
Abstract
Background:
Critical care nurses (CCNs) face difficulties and stress when caring for patients with delirium, and the level of delirium-related stress may be related to gaps in their knowledge and skills.
Aim:
This study aimed to assess the impact of a psychoeducational and relaxation program on reducing the stress of CCNs caring for patients with delirium in intensive care units (ICUs) in Taiz city, Yemen.
Methods:
From June to the end of December 2022, a quasi-experimental study was conducted among 60 CCNs from two ICUs of Al-Thawra Hospital in Taiz. Demographic characteristics were collected using a pre-designed data collection sheet, and the levels of CCNs’ stress were measured using the Delirium Nursing Stress Scale (DNSS). To assess the impact of the developed psychoeducational and relaxation program, stress levels were measured before and after the program, as well as at a 3-month follow-up for long-term impact. The association of demographic characteristics with delirium-related stress was also studied. Data were then analyzed using appropriate statistical tests at a significance level of <0.05.
Results:
Before the program, the mean score of CCNs’ stress was 60.48 ± 9.51, corresponding to a moderate stress level of 86.7%. However, this score was significantly reduced to 30.98 ± 4.35 immediately after the program and was sustained at 33.13 ± 5.31 3 months after the program, corresponding to a mild stress level. The highest mean score of CCNs’ stress related to caring for patients with delirium was observed before the program for all causes of stress on the DNSS, being 4.95 ± 1.77 for the nursing environment, 9.37 ± 2.16 for relationships with peers, 14.40 ± 4.02 for knowledge about delirium, and 31.77 ± 5.78 for nursing practice and work. However, the mean stress scores related to all these causes showed a significant reduction after the program (2.85 ± 0.95, 4.70 ± 1.33, 7.20 ± 1.67, and 16.23 ± 2.80, respectively) and at the 3-month follow-up (3.15 ± 1.05, 4.95 ± 1.23, 7.67 ± 1.66 and 17.37 ± 3.57, respectively). On the other hand, the mean score of total stress for all DNSS items showed a significant reduction from 60.48 ± 9.51 before the program to 30.98 ± 4.35 after the program and 33.13 ± 5.31 at the 3-month follow-up. There were no statistically significant differences in the mean scores of delirium-related stress before and after the program, or at the 3-month follow-up for any of the demographic characteristics of CCNs.
Conclusion:
Psychoeducational and relaxation programs have a positive impact on stress reduction in CCNs caring for patients with delirium, improving the standard of care provided to these patients. Regular assessment of CCNs for delirium-related stress and educating them to acquire knowledge and skills are recommended to reduce this stress when caring for delirious patients.
Introduction
Delirium is characterized by an abrupt alteration in the baseline neurocognitive functions of patients, resulting in acute impairment of attention, consciousness, and cognition. According to the American Psychiatric Association, this condition is caused by an underlying medical problem rather than an established or emerging neurocognitive disorder. 1 Delirium incidence in patients admitted to intensive care units (ICUs) can vary widely depending on the study population, study design, and diagnostic criteria used. However, delirium is a common problem in ICUs and can have a significant negative impact on patient outcomes. Several studies have reported delirium incidence rates ranging from 60% to 80% in ICU patients.2–5
Critically ill patients and those with life-threatening conditions admitted to hospitals receive continuous and comprehensive care in ICUs. 6 Critical care nurses (CCNs) face several challenges when working in ICUs, including overwhelming workloads, dealing with dying patients, a negative social environment, and insufficient resources. 7 Other factors that contribute to their stress include difficult family relationships, conflicts with physicians, unskilled nursing personnel, time constraints, staff shortages, and violence. 8 The constant stress in the work environment and the demanding nature of critical care make CCNs highly susceptible to burnout. 9
The nursing role is widely perceived to be challenging, and stress can negatively impact nurses’ health and job satisfaction, ultimately affecting the quality of care provided to patients. Job-related stress has been linked to poor quality healthcare services, low productivity, decreased initiative, lack of motivation, enhanced resistance of thought, less interest in colleagues and facilities, and a lower sense of responsibility. 10 Caring for patients with delirium increases CCNs’ effort and frustration and raises their stress levels. Delirious patients are functionally worse than those without delirium and are therefore more dependent on CCNs for their care. Some patients may become hostile and combative during nursing care, interfering with the achievement of care goals and putting staff at risk of harm. As a result, delivery of nursing care takes longer and usually requires more CCNs.11,12
It has long been thought that dealing with behavior that challenges is time consuming and discouraging, making CCNs feel anxious about restraining agitated patients. Moreover, they are frequent targets of physical and verbal aggression by hyperactive delirium patients. Caring for delirious patients presents a psychological challenge for CCNs when determining the appropriate approaches to deal with such patients. As a result, CCNs either spend too much time planning what to do or react too quickly with worry, which makes care less efficient. CCNs usually complain of the unsupportive environment and managers when addressing patient care problems.13,14
