
Abstract
Background:
Mechanical ventilation is a common and often lifesaving intervention that is utilised in intensive care. However, the practices can vary between centres. Through this national survey we aim to gain more information about different strategies adopted across the UK.
Methods:
All adult intensive care units in the UK were approached to participate. The questionnaire was developed with an electronic survey engine and conducted between 09/11/2023 and 01/04/2024 (Survey Monkey®). The survey included questions on ventilator modes, settings, protocols/pathways, rescue strategies, immediate post-extubation period and follow-up.
Results:
There were 196 responses from 104 hospitals. The most widely adopted start-up ventilation mode was pressure-regulated volume-controlled mode. For acute hypoxaemic respiratory failure (AHRF), most of respondents reported full (39.8%) or partial compliance (58.1%) with the ARDSnet protocol, with PEEP settings being the commonest deviation. Prone positioning (99.0%), followed by recruitment manoeuvres (91.3%) were commonly used rescue measures during AHRF. APRV (55.7%), inhaled (51.3%) and systemic pulmonary vasodilators (44.1%) were also commonly used. Conservative oxygen targets (SaO2 of 88%–92%) were commonly adopted (70.6%). As a care bundle, intermittent ETT cuff pressure monitoring was more common (65.5%) than continuous cuff pressure monitoring (20.0%). Propofol and alfentanil were the most common initial sedative and analgesia (99.5% and 56.9%) respectively. Routine volatile anaesthetic use was rare.
Conclusions:
Our survey has shown significant variation of practice in common but crucial elements of management of patients receiving mechanical ventilation. We hope the results in our survey highlight potential future areas of research.
Collaborators
South-coast Peri-operative Audit and Research Collaborative (SPARC)
Severn Trainee Anaesthetic and Critical Care Research group (STAR)
Collaborative research in Anaesthesia in the Northeast (CRANE)
Introduction
Mechanical ventilation is a common and often lifesaving intervention that is utilised in intensive care units across the world. Between 2022 and 2023, in England, Northern Ireland and Wales, over 88,000 patients were admitted to ICU for advanced ventilation support. 1 Whilst there are specific guidelines on managing a patient during mechanical ventilation, ventilation practices vary between centres. Ventilation adjuncts such as sedation, fluid management, selective digestive decontamination (SDD), can also influence patient outcomes. 2 There is currently limited information available regarding the different ventilation and patient management strategies adopted across the UK, reflected in diverse practices and the lack of implementation of a uniform therapeutic strategy by authoritative intensive care bodies.
Therefore, we designed a survey to collate detailed information on current management practices adopted for ventilated patients across the UK. This information will feed into discussion and guideline generation to further improve outcomes for mechanically ventilated patients. The specific aim of this survey is to identify the following practices regarding mechanically ventilated patients in intensive care units across the UK.
To assess current mechanical ventilation practices including ventilatory modes, weaning, recruitment manoeuvres and approaches used during the post-extubation period.
To determine the use of specific guidelines/protocols/pathways.
To determine routine and rescue management strategies including sedation, paralysis, proning, fluid balance and pharmacological strategies adopted to treat mechanically ventilated patients.
To assess the post discharge approach and any specific rehabilitation programmes offered in different units.
To assess different units’ involvement of patients in clinical trial.
Methods
This was a national survey aimed at intensive care physicians. The survey was designed by the Perioperative and Critical Care theme within the National Institute for Health and Social Care Research (NIHR) Southampton Biomedical Research Centre, and an internal pilot of the questionnaire was conducted at the General Intensive Care unit, University Hospital Southampton prior to wider dissemination. All adult intensive care units (ICU) including general and specialist units in the UK were approached to participate in this survey. The survey was conducted between 09/11/2023 and 01/04/2024. The survey invitation was placed on the website of the ICS. We further reached out to intensive care medicine trainee research networks and critical care operational delivery networks to disseminate the survey to their appropriate regions. The electronic survey was accessible through a hyperlink or QR code. We targeted consultants working in each ICU as they represent a senior medical workforce for each unit. Multiple methods of approach were tried to facilitate the response rate. The questionnaire was developed and delivered via an electronic survey engine (Survey Monkey Inc, San Mateo, California, USA).
This was a voluntary survey sent to the healthcare professionals and implied consent was assumed by their participation. The survey contained 31 questions (Appendix 1). The survey questionnaire incorporated the following specific sections:
Responder’s grade.
Contextual information describing the unit and hospital size.
Typical start-up and weaning ventilation modes and the use of closed-loop ventilation modes.
Use of daily sedation interruption, continuous/intermittent endo-tracheal tube (ETT) cuff pressure monitoring, closed/open tracheal suction catheter systems, supraglottic secretion drainage, selective digestive decontamination (SDD) and gastrointestinal stress ulcer prophylaxis.
The strategies adopted for sedation, paralysis, recruitment manoeuvres, positive end-expiratory pressure (PEEP) titration, ventilator settings, neuromuscular agents, daily fluid balance and conservative targets of oxygen saturation (SaO2), partial arterial pressure of oxygen (PaO2), partial arterial pressure of carbon dioxide (PaCO2), and potential of hydrogen (pH).
Use of specific guidelines/protocols/pathways for early mobilisation, suitability for extubation, sedation assessment and management, screening for delirium and management, ventilation weaning and setting of PEEP.
Ventilation and rescue strategies for patients with acute hypoxaemic respiratory failure (AHRF).
Timing of tracheostomy.
Approaches used (non-invasive ventilation (NIV), continuous positive airway pressure (CPAP) and high flow nasal oxygen (HFNO)) during the post-extubation period.
Availability of facilities such as bispectral index (BIS) for sedation monitoring, train of four for neuromuscular blockade, thoracic and cardiac ultrasound, oesophageal balloon for measuring transpulmonary pressure and indirect calorimetry.
Post discharge approach and any specific rehabilitation programmes offered.
