
Abstract
Specialist weaning units (SWUs) aim to liberate patients with complex weaning failure from mechanical ventilation and facilitate their discharge from the ICU. This retrospective service evaluation reports the outcomes of a SWU at Wythenshawe Hospital, Manchester between 2017 and 2019. In total, 75.0% (n = 33/44) of patients survived to hospital discharge. Of these patients, 72.7% (n = 24/33) were self-ventilating. Overall, 1-year survival was 68.2% (n = 30/44), whilst 5-year survival was 52.3% (n = 23/44). Whilst this study is relatively small, these findings are encouraging and further support the case for SWUs.
Keywords
Introduction
Weaning the ventilatory support for patients receiving invasive mechanical ventilation presents a challenge in a subset of patients admitted to the Intensive Care Unit (ICU). 1 Specialist Weaning Units (SWUs) are evolving with the aim of liberating these patients from mechanical ventilation and facilitating their discharge. 2 This retrospective service evaluation reports the outcomes of a tertiary SWU in the North West of England. The SWU occupies two beds in the long-term ventilation ward. Patients are admitted via the general ICU before being stepped down to the long-term ventilation ward, which houses the regional complex ventilation service (including domiciliary tracheostomy ventilation). The SWU is staffed by four consultants with wider MDT input from the complex ventilation service.
Methods
Data were retrospectively collected from patients treated by the SWU at Wythenshawe Hospital, Manchester University NHS Foundation Trust, between February 2017 and December 2019. Patients from the general ICU in Wythenshawe Hospital were excluded from analysis. Data obtained from electronic and paper medical records were anonymised. Admission diagnoses and reason for weaning failure were categorised according to Table 1. Where multiple reasons for weaning failure were identified, these were recorded. Weaning outcome at discharge were categorised as: (1) self-ventilating, (2) nocturnal non-invasive ventilation (NIV), (3) over 16 h NIV per day, (4) long-term tracheostomy ventilation, (5) died prior to discharge. Kaplan-Meier curves were generated using GraphPad Prism version 9.5.1 for Windows, GraphPad Software, www.graphpad.com.
Demographics, admission diagnosis and reason for weaning failure.
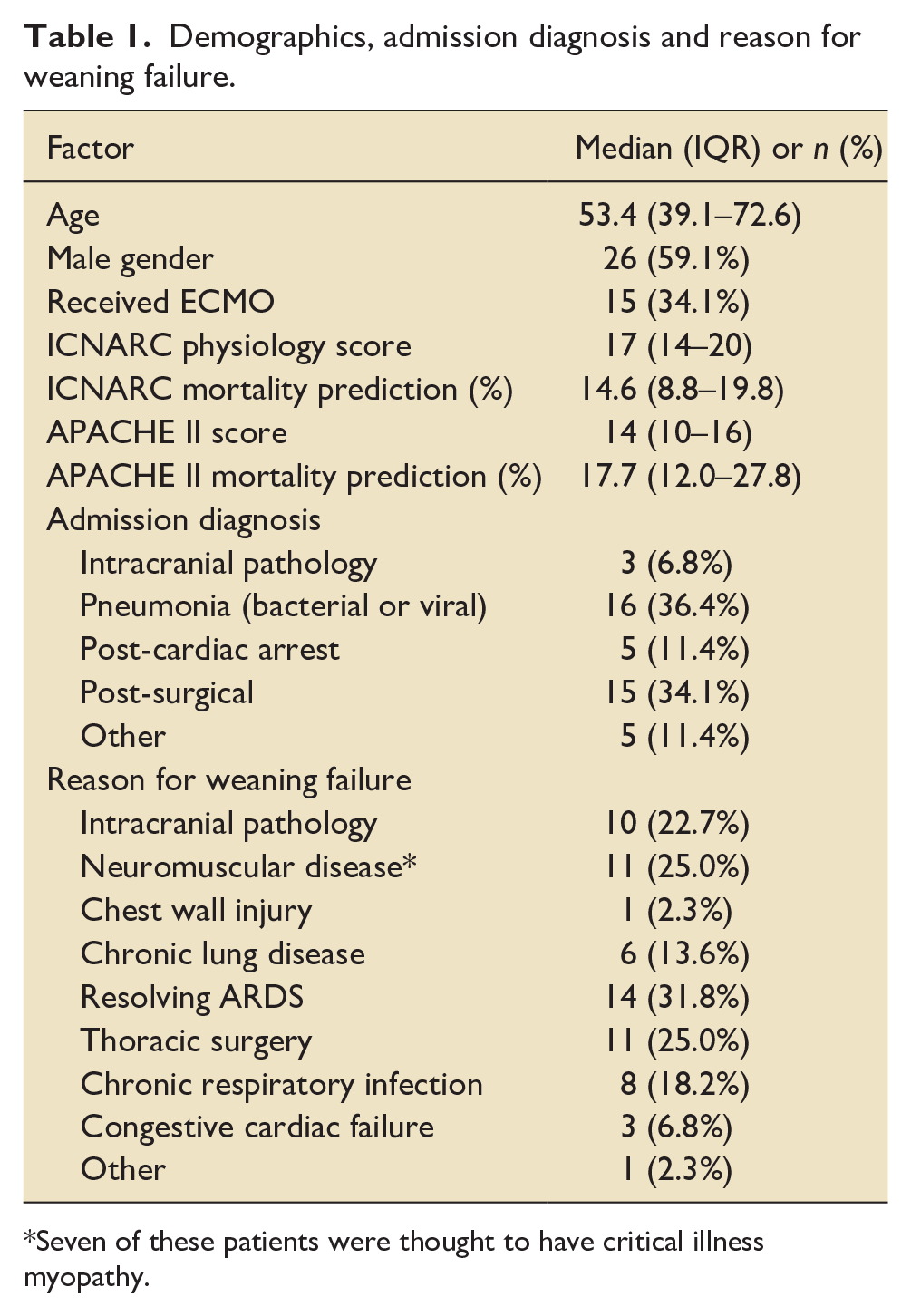
Seven of these patients were thought to have critical illness myopathy.