Several studies have revealed the importance of educating and supporting CCNs caring for delirium to alleviate the stress they face that can negatively affect their care and practices. Therefore, support from a multidisciplinary critical care team is critical. This support can take the form of multidisciplinary team meetings, nursing team meetings, and meetings with management.15 –17 Without measures to modulate the stress response, the consequences of stress on CCNs’ physical health can be deleterious, as manifested by symptoms such as headache, fatigue, skin rashes, somatic disturbance, lower back pain, stomach aches, gastrointestinal disorders, hypertension, coronary artery disease, sleep disorders, and weight fluctuations.18,19
Earlier research on stress in nursing has found an association between occupational stress and personal judgment of emotional distress, as well as high rates of stress-related burnout and emotional illnesses.20 –22 Occupational stress can directly or indirectly affect the quality and quantity of critical care provided to patients and their families, compromising patient care.23,24 Although nurses are at high risk of job stress and burnout, they can benefit from the same stress management strategies they use to educate their clients. Nurses need to identify and manage workplace stressors and seek social support from colleagues to maintain a caring attitude toward patients. Stress management entails employing adaptive coping strategies in response to different situations.25 –27
Ideally, stress can be reduced to an acceptable level, allowing nurses to work optimally and comfortably. Accordingly, the first step is to assess the environment for the necessary changes, followed by implementing appropriate coping strategies. Different physical, mental, emotional/spiritual, and organizational strategies can be used individually or in combination.28,29 Implementation of various strategies to address stress issues has been suggested, including managing workload, promoting work-life balance, enhancing communication and teamwork through training and technology, and fostering a supportive and inclusive work culture. Furthermore, the need for collaboration between the healthcare professionals, the hospitals’ administrators and the healthcare policymakers to create an improved and sustainable working environment in the ICU has been emphasized. Addressing the above challenges and implementing the recommended strategies can improve the quality of patient care and the well-being of ICU staff. 30 Nurse satisfaction has been shown to be positively influenced by ICU design features such as lighting, privacy, layout, and equipment accessibility. 31 In Saudi Arabia, a study identified inadequate staffing and resources, high workload, and limited organizational support as the challenges facing ICU nurses, emphasizing the need for improvement. These findings underscore the importance of improving the work environment in the ICU for the well-being of nurses and the quality of patient care. 32 Therefore, this study aimed to assess the impact of a psychoeducational and relaxation program on reducing the stress of CCNs caring for patients with delirium in ICUs in Taiz city, Yemen.
Methods
Data collection and tools
Demographic characteristics of CCNs, including age, sex, level of education, marital status, duration of work in the ICU and participation in previous training on delirium, were collected using a pre-designed data collection sheet.
The Delirium Nursing Stress Scale (DNSS), a self-report tool developed by Suh and Yoo 33 and modified by Kim and Lee, 34 was used to measure stress levels in nurses caring for patients with delirium. This scale included 20 items across 4 sections: stress related to knowledge about delirium, nursing work environment, relationships with peers, and nursing practice and work. Each item was rated on a 5-point Likert scale from “not at all” to “extremely,” with a total score ranging from 20 to 100. Accordingly, stress was categorized into four levels: no stress (score 20), mild stress (score 21–46), moderate stress (score 47–73), and severe stress (score ⩾74). An Arabic-translated version of the scale (Supplemental File 1) The tool was validated by two psychiatrists and three professors of psychiatric nursing from the Faculty of Medicine and Health Sciences, Taiz University. The reliability of the DNSS tool was 0.89 as measured by Cronbach’s alpha.
Psychoeducational and relaxation program
Overview of the program
The psychoeducational and relaxation program was developed by the researchers after a three-month review of relevant materials and resources by two psychiatrists from Medicine department and five professors of psychiatric nursing and critical care nursing from Nursing department, the Faculty of Medicine and Health Sciences, Taiz University. The program had two components. One component involved the educating CCNs on the definition, causes, clinical manifestations, assessment, and nursing care plan for patients with delirium. The other component involved training CCNs in relaxation techniques, including problem-solving, deep breathing exercises, progressive muscle relaxation exercises, and meditation exercises and techniques.
