
Abstract
Background:
Occupational Therapy (OT) in the Intensive Care Unit (ICU) supports recovery in physical, cognitive, emotional domains, and activities of daily living (ADL), yet. Provision across the UK remains inconsistent, with variable staffing and role integration and no data illustrating the potential impact from such roles.
Method:
A retrospective service evaluation was undertaken in a UK NHS adult ICU to examine the association of increased OT staffing with changes in rehabilitation activity and functional status. Patients with ICU stays over 7 days were included in line with NICE CG83 high rehabilitation risk criteria. Three 1-month timepoints were compared. Data included delivery of OT interventions, functional outcomes (Modified Barthel Index), and discharge destination.
Results:
Ninety-nine patients were included. Increased OT staffing was associated with a greater proportion of patients receiving OT assessments, upper limb rehabilitation, personal activities of daily living retraining, cognitive screening, delirium management, and therapy handover. Modified Barthel index scores at hospital discharge increased across timepoints 1, 2 and 3 (55, 71.5 and 82, respectively (p = 0.02)). Discharge destination patterns varied and could not be attributed solely to staffing changes.
Discussion:
Increased OT staffing was associated with greater delivery of rehabilitation interventions and potential improvements in functional outcomes. However, differences in patient clinical complexity across timepoints may also have influenced these results. Further evaluation is required to establish causal relationships.
Keywords
Introduction
Occupational therapists (OT’s) are recognised as core members of the intensive care unit (ICU) multi- disciplinary team.1–5 Their role includes assessment and rehabilitation of physical function cognition, mood, and engagement in daily activities alongside delirium management and early discharge planning,1,3,4,6–9 maintaining joint range, conducting seating assessments, addressing sensory needs, providing mental health support, and assessing and managing cognitive function and delirium.5,10–12 However, provision remains variable, and many ICUs have limited dedicated OT staffing.10,13 Under-resourcing, role misunderstanding, and workforce constraints contribute to inconsistent delivery and service variation.2,13
This underutilisation of OT may prevent patients from receiving the comprehensive, multidisciplinary care that is crucial for their recovery.3,4,13 It is therefore essential to continue demonstrating the impact of the ICU OT role on achieving important patient outcomes as described in relevant guidelines. This will in turn support future growth of the OT workforce in the ICU setting.
Aim
To examine the association between OT staffing levels, delivery of rehabilitation interventions, and patient functional outcomes.
Method
Study design
A retrospective service evaluation was undertaken in a 32-bed adult ICU in a UK NHS hospital. The general ICU comprises of respiratory, cardiac and surgical adult (>16 years) admissions who require intensive care medicine. The unit receive a 6-day rehabilitation therapy service.
Inclusion criteria
Patients aged ⩾16 years with an ICU length of stay ⩾7 days, who are at risk of physical and non-physical risk factors for likelihood of ongoing mortality, were included in line with NICE CG83 high-risk rehabilitation guidance which identifies prolonged ICU stay as a marker of rehabilitation risk.2,14,15 Patients who died during ICU admission were excluded.
Data collection and analysis
Data collection occurred at three time points which corresponded with staffing expansion reflecting a staged recruitment (Table 1). Each data collection period was 1 month in duration.
Timepoints of data collection with corresponding occupational therapy staffing levels and bed: staff ratios.
