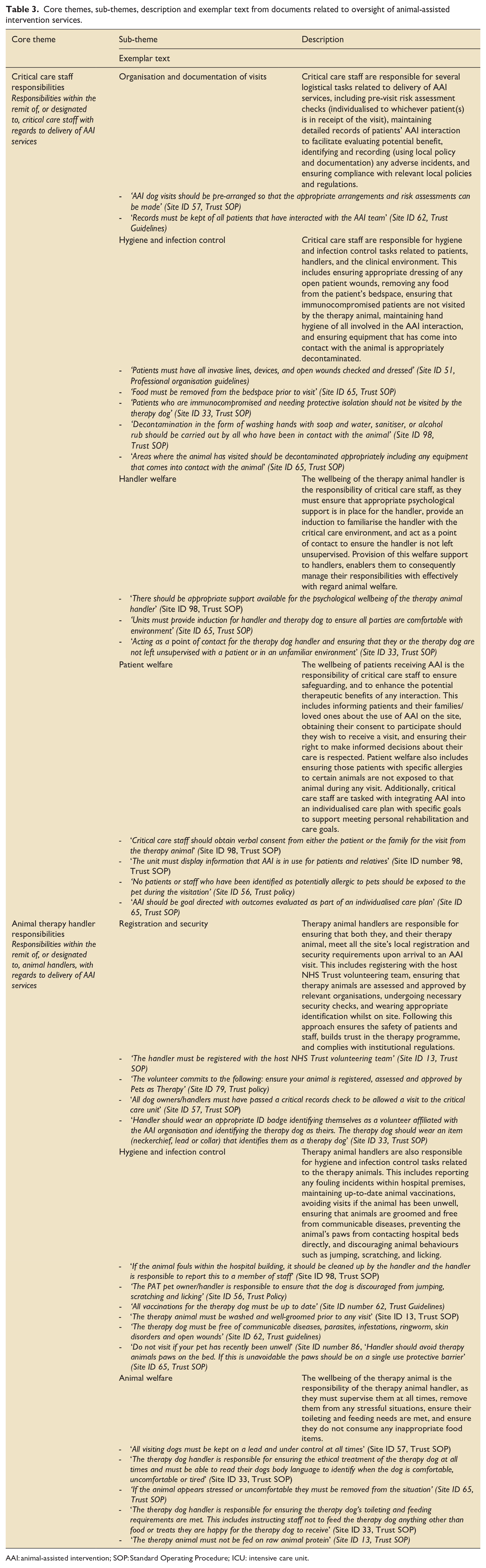
AAI: animal-assisted intervention; SOP: Standard Operating Procedure; ICU: intensive care unit.
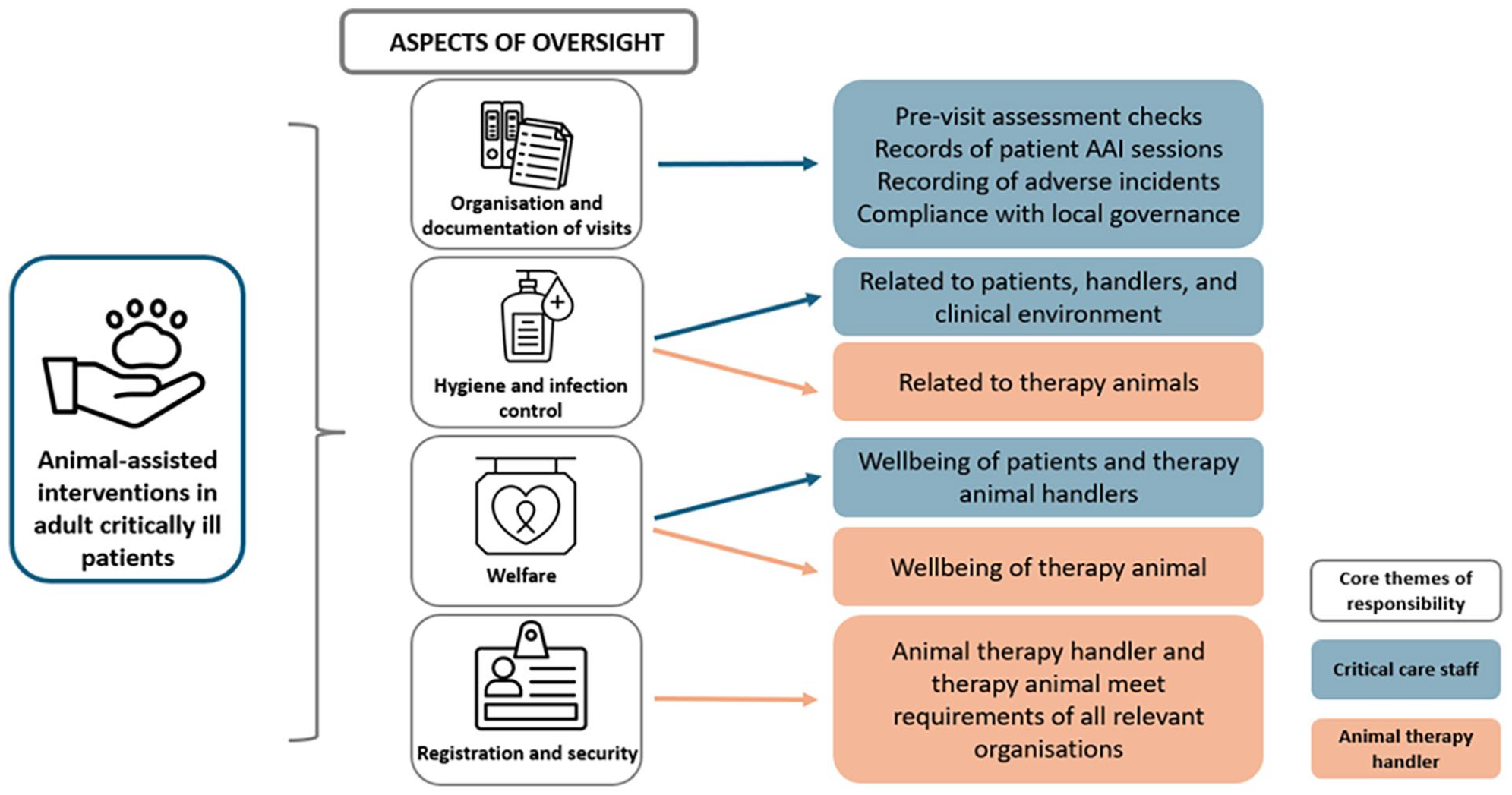
Summary of oversight related to animal-assisted interventions in adult critical care units. Overview summary depicting aspects of oversight related to delivery of animal-assisted interventions in adult critical care units. Aspects of oversight (sub-themes) were the responsibility of both critical care staff (orange) and animal therapy handlers (blue; core themes). Some aspects overlapped but with distinct content detail.
Sites with no available AAI services
Forty-two sites (/74, 56.8%) had no current AAI services available. Barriers to sites commencing services, and reasons for sites stopping services where they had been previously available, are reported in Table 4. Concern regarding Infection Prevention and Control was the most prevalent factor in each case (26/34, 76.5%, and 4/8, 50.0% respectively). Lack of funding and personnel understaffing were other frequently reported barriers to initiating services. Patient/family declining services was not reported as a concern by any site. Of 34 sites that had never had service previously available, the majority had no plans to commence these in the future (22/34, 64.7%); the same was also true for those sites that had previously had services (5/8, 62.5% indicated no plan to recommence). Free text responses provided by sites with AAA services are outlined in Supplemental File 2 (Table E3).
Limitations to animal-assisted intervention service provision.

AAI: animal-assisted intervention; ICU: intensive care unit.
Respondents could select more than one applicable reason hence totals exceed denominators.
Indicates reasons provided as ‘Other’.
Discussion
This study involved a national UK service evaluation to ascertain availability, characteristics and oversight of AAI services in adult ICUs. Data from two sources, quantitative survey and qualitative document analysis, were assimilated to characterise current service delivery. Our data demonstrate that AAI services were available in nearly half of responding sites. Reflecting the recency of animal therapy into the clinical setting of UK critical care, most services