The program was delivered over 11 h, five of which were theoretical and six practical hours. It consisted of 11 one-h sessions (one pre-assessment and 10 instructional) for 15 participants 3 days a week. Each session included an interactive lecture with videos and PowerPoint presentations, group discussions and practical training.
Program phases
The following phases were conducted to develop, implement and assess the impact of the program:
Stress assessment phase
In this phase, the stress of CCNs caring of patients with delirium was assessed over 1 month.
Program development phase
In this phase, the content and implementation strategy of the program, including the time and number of sessions and teaching methods, were discussed and developed over 2 months. In addition, the suitability of teaching location and facilities was assessed. The psychoeducational and relaxation program included 10 instructional sessions to educate CCNs about different aspects related to delirium and train them in relaxation strategies to reduce stress. These sessions included:
Session 1: Introduction, definition, subtypes, and incidence of the delirium
Session 2: Risk factors and causes of delirium
Session 3: Clinical manifestations and differential diagnosis of delirium from dementia and depression
Session 4: Screening tools used to assess delirium
Session 5: Prevention, treatment and nursing care plan for patients with delirium
Session 6: Identifying stress and methods for facing and managing it
Session 7: Problem-solving
Session 8: Deep breathing exercises
Session 9: Progressive muscle relaxation exercises
Session 10: Meditation exercises and techniques
Program implementation
Before implementing the 10 instructional sessions of the program, the researchers conducted a pre-assessment session to assess the stress levels of CCNs caring for patients with delirium using the DNSS tool and to collect demographic data. The CCNs were assessed at the end of each instructional session, and a report on the assessment results was presented at the next session to determine how well they understood the topics from the previous session. The researchers provided the participants with constructive feedback and guidance on areas for improvement.
Assessment of program impact
CCNs were assessed for stress reduction using the DNSS tool immediately after the completion of the program. A follow-up assessment was performed 3 months later to assess the long-term impact of the program on reducing stress.
Statistical analysis
Data were analyzed using the IBM SPSS Statistics software, version 26.0 (IBM Corp., Armonk, NY, USA). The normality of quantitative data distribution was verified by the Kolmogorov-Smirnov test. Categorical variables were expressed as frequencies and percentages, and continuous variables were expressed as mean and standard deviation (SD). The chi-square test was used to compare between categorical variables, and the repeated measures analysis of variance (ANOVA) was used to compare between the means of three related groups (before program, after program and follow-up). The independent-samples t-test for two groups and ANOVA for more than two groups were used to compare the mean score of stress level between different groups. Statistical significance was considered at a p-value < 0.05.
Ethical considerations
This study was ethically approved by the Institutional Review Board of the Faculty of Nursing, Assiut University, Assiut, Egypt (approval No. 3460022). In addition, permission to conduct the study was obtained from the Director General of Al-Thawra Hospital after explaining its purpose. Written informed consent was obtained from the CCNs after being informed of its purpose. The CCNs were also advised that the privacy and confidentiality of their data would be ensured. This study was conducted in accordance with the latest version of the Declaration of Helsinki.