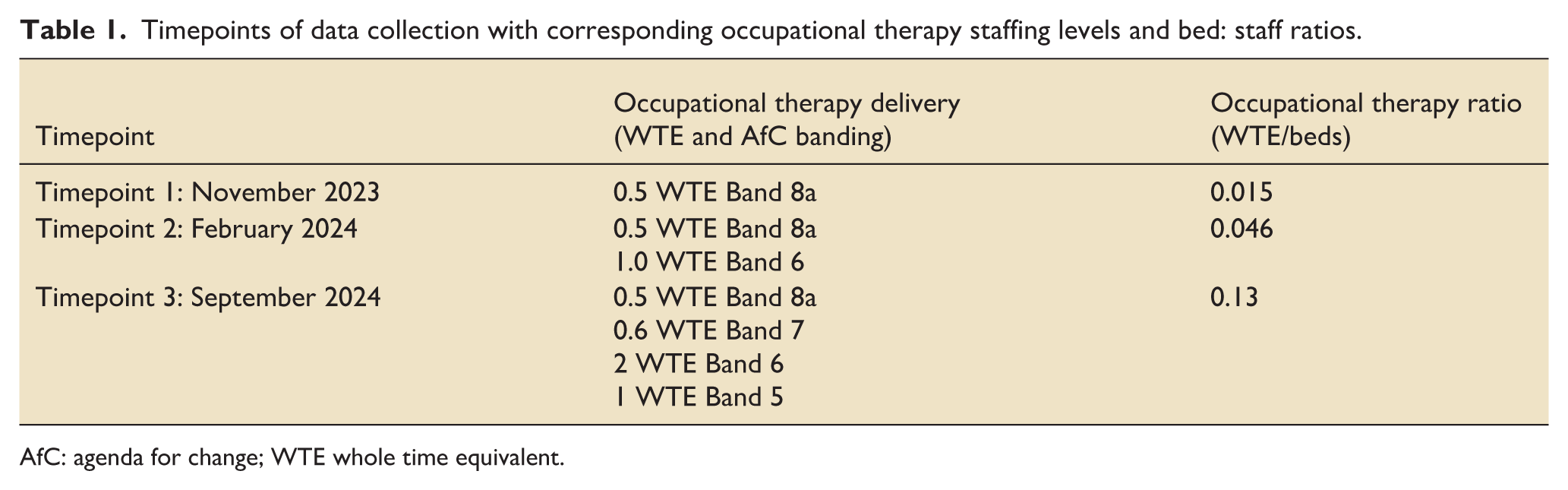
AfC: agenda for change; WTE whole time equivalent.
Data collection and analysis
Demographic and clinical data (age, diagnosis, frailty, APACHE II) were extracted from ICNANRC -linked MedICUS records. Rehabilitation activity was identified through documented OT interventions within electronic clinical notes (ICCA and CareFlow EPR). NICE CG83 rehabilitation risk stratification 14 was recorded within ICCA and confirmed through clinician documentation (physical or non-physical risk factors for likelihood of ongoing morbidity).
Patient outcome data was collected retrospectively using the ICU electronic notes platform (ICCA) and hospital database (Careflow EPR). Data included intubation and if tracheostomy requirement, evidence of delirium, length of ICU stay, overall hospital stay, and discharge destination at the point of acute hospital discharge. All data was collated into a Microsoft Excel 2018 database (Microsoft Corp, Remond, Washinton). This was password protected and maintained on a Microsoft SQL server database system within the Trust. Data was manually checked by a member of the study team (JB) for accuracy which was further checked by a second member (JS). The database was only accessible to the relevant members of the study team.
The Guideline for Provision of ICU Services V2.1 (GPICS) provides national guidance for all professions working within an ICU. 2 The OT and rehabilitation chapters set quality standards to guide OT practice throughout the UK. These recommendations were used to benchmark set interventions delivered, our service interpretation included:
All patients screened as delirium positive receive an assessment and are provided a non-pharmacological treatment plan
Patients are provided with individualised rehabilitation programmes including physical and non-physical elements (including upper limb rehabilitation, personal care, cognition, and mood)
To screen the patient’s preadmission and current functional abilities to set realistic goals
Screen high rehabilitation needs patients for their follow up requirements and provide a therapeutic handover to the ward
Statistical analysis was performed using the Statistical Package for the Social Sciences, version 30.0 (SPSS Inc., Chicago, IL, USA). Descriptive analyses of the continuous variables are presented as the mean ± standard deviation (SD), median (interquartile range (IQR)), or frequency, as appropriate according to the distribution of the data. Continuous variables were analysed using ANOVA or Kruskal–Wallis tests; categorical variables using Chi-square analysis. p < 0.05 was considered statistically significant.