Involvement of patients into clinical trials.
Data collected for this study was anonymised and stored electronically on a University Hospital Southampton trust computer in a locked area. Data collection and storage followed the data protection act and the policies of the hospital. Data were presented as numbers and percentages and the results were analysed within SurveyMonkey. The graphics were generated by GraphPad Prism software version 10.2.0 La Jolla California, USA.
Results
Characteristics of respondents
There were 196 responses received from 104 hospitals across the UK. Compared to the total number of hospitals with an ICU of 241 based on data from the Intensive Care National Audit & Research Centre and the Scottish Intensive Care Society Audit Group this gave a response rate of 43.6% nationally.3,4 The response rate from England was 45.4%, and from Scotland, Northern Ireland and Wales were 40.9%, 44.0% and 21.4% respectively (Figure 1). The responses were from general intensive care units (85.7%), specialist cardiac intensive care units (4.6%), specialist neurology intensive care units (4.1%) and combined general and specialist ICUs (4.6%). The median number of ICU beds was 16 with a median 600 available hospital beds. Most responses were from consultants (96%).
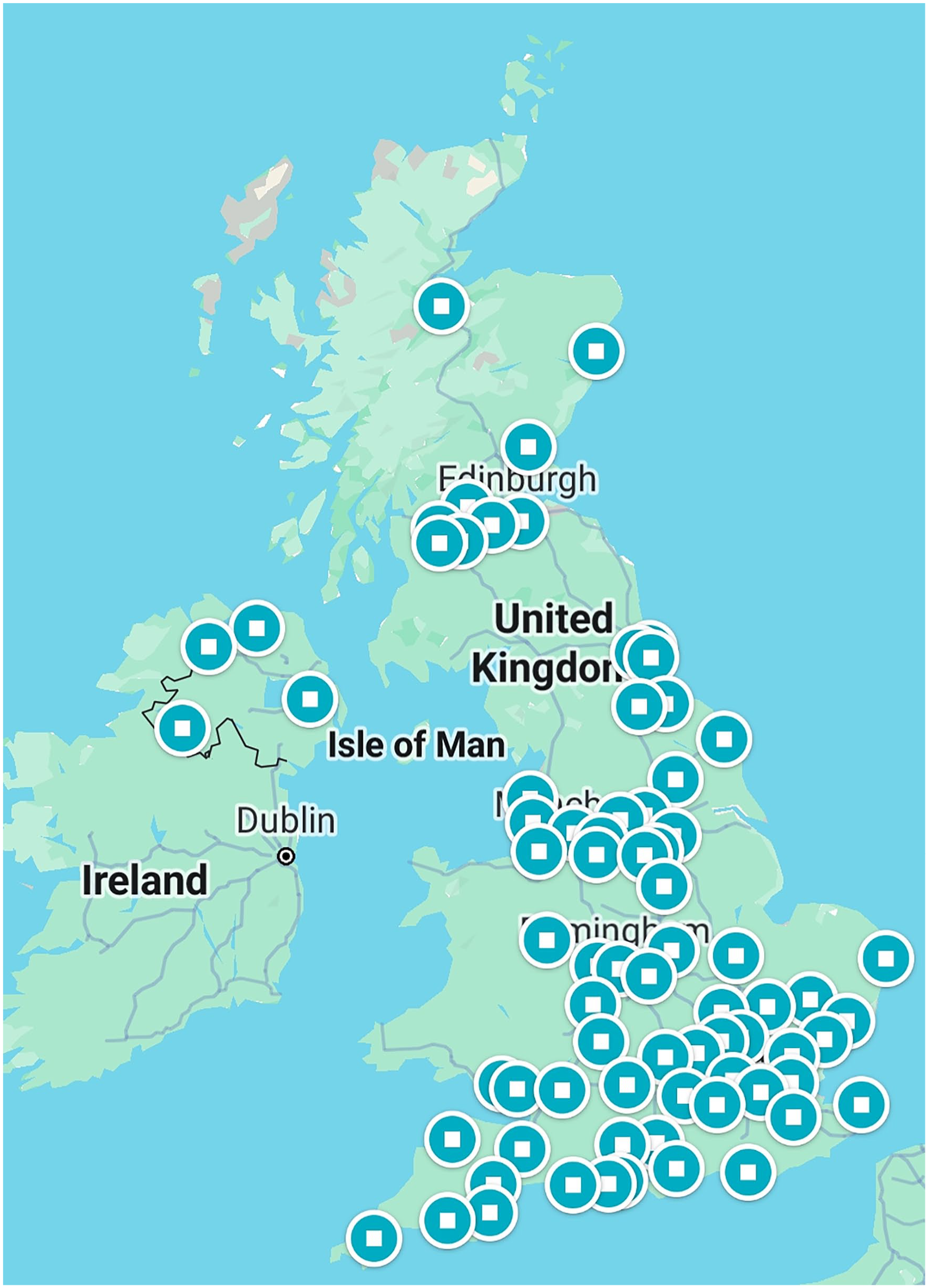
A pictorial representation hospital where responses obtained.
Modes and setting of ventilation
The initial start-up mode of mandatory ventilation included pressure regulated/adaptive pressure ventilation with target tidal volumes (39.5%) followed by synchronised intermittent mandatory ventilation (SIMV) (22.0%), pressure-controlled ventilation (19.0%) and closed loop (e.g. adaptative supportive ventilation (ASV, Hamilton Medical, Bonaduz, Switzerland) or neurally adjusted ventilatory assist (NAVA, Getinge, Gothenburg, Sweden) etc.) ventilation modes (10.3%). Airway pressure release ventilation (APRV) was rarely utilised as an initial start-up mode of ventilation (0.5%). Other ventilator modes included synchronised intermittent mandatory ventilation – pressure control (SIMV-PC), synchronised intermittent mandatory ventilation – pressure regulated volume control (SIMV-PRVC), and SIMV-autoflow. Once patients started to trigger ventilation, the common ventilator mode used was pressure support ventilation (PSV) (60.5%), followed by SIMV-PC (12.3%), closed loop ventilation (7.7%), SIMV-VC (7.2%) and bilevel ventilation (6.7%).