Result
Demographic characteristics of CCNs
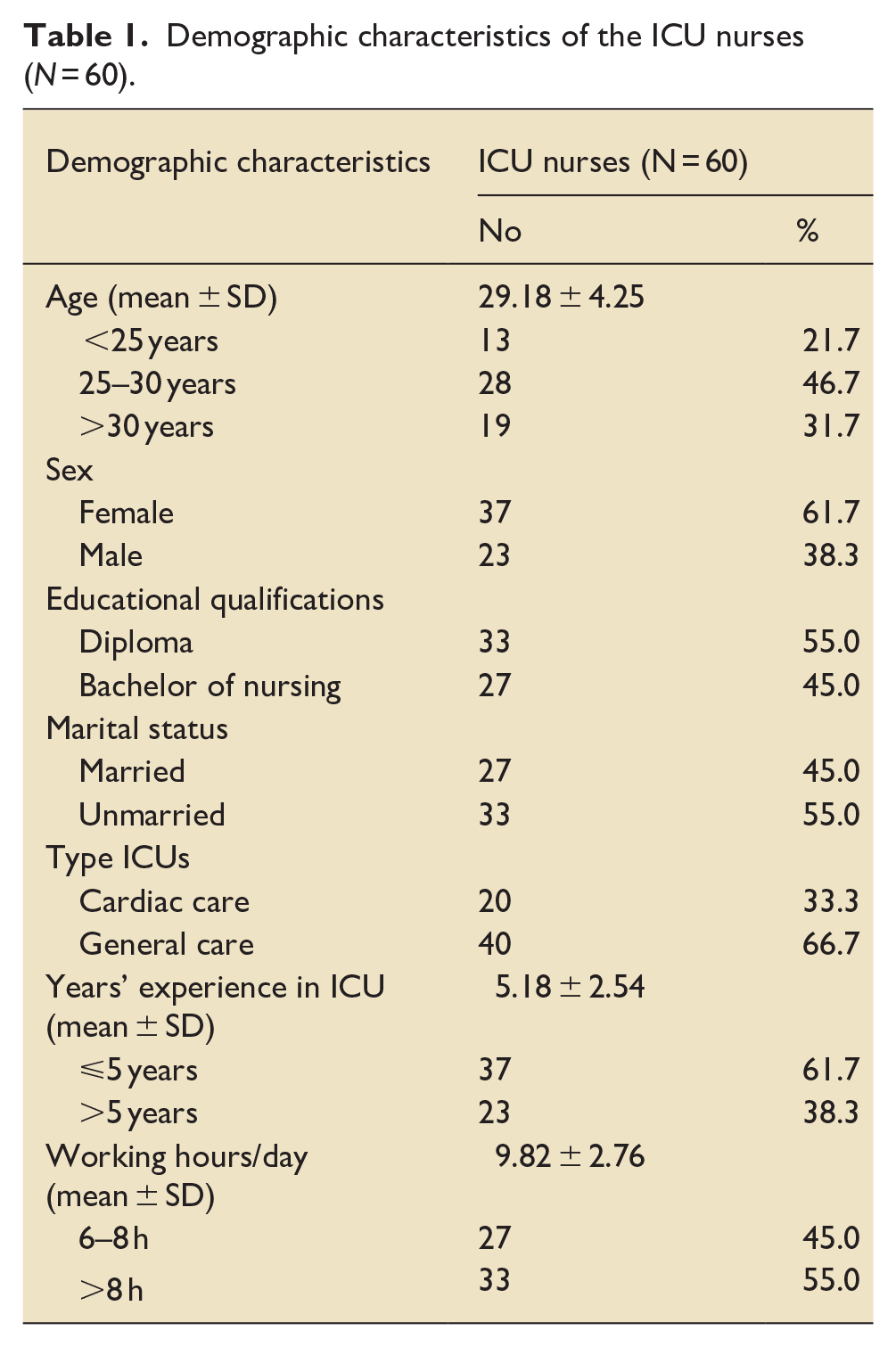
The mean age of CCNs was 29.2 ± 4.2 years, with the majority (46.7%) being in the 25–30 age group. Most CCNs were females (61.7%), and more than half were unmarried (55%) and had a nursing diploma (55%). Most of the nurses (66.7%) working in general care, 61.7% had 5 years of ICU experience or less, with a mean ICU experience of 5.2 ± 2.5 years. On the other hand, more than half of the nurses (55%) worked >8 h per day, with a mean working duration of 9.8 ± 2.8 h per day (Table 1).
Demographic characteristics of the ICU nurses (N = 60).
Impact of the psychoeducational and relaxation program on CCNs’ stress
The mean score of CCNs’ stress before the program was 60.48 ± 9.51, corresponding to a moderate stress level of 86.7%. However, the mean score of stress was significantly reduced to 30.98 ± 4.35 and was sustained at a mean score of 33.13 ± 5.31 3 months post-program, corresponding to a mild stress level (Figure 1).