Results
Data collection took place between November 2023 to September 2024. There were no statistically significant differences in age, sex, or primary admission pathway across timepoints; however, differences in markers of clinical complexity were observed.
Specifically, the prevalence of tracheostomy, Rockwood Frailty Score, and APACHE II scores were lower in Timepoint 3 compared with Timepoints 1 and 2 (Table 2).
General characteristics of the patients.
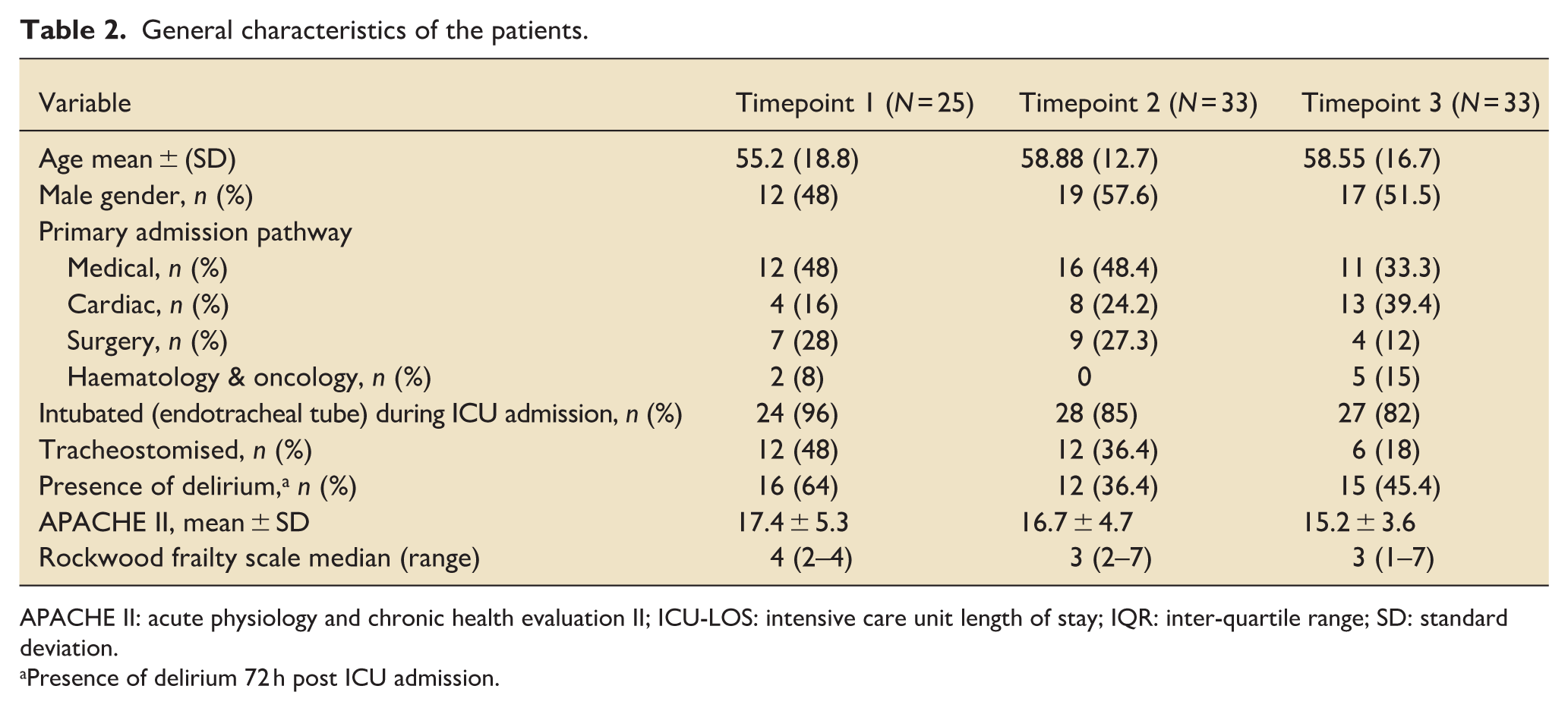
APACHE II: acute physiology and chronic health evaluation II; ICU-LOS: intensive care unit length of stay; IQR: inter-quartile range; SD: standard deviation.