When asked specifically about the use of closed loop ventilation modes, most said they did not use this mode of ventilation (76.9%). Only 12.8% said they used adaptive support ventilation (ASV). Other closed loop modes were Automode (Siemens, Munich, Germany) (5.6%) and INTELLIVENT-ASV (Hamilton Medical, Bonaduz, Switzerland) (2.6%). NAVA was rarely used (0.5%).
When asked about tidal volume targets, most used 6.1–8.0 ml/kg/predicted body weight (PBW) (51.6%) followed by 4.0–6.0 ml/kg/PBW (45.4%). An unrestricted tidal volume target was rare (2.6%). Ventilator settings were limited to peak pressures (86.8%), plateau pressure (60.7%) and driving pressure (38.2%). About 14.7% of respondents reported they limit the mechanical power generated by the ventilator. When asked about guidance and variables used to titrate PEEP, most said they use the degree of hypoxia (80.9%) to titrate PEEP. Other measures to titrate PEEP were recruitability using hysteresis via pressure-volume (P-V) loop (47.4%), ARDSnet protocol (43.8%), plateau pressure (41.2%), driving pressure (38.1%), peak airway pressure (35.1%), oesophageal pressure (2.6%) and end-expiratory transpulmonary pressure (2.1%). Recruitability assessed by computer tomography scan and ultrasound chest were utilised by 8.8% and 7.2% respectively. The use of functional imaging (e.g. electrical impedance tomography) was rare (2.6%).
Acute hypoxaemic respiratory failure
When asked about the primary ventilation strategy for mechanically ventilated patients with AHRF, most were partially compliant with ARDSnet protocol with deviations in PEEP recommendations (48.4%), followed by full compliance of ARDSnet protocol (39.8%) and airway pressure ventilation (16.7%). Eleven respondents (5.9%) said they did not use the ARDSnet protocol. When the question was about the use of recruitment manoeuvres for patients with AHRF, APRV ventilation was commonly used (55.7%). The use of recruitment manoeuvres whilst managing patients with AHRF is presented in Figure 2.
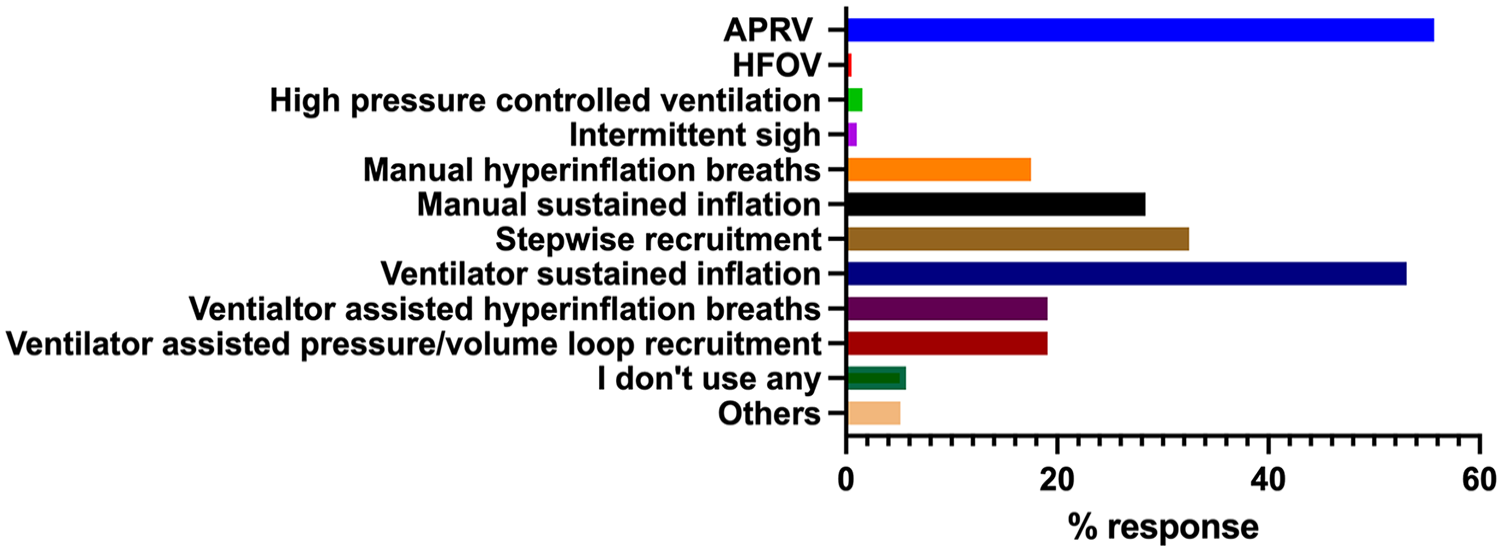
The recruitment measures used during mechanical ventilation of patients with acute hypoxaemic respiratory failure.
We further asked about what rescue measures were available at individual centres for patients with AHRF when there is no improvement despite maximal ventilation. By far, the two commonly available rescue measures for patients with respiratory failure was the use of proning (99.0%) and recruitment manoeuvres (91.3%). Inhaled (51.3%) and systemic (44.1%) pulmonary vasodilators were also commonly available. ECMO (18.5%), ECCO2 (3.1%) and HFOV (3.1%) were less frequently available.
Prone positioning was used by most as a rescue measure (99.0%) and the indication for prone positioning is mostly defined by the PaO2/FiO2 ratio (51.0%). Routine use of prone positioning was rare (8.8%). The duration of a prone cycle was 16–18 h (59.9%), followed by 12–16 h (31.8%). Longer duration of prone cycles (>18 h) was used by 4.2%. Most continued to prone until improvement in PaO2/FiO2 (43.5%). Only 5.0% respondents said they had a dedicated prone team.