had commenced in the last 5 years. Oversight documents revealed two core themes of information pertaining to responsibilities of critical care staff and animal therapy handlers. Importantly, all AAI services were reported as provided on a volunteer basis by bedside clinicians, animal handlers, and others who see potential benefit to patients, families, and staff that has yet to be academically quantified but feels meaningful. This is consistent with documented efforts to evolve critical care by ‘humanising’ the ICU environment. The intention of such humanisation efforts are to focus not only on survival and medical treatment, but to also create a culture flourishing for patients, families and staff.25 –27 The potential for progression from small and unfunded pilot programming (as evidenced by existing AAI service provision) to larger-scale research efforts is consistent with similar initiatives to humanise critical care including end-of-life support programmes,28,29 patient navigation programmes 30 and music programmes.31,32
Interpretation of findings
Our data demonstrated that most UK ICUs with AAI services available for adult patients reported these to be animal-assisted activity services, focusing on interactive-based engagement. Animal-assisted therapy services, providing more personalised treatment interventions, were relatively rare. This is consistent with the observation that all services are conducted on a volunteer basis, leaving limited flexibility and availability for more skilled and nuanced interventions of potential therapeutic effect. Additional resources (time and funding) could resolve this, as seen in a recent study in the paediatric critical care population investigating the feasibility of animal-assisted therapy comprising an occupational therapist, psychologist and a therapy dog. 14 Evaluations of therapy sessions (on average approximately 40 min duration) across 61 patients revealed significant reductions in pain, fear and anxiety levels following the intervention against a background of clinical stability, with no adverse effects reported, and subjective positive feedback from all involved. Further evaluation would be valuable for determining how these benefits may then translate into other clinical aspects.