Presence of delirium 72 h post ICU admission.
These differences suggest possible variation in patient acuity and functional reserve across cohorts.
Delivery of occupational therapy interventions
The proportion of patients receiving guideline-aligned OT interventions increased across timepoints (Figure 1). This included: functional history screening, OT assessment completion, non-pharmacological delirium management, personal activities of daily living (PADL) retraining, therapy handover to ward-based teams (p = <0.001), and cognitive screening (p = 0.049). There was no significant difference between the timepoints regarding objective mood screening (p = 0.26), goal setting in the unit (p = 0.22) and goal setting in the stepdown ward (p = 0.07; Figure 1). Timepoint 3 demonstrated the greatest breadth and frequency of intervention delivery, coinciding with the highest staffing level (4.1 WTE).
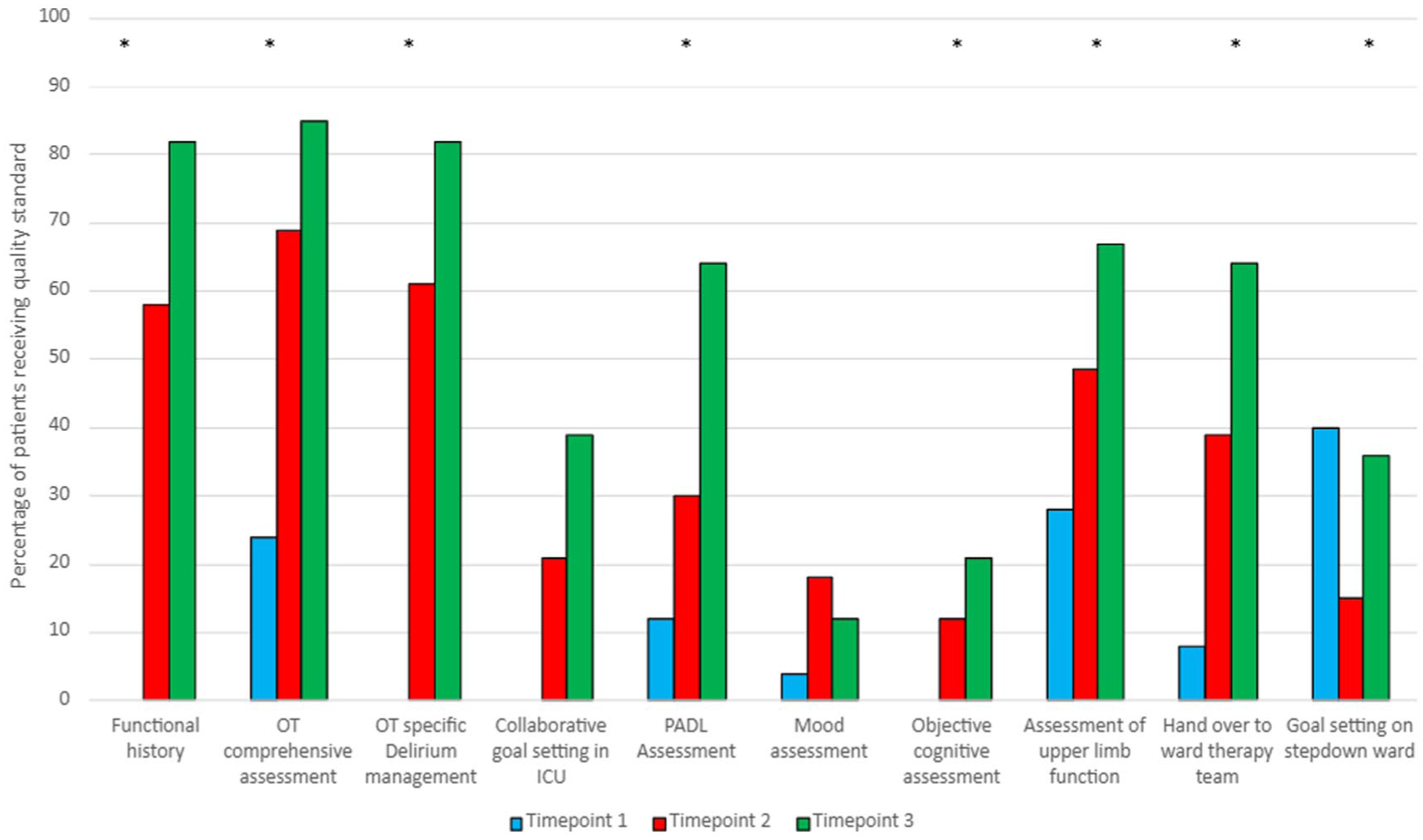
Delivery of ICU quality standards by an occupational therapist.