Permissive gas targets for all critically ill mechanically ventilated patients
The survey also questioned about permissive targets for oxygenation (PaO2, SaO2, PaCO2 and pH for all critically ill mechanically ventilated patients. Most set a conservative SaO2 target of 88%–92% (70.6%), PaO2 of 8.1–9.0 kPa (50.6%) with no PaCO2 targets (59.9%) and a pH range of 7.21–7.25 (47.3%) (Figure 3).
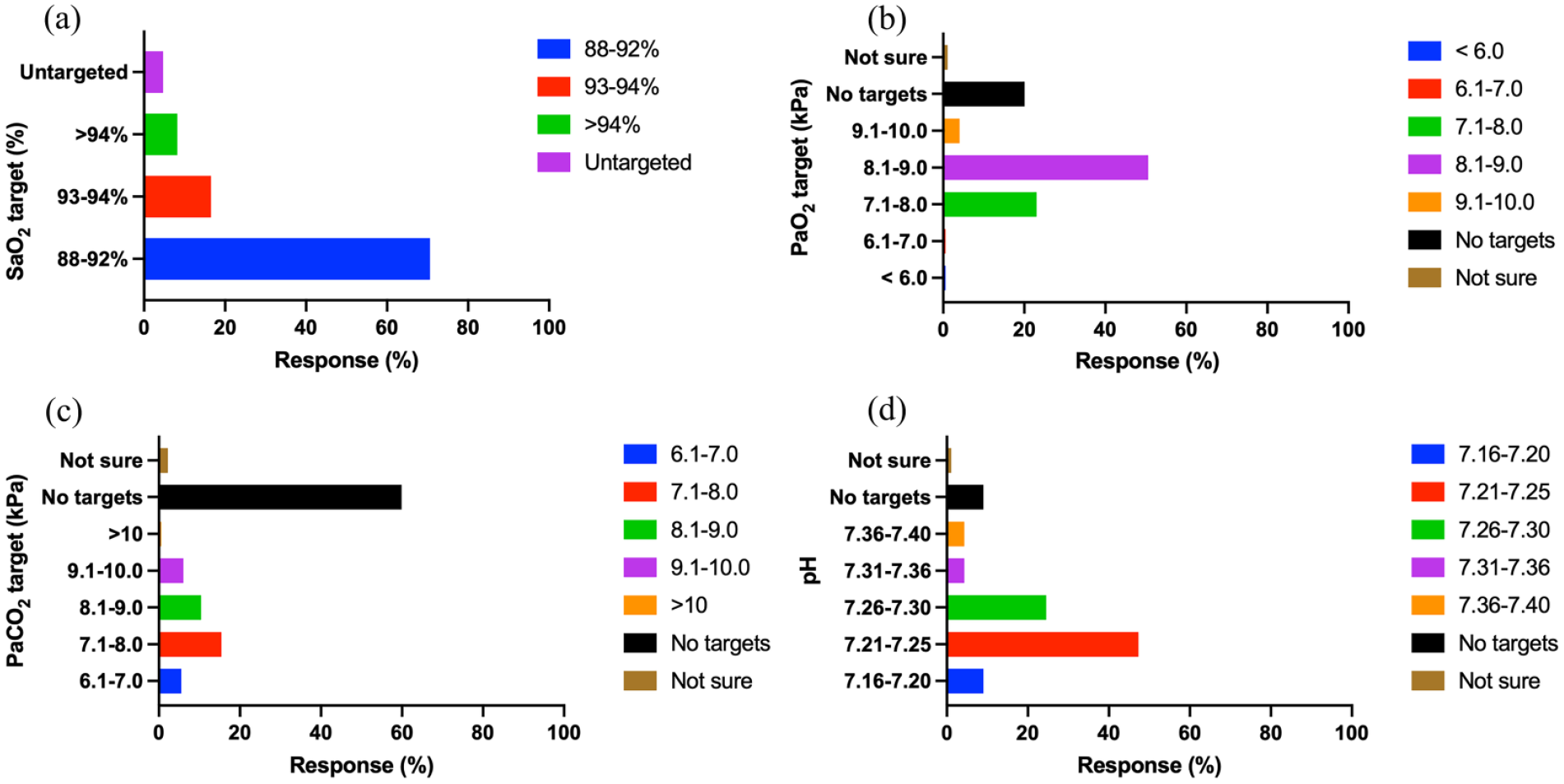
The permissive targets for the variables SaO2 (%) (a), PaO2 (kPa) (b), PaCO2 (kPa) (c) and pH (d) for all critically ill mechanically ventilated patients.
Fluid use and daily fluid balance strategy for all critically ventilated patients
When the question was about fluid balance strategy in critically ill ventilated patients, the preferred daily fluid balance status was euvolaemia (61.6%), followed by dry (27.7%) and no specific targets (10.2%). The preferred resuscitation fluid was balanced crystalloids (95.3%). Few respondents 2.3%, 1.2% and 0.6% used resuscitation fluids in the forms of colloids- albumin, semi-synthetic colloids and saline respectively. When negative fluid balance was desired, this was achieved by a combination of diuretics and fluid restriction (64.4%). Hemofiltration was not used first-line to achieve negative fluid balance.
Specific guidelines/protocols/pathways and other measures available
This question was based on the use of specific guidelines/protocols/pathways for mechanically ventilated patients. Most units had specific guidelines for key components of the care of managing ventilated patients, particularly for screening for delirium and management (89.8%) (Figure 4).