Understaffing of personnel also contributes to operational limitations in AAI service delivery, reported as a barrier by a third of respondents. Furthermore, only around half of respondents reported presence of a designated coordinator or champion. These roles can be particularly important for implementing new innovations with patients albeit their full potential remains under-explored. 33 That said, for overseeing administrative and other coordination aspects of AAI service delivery, the practical advantages to such a role are clear. We did not explore how these roles are currently funded (if available), but speculate they are supernumerary and goodwill, and therefore at risk of limited sustainability with staffing turnover or other workload pressures. In the future, if provision of AAI services becomes established, then resourcing will need to consider administrative support.
Despite concern regarding infection risk being the most prevalent barrier to either commencing new, or having ceased previously available, AAI services, respondents from currently active sites reported no episodes of patient harm including acquired infection. Nonetheless this remains an important factor that warrants continued monitoring in future clinical and research contexts. Similarly, engagement from patients, family, and care partners was evident in responses, and no site reported any negative experiences from AAI delivery. However, as a self-selected, relatively small sample of responses, this would merit further exploration. Understanding the potential for unintended consequences associated with AAI is essential, and we did not capture this in our survey; for example, the experience of patients, visitors or staff who have a fear of, or allergy to, animals – even if they are not directly involved in the interaction, the presence of animals in the environment may be significantly detrimental. Similarly for example, for patients experiencing delirium, confusion, or disorientation, observing the presence of animals may further exacerbate their clinical state. Empirically clinicians should be mindful of any necessary environmental adaptations that may support these scenarios for example, separate physical locations for AAI interactions to occur, as well as careful balance of the potential benefits and harms that could occur. Notably, all AAI services in our data reported use of dogs as the therapy animal, but in other contexts, other animals have been reported of benefit and this could be expanded to explore in future work with critically ill patients.34 –36
Many reported AAI services had commenced within the last 5 years. Whilst causal association is not possible to determine, this timeframe aligns with publication of the UK Intensive Care Society Guidance for delivering AAI in critical care settings, 15 and it is possible that publication of this guidance from the national specialist professional organisation may have prompted service emergence. This guidance document, one which many sites reported as either their primary or locally modified source of service oversight, offers practical instruction on the logistical considerations for offering AAI along with a narrative description of some of the related evidence. However, it is important to highlight that there is currently a lack of definitive randomised controlled trial data to confirm effectiveness of AAI,6,13,14,37 and this was cited as the reason for lack of service availability by a fifth of respondents in the current study. As the critical care specialty embraces humanising the ICU environment, culture and experience for the benefit of patients, caregivers, and staff,25 –27 ensuring a rigorous foundation of evidence to underpin interventions such as AAI will be important for justifying the resources needed for equitable access and delivery of services. A small number of respondents reported ‘lack of priority’ as a barrier to service availability, which reflects this point, and a possible lack of willingness to offer AAI service that may divert capacity away from core services in the absence of demonstrable benefit at present.
Our analysis of oversight documents revealed both individual and shared themes of responsibility for the effective and appropriate delivery of AAI services between critical care staff and animal therapy handlers. Following governance preserves the safety and wellbeing of all participants involved in AAI opportunities and the clinical environment. However, the considerable overlap in content of oversight documents from sites suggests scope for avoiding redundancy and duplication of efforts if nationally generated guidance documents could more easily be approved locally. This would also reflect a move to efficiency within service delivery, which would be invaluable if service upscaling were to occur across the UK at any point.