Patient outcomes
There was no significant difference in ICU mobility scale score across timepoints but there was a step wise increase by one score in each time point (Table 3). Modified Barthel Index (MBI) scores at hospital discharge (Table 3) increased across the three timepoints from 55 to 71.5 to 82 respectively (p = 0.02). This suggests potential improvement in functional independence; however, interpretation must consider differences in patient clinical complexity.
Patient outcomes at the three timepoints of data collection.
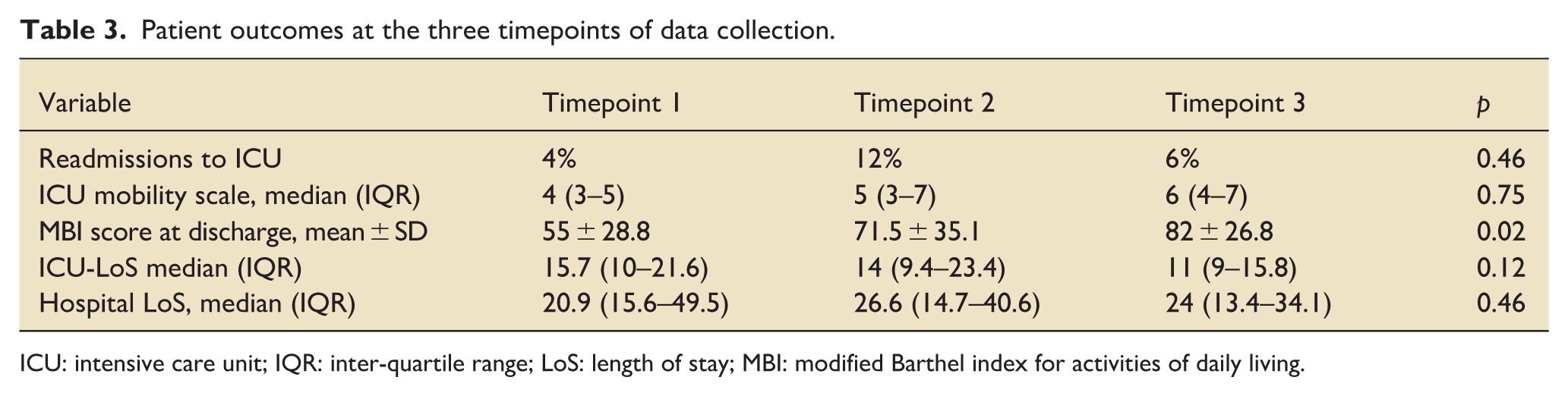
ICU: intensive care unit; IQR: inter-quartile range; LoS: length of stay; MBI: modified Barthel index for activities of daily living.
ICU readmission and length of stay
There were no significant differences in ICU readmission or length of stay across timepoints (Table 3). This indicates that staffing changes did not adversely affect throughput or discharge timing.
Discharge destinations
Hospital discharge destination distributions varied across timepoints (Figure 2).