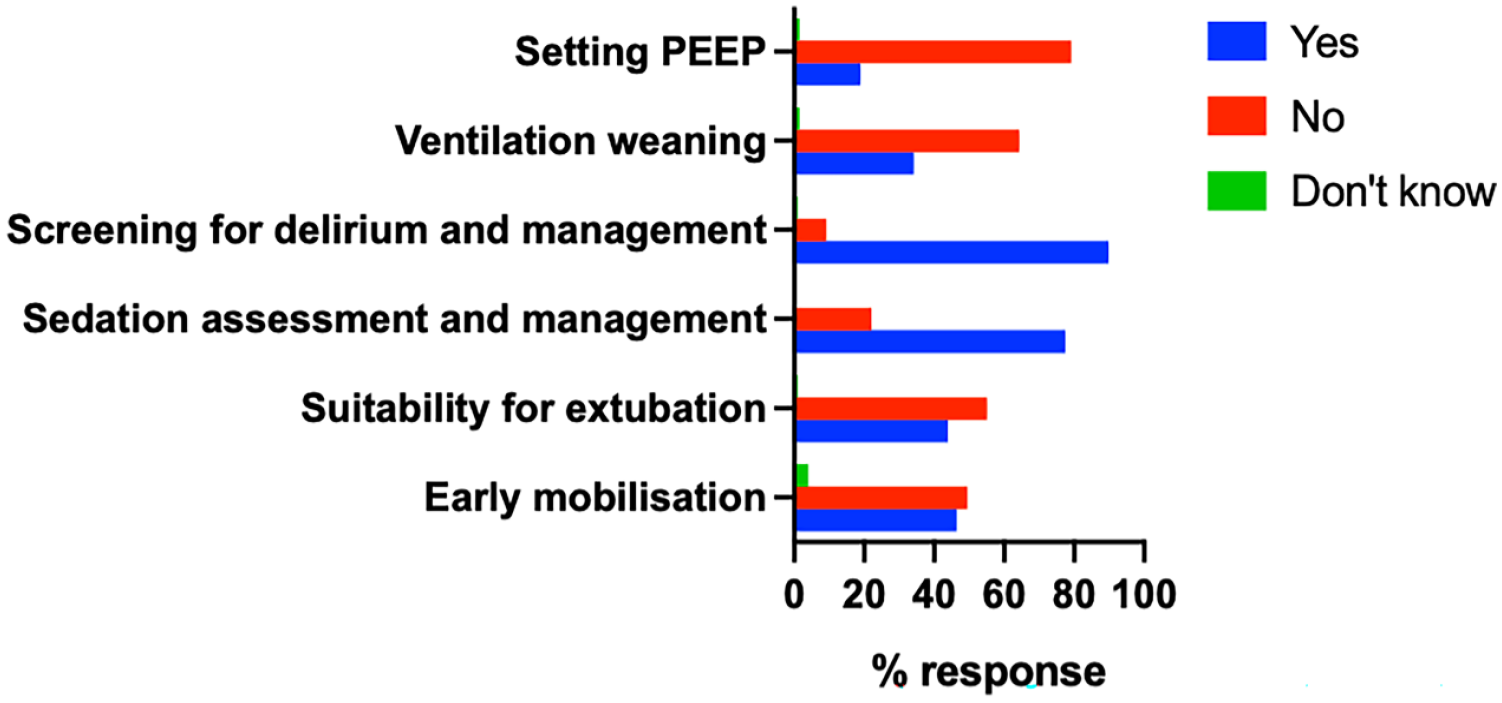
The use of dedicated pathways/protocols/guidelines.
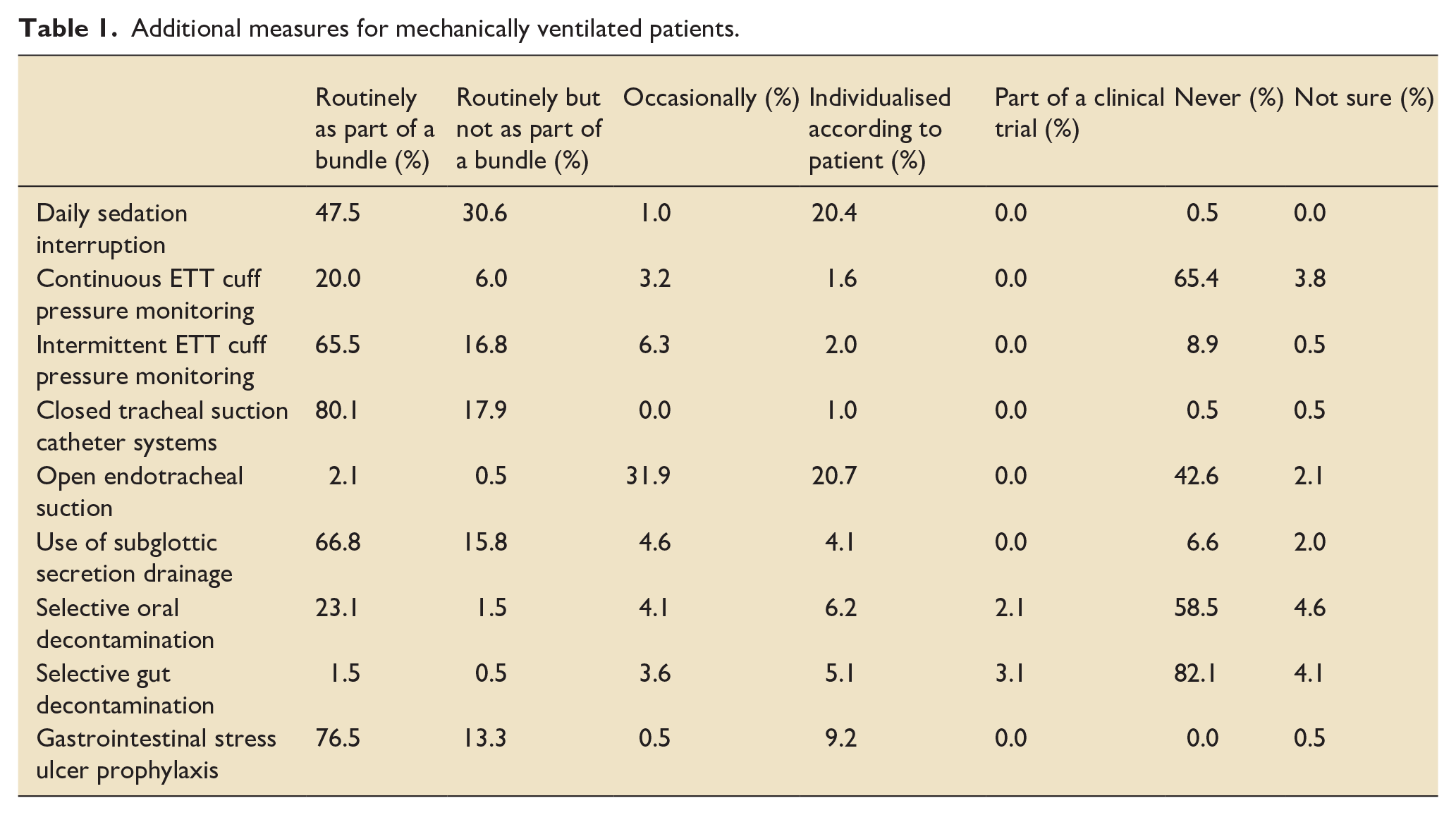
The survey also questioned other measures such as daily sedation interruption, cuff pressure monitoring, tracheal suction systems, subglottic secretion drainage, SDD, and gastrointestinal stress ulcer prophylaxis, when managing mechanically ventilated patients (responses are detailed in Table 1). Moreover, routine use of BIS for sedation monitoring (8.7%), oesophageal balloon for transpulmonary pressure monitoring (0.0%), indirect calorimetry for quantifying energy expenditure (1.0%) and thoracic ultrasound for assessment of lung recruitability (5.7%) and thoracic ultrasound for ventilator weaning (1.5%) were rare.
Additional measures for mechanically ventilated patients.
Sedation for mechanically ventilated patients
These questions aimed to seek the common sedation drugs and the preferred method of delivery. The preferred choice of sedation delivery was as a continuous infusion (80.5%) followed by a combination of continuous and bolus regimen (18.5%). Bolus delivery alone was rare (0.5%). Propofol was the most common initial sedative for mechanically ventilated patients (99.5%). A few respondents reported the use of dexmedetomidine (3.1%), midazolam (1.5%), and clonidine (1.5%) as initial sedative medications. Alfentanil was the commonest analgesia (56.9%), followed by fentanyl (27.7%), remifentanil (18.0%) and morphine (7.7%). No units reported the use of ketamine as initial analgesia. Sedation levels were primarily monitored with sedation scores, with the Richmond