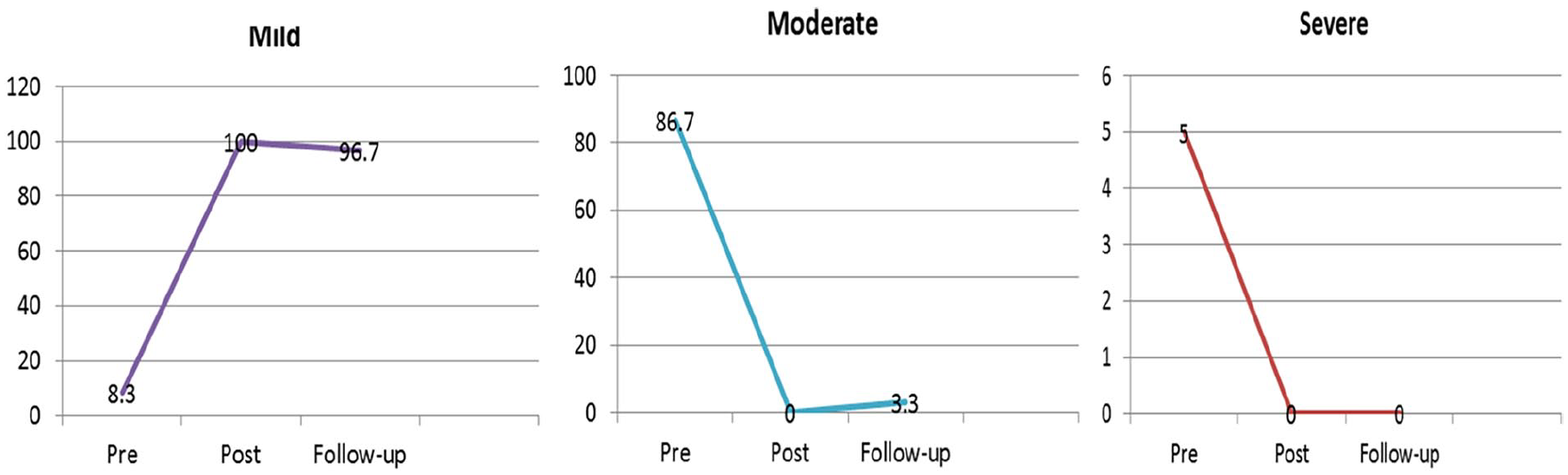
Comparison of levels of stress among CCNs about delirium at pre, post-implementation and follow up evaluation of the educational program (N = 60).
The highest mean score of CCNs’ stress related to caring for patients with delirium was observed before the program for all causes of stress on the DNSS, being 4.95 ± 1.77 for nursing environment, 9.37 ± 2.16 for relationships with peers, 14.40 ± 4.02 for knowledge about delirium, and 31.77 ± 5.78 for nursing practice and work (Table 2). However, the mean scores of stress related to all these causes showed a significant reduction after the program (2.85 ± 0.95, 4.70 ± 1.33, 7.20 ± 1.67, and 16.23 ± 2.80, respectively) and at the 3-month follow-up (3.15 ± 1.05, 4.95 ± 1.23, 7.67 ± 1.66, and 17.37 ± 3.57, respectively). On the other hand, the mean score of total stress for all DNSS items showed a significant reduction from 60.48 ± 9.51 before the program to 30.98 ± 4.35 after the program and 33.13 ± 5.31 at the 3-month follow-up (Table 2).
The average scores of nurses on the Delirium Nursing Stress Scale (DNSS) were measured before, after, and during follow-up evaluations of psychoeducational program (N = 60).
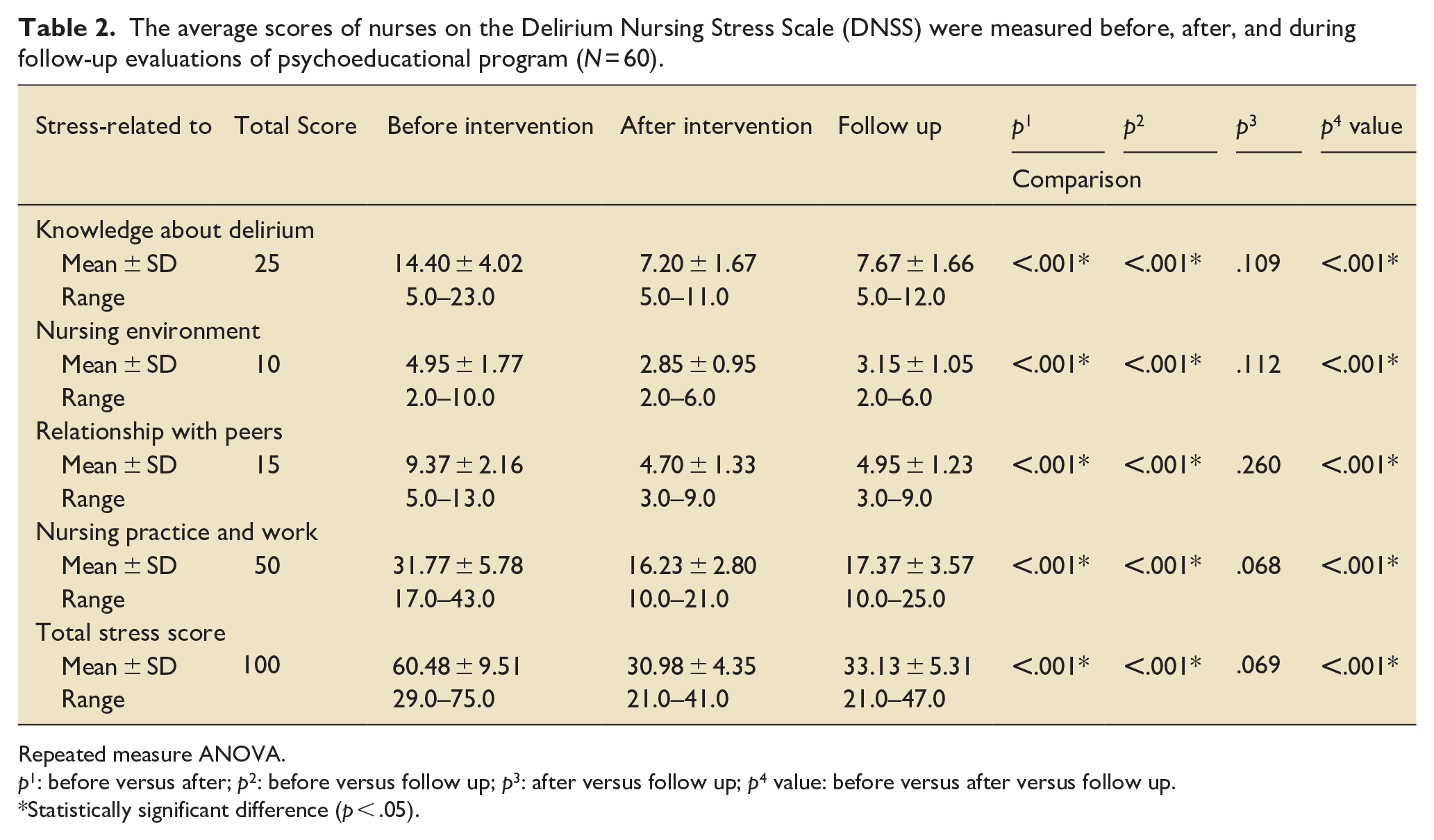
Repeated measure ANOVA.
p1: before versus after; p2: before versus follow up; p3: after versus follow up; p4 value: before versus after versus follow up.