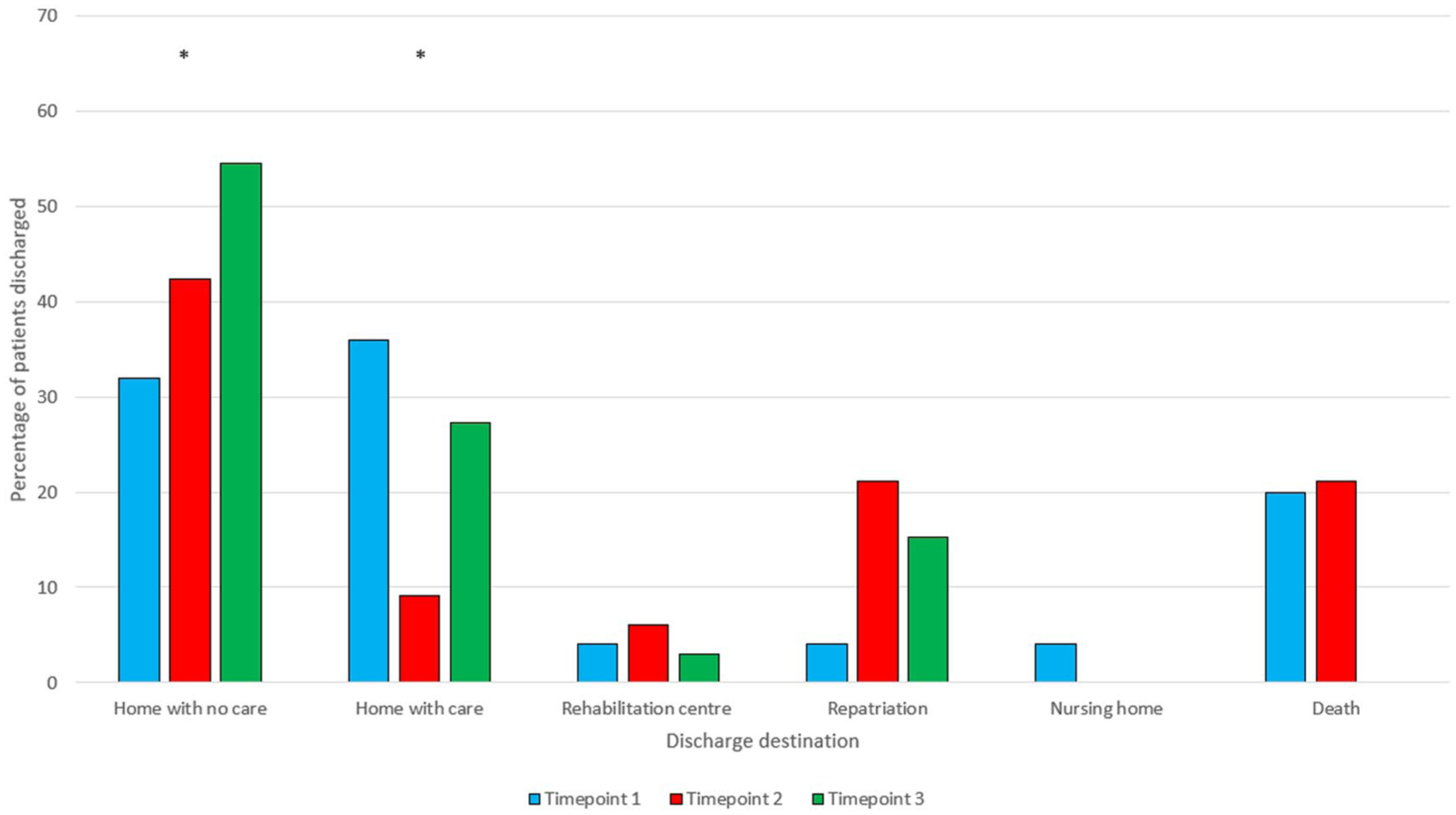
Patient discharge destination from ICU.
Although the proportion of patients discharged home was highest in Timepoint 3, the decrease in tracheostomy prevalence and frailty in this cohort indicates that clinical characteristics may have contributed to this pattern. Therefore, no causal inference can be made between OT staffing and discharge destination.