Agitation Sedation Scale (RASS) being the most common (88.7%), followed by the Ramsey Sedation Scale (4.6%). Others (4.6%) used a combination of RASS + BIS, patient state index (Sedline PIS) and electroencephalograms (EEG). When asked about the use of volatile anaesthetic agents, 58.5% of respondents reported never using volatile anaesthetic sedation in ICU followed by rare use (29.7%) and sometimes (10.3%).
Ventilation weaning, the use of NIV/CPAP/HFNO post extubation and timing of tracheostomy
When asked who lead the initiation and management of ventilator weaning, 43.8% said this was done by the senior medical team (consultants and/or ST6+) followed by all members of the medical team (16.5%). Nurse (2.1%) and physiotherapy (2.1%) led weaning was rare. However, 30.4% of respondents reported a combination of medical, nursing and physiotherapists led ventilator weaning.
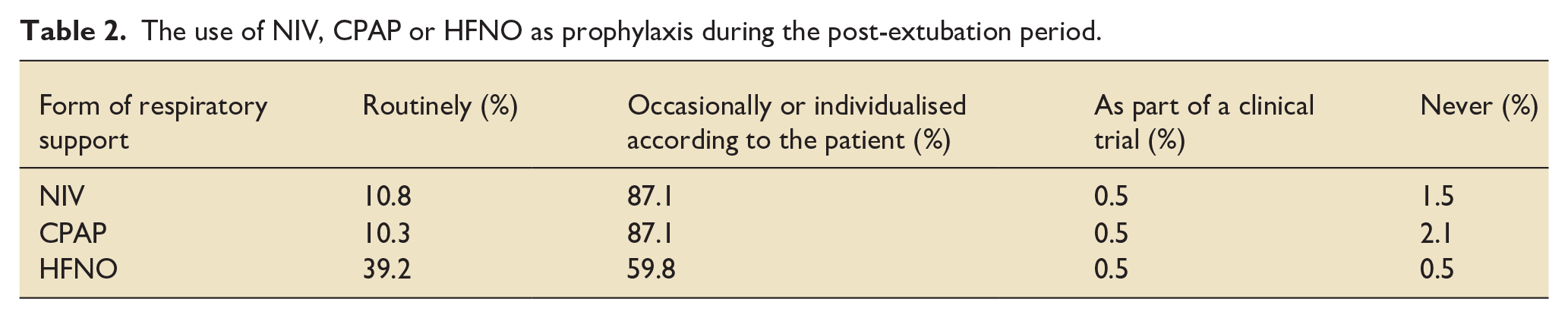
We asked about the prophylactic use of non-invasive ventilation (NIV), continuous positive airway pressure (CPAP) or high flow nasal oxygen (HFNO) during the post-extubation period. We classified the answers as these interventions were routinely given, occasionally, individualised, according to patient, as part of clinical trial or never. Most expressed that they use these occasionally or individualised according to the patient and the routine use of these interventions was not common. However, in comparison to NIV or CPAP, HFNO was more frequently used as prophylaxis during post-extubation period (Table 2).
The use of NIV, CPAP or HFNO as prophylaxis during the post-extubation period.