Statistically significant difference (p < .05).
Comparison of mean scores of CCNs’ stress related to delirium according to demographic characteristics
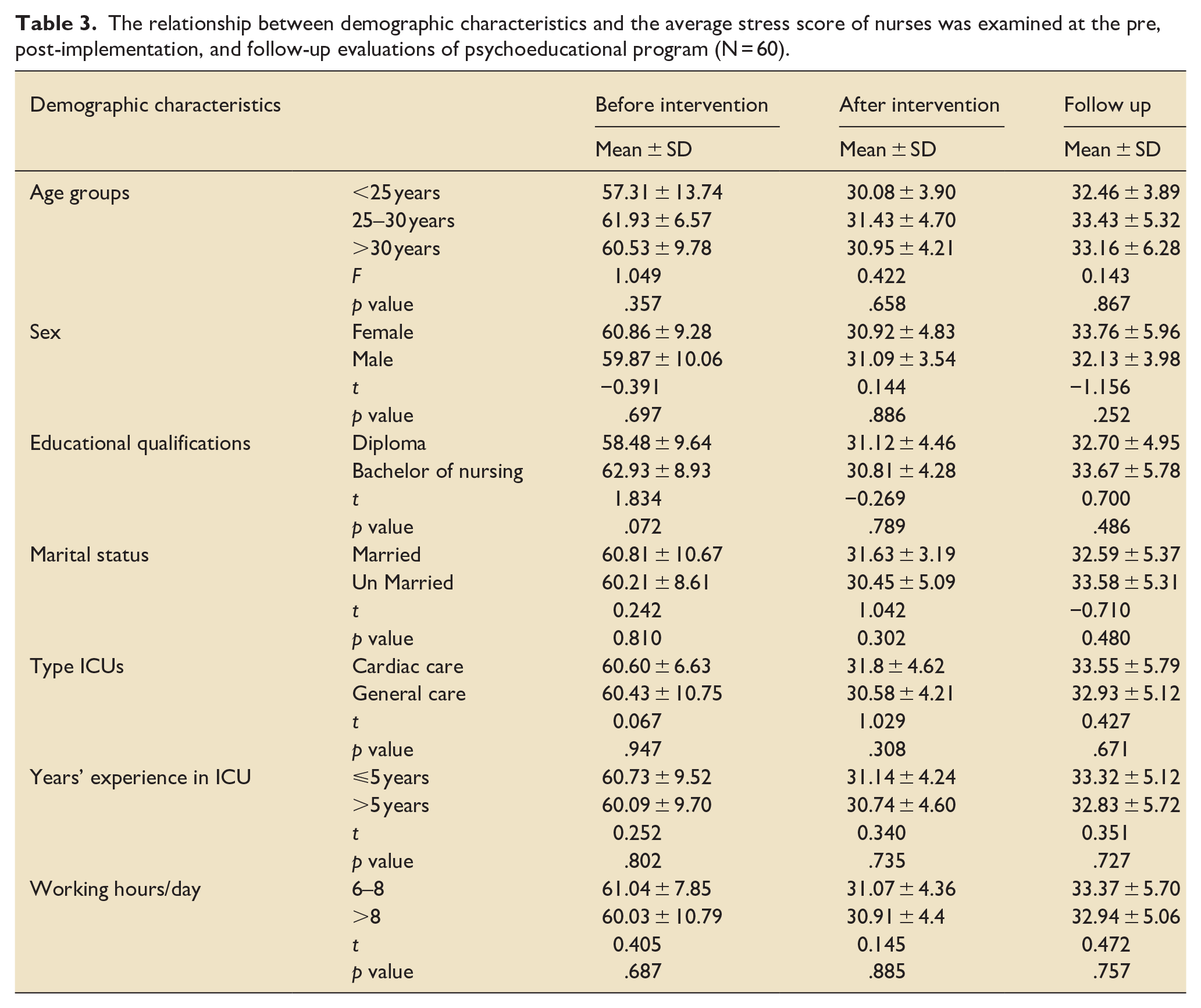
There were no statistically significant differences in the mean scores of CCNs’ stress before and after the program, or at the 3-month follow-up for any of the demographic characteristics (Table 3).
The relationship between demographic characteristics and the average stress score of nurses was examined at the pre, post-implementation, and follow-up evaluations of psychoeducational program (N = 60).
Discussion
The present study showed moderate stress in the majority of CCNs caring for patients with delirium in Taiz, as reflected by a high mean score of total stress before implementing a psychoeducational and relaxation program. This finding may be attributed to the need for self-protection felt by the majority of nurses and the perceived threat that dealing with delirious patients may jeopardize their personal safety. Nurses believe that delirious patients are entirely dependent on them because they often need more support to perform their daily activities due to their major physical and cognitive deficits. This finding is supported by several earlier studies,33 –37 showing that the majority of ICU nurses had moderate stress with high mean scores of total stress when caring for patients with delirium. Furthermore, the physical restraints of patients with delirium are mostly managed by nurses in various healthcare settings, adding to their stress. 38 The use of physical restraints was found to induce feelings of sadness and guilt in nurses. 39
The present study revealed high levels of stress experienced by the majority of CCNs prior to implementing the psychoeducational and relaxation program in terms of knowledge about delirium, nursing environment, relationship with peers, and nursing practice and work. These findings are consistent with those reported in previous studies conducted elsewhere,34,40 –44 which found significantly high mean scores of stress among CCNs caring for patients with delirium due to insufficient information on delirium prevention and management. In addition, there are several factors that may contribute to CCNs’ stress while caring for patients with delirium, including a lack of awareness of delirium causes, unfamiliarity with the delirium consequences and facing numerous barriers such as ICU regulations, quality of relationships at work, and end-of-life concerns in the ICU. The most common stress-related cause reported by CCNs caring for patients with delirium in the present study was the lack of appropriate screening tools in the ICU, followed by lack of contact with patients due to heavy workload, time-consuming use of delirium-screening techniques, and insufficient knowledge of delirium in the ICU.