Discussion
To the authors knowledge, this service evaluation is the first to analyse OT activity in the critical care setting against national quality standards. Findings therefore provide a foundation for future work exploring optimal staffing models and the role of occupational therapy in critical care rehabilitation pathways. This evaluation demonstrates that increased OT staffing was associated with greater delivery of holistic and guideline-aligned rehabilitation interventions in the ICU.
Within the UK healthcare context, a growing proportion of patients are surviving critical illness and transitioning to community care.13,16–18 While survival rates have improved, many continue to experience persistent physical, cognitive, and psychological impairments, collectively referred to as post-intensive care syndrome.19–21 Addressing these complex needs requires coordinated multidisciplinary team (MDT) rehabilitation, to include OT, across the entire recovery pathway.1,3,5,6,12
The impact of increased OT staffing aligns with national recommendations promoting early, occupation-focussed rehabilitation as part of routine critical care therapy provision.2,13–16 The increased OT provision enabled more comprehensive functional and cognitive assessment; greater frequency of upper limb rehabilitation and PADL retraining; increased non-pharmacological delirium management and improved therapy handover to ward teams, thus supporting continuity of care. These are positive changes in light of the recent NCEPOD report: Rehabilitation Following Critical Illness. This report highlighted significant shortfalls in the critical illness patient pathway, including poor coordination of rehabilitation between ICU, ward-based care, and community care; limited policies and audits; and a lack of key workers to coordinate rehabilitation. 16 In Timepoint 1, intervention delivery was constrained due to limited staffing (0.5 WTE).
While MBI scores improved across timepoints (Table 3), these changes cannot be attributed solely to ICU OT staffing due to observed differences in patient frailty and clinical complexity (Table 2). This is particularly relevant at Timepoint 3, where lower frailty and fewer tracheostomies (Table 2) likely facilitated improved discharge outcomes and self-care independence. These findings therefore indicate an association, rather than demonstrating causation. Nonetheless, the results underscore the clinical value of sustained OT presence, particularly in relation to delivering occupation-focussed assessment and rehabilitation that may otherwise be deprioritised in ICUs with constrained therapy staffing. Previous research has demonstrated that less than half of UK ICUs (48.1%) have input from OT, 11 findings such as those presented here are therefore important to further justify the role of an OT within the critical care setting.
Early functional assessment and delirium management are increasingly recognised as key components of post-ICU recovery pathways. 22 Our findings illustrate that with an expanding OT provision there may be more consistent delivery of these delirium specific interventions.
Limitations
This service evaluation has several limitations. The evaluation demonstrated an increase in the quantity of documented interventions; however, intervention quality was not measured, and therefore no conclusions regarding quality can be drawn.
Data were obtained retrospectively from clinical documentation, and therefore the accuracy of recorded interventions is dependent on documentation completeness. This may have resulted in either underestimation or overestimation of intervention delivery. Additionally, differences in patient clinical complexity across timepoints (including lower frailty scores and reduced tracheostomy prevalence in Timepoint 3) may have influenced functional recovery and discharge outcomes, independent of therapy provision.
As a single-centre evaluation without a comparator group, findings may not be fully generalisable to other settings with different staffing models or patient profiles.
Future research should include prospective multi-centre designs, consistent functional outcome measurement points and analysis of patient- and family-reported outcomes.
Conclusion
This evaluation found that increased OT staffing was associated with greater delivery of holistic rehabilitation interventions in ICU and may be linked to improvements in functional outcomes at hospital discharge. However, given variations in patient clinical complexity across timepoints, causation cannot be established. These findings reinforce the value of consistent occupational therapy presence in ICU to support functional recovery, delirium management, PADL retraining, and continuity across the ICU–ward transition. While the results are encouraging, further research is needed to determine the extent to which expanded OT provision directly influences recovery trajectories and longer-term patient outcomes.
Footnotes
Author contributions
JB proposed and developed the service evaluation. Data collection quality control was provided by JB and JS. Ideas were developed further with ES. All authors contributed to and approved the final manuscript. VS provided expertise with the statistical strategy.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study/research is funded by the National Institute for Health and Care Research (NIHR) Bristol Biomedical Research Centre (BRC). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.