Respondents were also asked about the timing of tracheostomy insertion on their units. The most selected timing option was ‘during 7–14 days of mechanical ventilation’ (59.0%). It should be noted 27.2% surveyed selected ‘other/comment’ and most of these comments expressed that the decision is based on patient/pathology specific for example, early in Guillain–Barré syndrome and posterior fossa pathology. Several respondents felt there was a need to fail an extubation attempt prior to tracheostomy insertion.
Participation in clinical research and data collection
When asked about their involvement in research, 43.1% of the participants reported that they were currently taking part in research related to mechanical ventilation. Additionally, a large majority (87.1%) reported that they were able to participate in research. Furthermore, most of the participants (68.0%) stated that they had an electronic database of mechanically ventilated patients, while 60.9% conducted regular audits of their current practices.
Follow-up and the availability of rehabilitation programmes
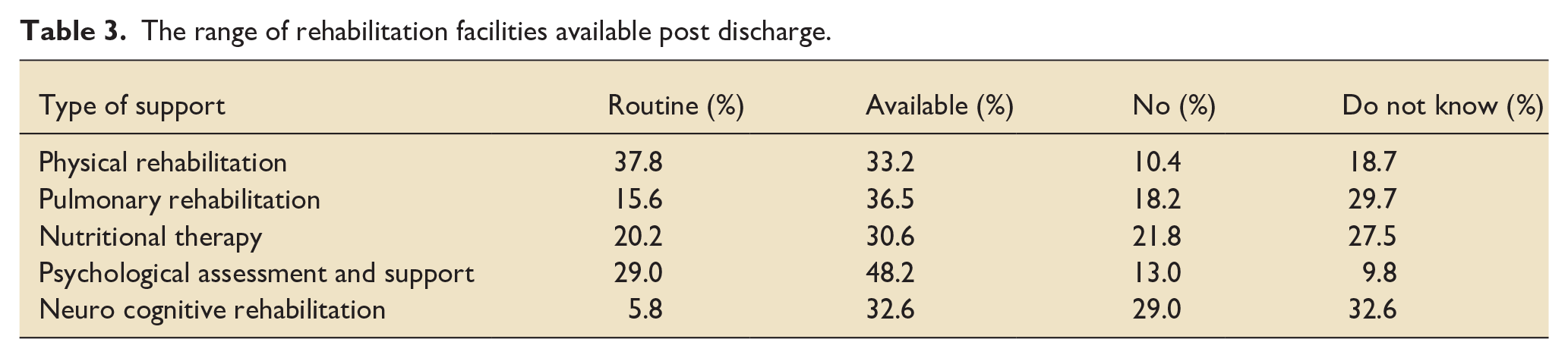
Once patients were discharged from hospital, 74.2% of respondents reported that they routinely follow-up their patients, with 10.8% saying no follow up was offered and 4.1% being unsure. After hospital discharge, there was a mixed response for the availability of specialist rehabilitation programmes for patients who received mechanical ventilation (Table 3).
The range of rehabilitation facilities available post discharge.
Discussion
This was the first cross-sectional national survey to evaluate mechanical ventilation practices across the UK comprehensively. The response rate was 43.6%, primarily from ICU consultants from a broad range of intensive care units across the UK. This is a response rate similar to that of other ICU national surveys. 5 This detailed survey explored all facets of the care of mechanically ventilated patients, including, ventilator modes, settings, sedation practices, permissive targets, use of pathways/guidelines/protocols and rescue strategies during AHRF.
The main findings were
(1) Common ventilation start-up modes were pressure regulated/adaptive pressure ventilation (PRVC) targeted tidal volumes and APRV ventilation was used as a rescue strategy rather than primary ventilation strategy and the use of closed loop ventilation modes was rare.
(2) Permissive oxygen targets with SaO2 of 88%–92% or PaO2 of 8.1–9.0 kPa were adopted by most for all critically ill mechanically ventilated patients.
(3) Pathways/guidelines/protocols were commonly used for sedation assessment and delirium screening but less so for early mobilisation, suitability for extubation, ventilation weaning and PEEP setting.
(4) Intermittent ETT cuff pressure monitoring and closed tracheal suction systems (CTSS) were more common and the use of SDD was rare.
(5) For patients with AHRF, most adopted partial compliance with ARDSnet protocol with deviations from PEEP recommendations. Ventilator sustained inflation was the most common recruitment manoeuvre and rescue measures included prone positioning, pulmonary vasodilators and APRV ventilation.
(6) Continuous sedation/analgesia with propofol and alfentanil was preferred with monitoring by RASS, volatile agent use was rare.
The ideal start up ventilation mode for all critically ill patients is not fully defined. Although there are theoretical advantage of reduced barotrauma and improved patient comfort with PRVC mode compared to conventional volume-controlled (VC) ventilation, there are no specific improvement in patient-centred outcomes. 6 The use of APRV ventilation has become prevalent during the COVID-19 pandemic and consistent with our previous finding, it was commonly used as a rescue mode than primary ventilation strategy.7,8 While there are pros and cons to different ventilator modes, head-to-head trials investigating different start-up modes of ventilation are lacking, and further research is needed into the optimal initial ventilation mode for all mechanically ventilated patients and patients with AHRF. Our results demonstrated that most adopted a conservative oxygen target for all mechanically ventilated patients. A previous survey has shown that critical care clinicians prefer higher oxygen saturations in ARDS patients 9 and indeed, national guidance still favours conservative targets only if there is a risk of hypercapnic respiratory failure. 10 The common use of conservative oxygen target for mechanical ventilated patients was surprising and this trend is possibly due to the increased awareness of the dangers of hyperoxia. The ongoing large national and international trials will help to answer this ongoing debate.11,12
Prone positioning has become a routine practice as a rescue to improve oxygenation in patients with AHRF. In our study, proning was the commonest (99%) rescue technique for refractory hypoxaemia. Inhaled and systemic pulmonary vasodilators were also commonly used. The use of pulmonary vasodilators and recruitment manoeuvres has substantially increased when compared to the previous survey conducted in 2014 on management strategies of ARDS patients. 5 This is despite the lack of reliable evidence of improved outcomes.13,14 This likely reflects clinicians being faced with large numbers of refractory hypoxaemic patients during the peak of the COVID-19 pandemic.