Critique of the method
This service evaluation benefits from several strengths. Our survey component follows methods successfully used to previously survey the same population of UK ICUs. 20 The sampling frame was established from two national registries, and we undertook various steps to ensure rigour of the survey design including internal and external pilot testing, refinement of questions and optimisation of survey platform functionality to facilitate user-experience of completion. 38 Missing data were minimal, and contact was made with authors where survey responses were incomplete or required clarification to ensure data accuracy. We disseminated the survey widely via multiple methods including professional organisations and social media and followed-up with repeat reminders during the active timeframe to maximise the response rate. We encouraged responses irrespective of AAI service availability at ICUs, knowing this would be valuable from a national service evaluation perspective. 16
However, despite these approaches our survey response rate after de-duplication was approximately 30%. Typically, a survey response rate of ⩾70% is considered representative19,39 and hence our findings should be interpreted with caution with regards reflection across all ICUs in the wider sample frame. Absence of data on survey non-responders limits comparison to responders and the potential for response bias,39,40 as well as ascertaining reasons for non-response. Common factors such as time and motivation may be causal, but it could be speculated that given the novelty of AAI services in UK ICUs, a large proportion of non-respondents do not currently have services available and therefore perceived the survey as irrelevant. Furthermore, in addition to surveying ICUs, our service evaluation additionally included a detailed analysis of independent oversight documents.41,42 This provided contextual information, albeit was also limited to documents provided from half of respondents. Nonetheless, this approach of methodological triangulation, incorporating mixed quantitative and qualitative data collection from two sources, added depth of understanding, meaning, and knowledge to strengthen interpretation and validity of our data and address our study aims. 43
For practical reasons, we encouraged a single response from each institution from any healthcare professional who was sufficiently knowledgeable regarding availability of AAI services to contribute to the service evaluation. In this way, we assumed a consistent approach to AAI service availability irrespective of whether a site had multiple ICUs, and we did not capture potentially important variations in the number, size, or specialty of ICUs at any individual site. Overall, this assumption was maintained, albeit we had one example of variability in service provision across different ICUs based on responses from one site. We also limited our data collection to adult ICUs, albeit empirically we are aware of AAI services being delivered in some UK paediatric critical care settings. Future research may consider inclusion of granular service details to reflect bespoke inter-ICU differences. Additionally, we did not gather certain important details on the services delivered by each of the sites. For instance, the online survey lacked items related to the contributions of volunteer dog handlers and healthcare personnel in AAT. Future research should therefore characterise AAI services in greater depth, as this would help identify differences in service delivery across sites and enhance interpretation of findings from different interventions. Nonetheless, we are confident our data are valuable for characterising services where these are delivered, at this relatively early stage of investigation into animal therapy in critical illness in the UK.
Conclusion
In a rigorously conducted national service evaluation, a small sample of responses revealed AAI services to be available in less than half of ICUs, with shared responsibility by critical care staff and animal therapy handlers. There were no documented harms to patients or staff, and only one minor harmful incident reported for a therapy animal. Empirical enthusiasm for, and value of, interventions is countered by current lack of definitive evidence of effectiveness, which should be addressed before wider implementation of AAI services and the associated resource requirements, is undertaken.
Supplemental Material
sj-docx-1-inc-10.1177_17511437241301000 – Supplemental material for Animal-assisted intervention services across UK intensive care units: A national service evaluation
Supplemental material, sj-docx-1-inc-10.1177_17511437241301000 for Animal-assisted intervention services across UK intensive care units: A national service evaluation by Sam Wright, Holly McAree, Megan Hosey, Kate Tantam and Bronwen Connolly in Journal of the Intensive Care Society
Supplemental Material
sj-docx-2-inc-10.1177_17511437241301000 – Supplemental material for Animal-assisted intervention services across UK intensive care units: A national service evaluation
Supplemental material, sj-docx-2-inc-10.1177_17511437241301000 for Animal-assisted intervention services across UK intensive care units: A national service evaluation by Sam Wright, Holly McAree, Megan Hosey, Kate Tantam and Bronwen Connolly in Journal of the Intensive Care Society
Footnotes
Acknowledgements
The authors would like to thank the following colleagues for their time providing external piloting and feedback of the survey during development: Aoife Abbey, Paul Dean, Rebekah Haylett, Reena Mehta, Stephen Webb and Clare Windsor (all via the UK Intensive Care Society), and Lindsay Leary (University Hospitals Plymouth NHS Trust).
Credit statement
Sam Wright: Data curation, formal analysis, investigation, methodology, project administration, supervision, writing – original draft, writing – review and editing.
Holly Mcaree: Data curation, formal analysis, investigation, methodology, writing – original draft.
Megan Hosey: Investigation, writing – review and editing.
Kate Tantam: Investigation, writing – review and editing.
Bronwen Connolly: Conceptualisation, data curation, formal analysis, investigation, methodology, project administration, supervision, writing – original draft, writing – review and editing.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Bronwen Connolly is a Director of Research, Intensive Care Society. Kate Tantam is Deputy Chair, National Rehabilitation Collaborative, Intensive Care Society and co-author, Intensive Care Society Guidance for Animal-Assisted Intervention in a Critical Care Setting. This study was conducted independently of these roles.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.