The present study found delirium-related stress was significantly reduced from moderate to mild stress in the majority of CCNs following the psychoeducational and relaxation program. This finding indicates that increasing awareness of delirium and its management through psychoeducational and relaxation techniques can reduce stress levels in CCNs caring for patients with delirium. This finding is in agreement with that reported by Park and Gu, 37 who found that overall delirium-related stress became milder as reported by the majority of CCNs who participated in an educational program. It was found that higher knowledge and good practice of nurses in dealing with delirium significantly reduce their levels of stress.36,45 Therefore, it is possible to reduce the work stress of nurses by providing them with the necessary knowledge, practices, and stress management tools. Meanwhile, interactive E-learning has been shown to lower the mean scores of nurses’ delirium-related strain of care. The advantage of E-learning in lowering the strain of care may be attributed to its effectiveness in enhancing nurses’ capacity to detect and manage delirium. 46 Overall, the mild stress reported by all CCNs after the program in the present study should be interpreted with caution because they might have overestimated their stress levels during the initial assessment prior to the program. In order to address this issue, further studies involving interviews with nurses are needed. Furthermore, nursing school curricula should be regularly reviewed and modified to ensure that theoretical knowledge aligns with current hospital practices, including topics related to recognizing delirium, stress, and stress management techniques.
In the present study, immediate reductions in CCNs’ delirium-related stress on the key components of the DNSS tool after the program were sustained 3 months later at follow-up. Similarly, a study among CCNs in Korea reported a significant reduction in delirium-related stress for these key components after receiving a psychoeducational program. 37 The less stressful work with delirious patients observed after the program in the present study may be due to standardized basic knowledge, effective communication of nurses when dealing with delirious patients, and improved communication of nurses with relatives of the patients. Moreover, improvement of knowledge can increase nurses’ self-confidence and ability to deal with emergency situations.
The present study did not find a statistically significant association between delirium-related stress and any of the demographic characteristics of CCNs, either before or after the program, or at the 3-month follow-up. This finding is in the line with that by Kim and Eun, 47 who found no significant association between the demographic characteristics of CCNs and average delirium-related stress. Likewise, Suh and Yoo 33 found no significant association between CCNs’ demographic characteristics and average stress, except for a statistically significant association with their age and level of education. Younger nurses are more likely to assume more job obligations and feel underprepared. They are thus subject to pressure and stress in the workplace, which may result in uncontrollable feelings of dissatisfaction.
The present study has some limitations as it was conducted in a single hospital. However, the present psychoeducational and relaxation program was the first to address the training gap among CCNs in Taiz city so as to reduce their delirium-related stress. Importantly, there was a remarkable lack of knowledge and skills to care for patients with delirium among CCNs in the city, particularly with deteriorated healthcare services and health systems as a result of the country’s armed conflicts. Although the present findings cannot be generalized to the critical care of patients with delirium in the whole country, the developed program may still have benefits in educating and training CCNs in the care and management of delirious patients. Another limitation might be introduced by measuring stress based on a self-report tool. Therefore, further studies are required to address this self-assessment issue and explore the program’s sustainability and potential for development of the program.
Conclusion
There is a positive impact of psychoeducational and relaxation program on reducing the stress levels in CCNs caring for patients with delirium in the ICUs in Taiz city, improve the standard of care provided to these patients. Demographic characteristics of CCNs have no association with the levels of stress before or after the program, either immediately or 3 months later. It is recommended that CCNs be regularly assessed for delirium-related stress and educated to acquire knowledge and skills necessary to reduce this stress when caring for delirious patients.
Supplemental Material
sj-doc-1-inc-10.1177_17511437241275307 – Supplemental material for Effect of psychoeducational program and relaxation training on critical care nurses’ stress regarding care of patients with delirium
Supplemental material, sj-doc-1-inc-10.1177_17511437241275307 for Effect of psychoeducational program and relaxation training on critical care nurses’ stress regarding care of patients with delirium by Saleh O Abdullah, Alaa El Din M Darweesh, Naglaa A Mohammed, Sameer A Alkubati and Awatif M Alrasheeday in Journal of the Intensive Care Society
Footnotes
Acknowledgements
Grateful acknowledgment to every nursing staff working at Intensive Care Units in the Al-Thawra Hospital.
List of abbreviations
CCNs: Critical Care Nurses, ICU: Intensive Care Unit, DNSS: Delirium Nursing Stress Scale
Authors contributions
Saleh Abdullah designed the study; Saleh Abdullah conducted the survey and data collection; Alaa El Din M Darweesh analyzed the data; Alaa El Din M Darweesh and Sameer A Alkubati interpreted the results. Saleh O Abdullah, Alaa El Din M Darweesh, Naglaa A Mohammed, Sameer A Alkubati, and Awatif M Alrasheeday wrote the first draft of the paper and contributed to the revision of the whole paper. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
The data presented in this study are available on request from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.