CTSS have theoretical advantage of being an easy technique with minimal risk of aerosol generation. 15 A recent systematic review suggests CTSS was non-superior over open tracheal suctioning systems (OTSS) with no difference in ventilator-associated pneumonia, mortality or length of ICU stay between CTSS and OTSS.16,17 However, the increased use is likely due to the recent COVID-19 pandemic. 18 In our survey, routine intermittent ETT cuff pressure monitoring as part of a bundle is more common (65%) than continuous ETT cuff pressure monitoring (20%). While a systematic review and meta-analysis of 14 RCTs with 2080 patients suggest continuous cuff pressure monitoring may reduce the incidence of ventilator acquired pneumonia (VAP) and duration of mechanical ventilation, a large trial of 600 patients recently reported no real benefits with continuous cuff pressure monitoring.19 –21 This result, coupled with continuous cuff monitoring being relatively new, may explain the lack of routine use.
Routine use of selective oral decontamination (SOD) was reported by 23%. A possible explanation for the low rates of SOD was the withdrawal of recommendations for its use by NICE and the ICS in 2016. This was triggered by evidence that suggested oral chlorhexidine in non-cardiac surgery patients did not reduce the incidence of VAP. 22 However, chlorhexidine oral decontamination is currently recommended only for patients undergoing thoracic/cardiac surgery, with evidence suggesting perioperative usage may reduce the risk of some post-operative infections.23,24 Similarly, consistent with previously published surveys, routine use of SDD was rare (<2%) despite cumulative evidence from a large systematic review and metanalysis of 32 clinical trials suggesting potential mortality benefits and reductions in ventilator-associated pneumonia. 25 Moreover, a sub-group analysis of the SuSSICU trial suggests that patients with acute brain injuries may have additional mortality benefits from SDD. 26 Further studies are needed to evaluate combination interventions as a bundle for preventing VAP and improving mortality.
Our other findings include: (1) most patients had a routine follow up after discharged from hospital, (2) the availability of physical, pulmonary, nutritional, psychological, and neurocognitive rehabilitation programmes after hospital discharge was variable for patients who received mechanical ventilation. Rehabilitation after critical care is an essential part of recovery from critical illness. NICE has highlighted the need for high-quality rehabilitation as a priority for patient health and well-being. 27 Indeed, rehabilitation and follow-up are part of the guidelines for providing intensive care services. 28 Rehabilitation services seem to have increased since a previous survey in 2014 which showed only 27.3% of ICUs had a specific ICU follow-up service compared to our finding of 74% routinely following up patients. 29 Despite the increase availability of services, research is still needed to demonstrate whether rehabilitation translates into improved long-term outcomes as the existing research is heterogenous and mixed. 30
Our survey does have several limitations. Although in line with other surveys, our response rate was less than 50% and we could not separate multiple responses from the same unit, which would affect the generalisability of the results. We also had several free texts comments that we were unable to analyse quantitatively. Some of these reflect situations the authors did not envisage for example, use of ventilator modes with different names in the question. We could not separate responses from specialist centres from general units, which may have implications regarding specific treatment strategies. However, separating these responses would give limited data and unlikely to be generalisable. Another potential weakness of this survey is that we sought responses from consultants for the reasons outlined above and this may have introduced selection bias in reflecting the real-world situation. For example, only 2.1% of respondents reported physiotherapists initiated and lead the ventilator weaning. If we had asked physiotherapists, based on the author’s experience, it is likely this number would be higher, particularly around the weaning of patients in an ICU for several weeks. Despite these limitations, this is the first national survey to comprehensively evaluate the management of mechanically ventilated patients in ICU.
Conclusions
Our survey has shown that there is significant variation of practice in common but crucial elements of management of patients receiving mechanical ventilation. This likely reflects the heterogenicity of ICU patients with treatments needing individualised therapy. However, some of this variation also reflects a lack of specific guidelines and research. The responses in our survey highlight future areas of research to be explored. Importantly, as studies are developed, we have shown that 87% of respondents feel their ICU could participate in future mechanical ventilation research.
Supplemental Material
sj-docx-1-inc-10.1177_17511437241292190 – Supplemental material for Management of adult mechanically ventilated patients: A UK-wide survey
Supplemental material, sj-docx-1-inc-10.1177_17511437241292190 for Management of adult mechanically ventilated patients: A UK-wide survey by James Ward, Isis Terrington, Katie Preston, Alexander Smith, Thomas Roe, Jonathan Barnes, Emma Allen, Sandra Lima, Rebecca Cusack, Michael P.W. Grocott, Ahilanandan Dushianthan and the South-coast Peri-operative Audit and Research Collaborative (SPARC) in Journal of the Intensive Care Society
Footnotes
Acknowledgements
We thank all the survey participants for their contribution. The study was conducted by NIHR Southampton Biomedical Research Centre and University of Southampton. We would like to thank all the General Intensive Care unit consultants at University Hospital Southampton for their involvement in the internal pilot validation of the survey questionnaire. We would also like to thank The Intensive Care Society for advertising this survey on their website, South-coast Peri-operative Audit and Research Collaboration (SPARC) for taking the lead, advertising, and distributing the survey, Severn Trainee Anaesthetic and Intensive Care Research group (STAR) and Collaborative research in Anaesthesia in the North East (CRANE), trainee research networks in anaesthetics/critical care who have helped with collecting survey responses in their region. Kashir Raza for help contacting ICUs and distributing the survey.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: MG holds an NIHR Senior Investigator award and is in part funded by the NIHR Southampton Biomedical Research Centre. This study received no extra funding.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.