Results
During the study period, 44 patients received care from the SWU. Demographics, admission diagnosis and reason for weaning failure are reported in Table 1. All patients were tracheostomy ventilated 24 h per day on arrival to the SWU. The median duration of critical care stay prior to input from the SWU was 30 days (IQR = 12–53). The median duration of total critical care stay was 56 days (IQR = 39–101). The median time from SWU input to discharge or death was 45 days (IQR = 28–83). Excluding patients who were already cuff-down for 24 h at the time of referral (2%, n = 1) or who never achieved 24 h cuff-down (11%, n = 5), the median time from SWU input to 24 h cuff deflation was 17 days (IQR = 7–24). At the time of hospital discharge, 61% of patients (n = 27) were established on a normal oral diet. The median time from SWU input to establishing normal oral diet was 24 days (IQR = 20–35).
Follow up data was available for all patients except for 5-year follow up with data censored in 17 participants. In total, 33/44 (75%) of patients survived to hospital discharge: 20/44 (45%) of patients were discharged home, 7/44 (16%) were discharged to a rehabilitation facility and 6/44 (14%) were transferred to another hospital. At the time of hospital discharge, 24/44 (55%) of patients were self-ventilating, 7/44 (16%) required nocturnal NIV, 2/44 (5%) required >16 h per day of NIV and none required long-term tracheostomy ventilation. Overall, 1-year survival was 68% (n = 30/44), whilst 5-year survival was 52% (n = 23/44; Figure 1).
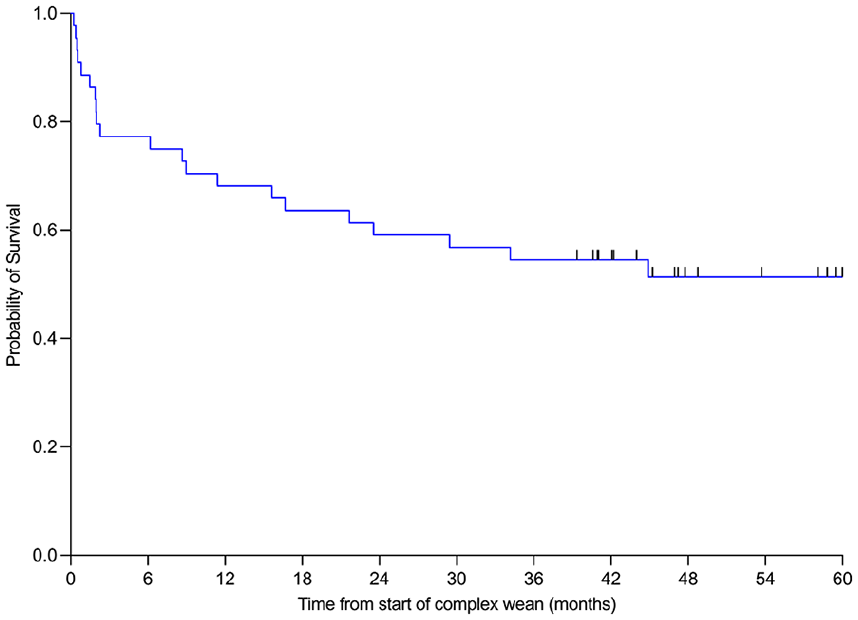
Five-year Kaplan-Meier survival curve for all patients referred to the complex weaning service; n = 44. I = censored observation (n = 17).
Discussion
In the present study, weaning failure was multi-factorial with the three leading contributors to weaning failure being neuromuscular disease (including critical illness myopathy), resolving acute respiratory distress syndrome and thoracic surgery.
Survival to hospital discharge was high at 75% and similar to that observed for all patients admitted to ICU nationally. 3 The majority of these patients were discharged home. Mortality data presented here are better than those from international meta-analysis of studies on prolonged mechanical ventilation 4 and equivalent to other UK SWUs where 1-year and 5-year overall survival has been found to be 65% and 29% respectively. 5 A degree of selection bias must be considered as patients who were considered impossible to wean or died awaiting transfer of care were not included in the current study.
A large proportion of patients were liberated from on-going ventilatory support at hospital discharge. Of patients who survived to hospital discharge, 73% required no on-going ventilatory support. Accepting differences in case-mix, the results presented here are comparable with those observed in studies from other UK SWUs.5,6
Over the 34-month data collection period, the SWU treated on average 1.3 patients per month with a median length of stay on the SWU of 45 days. This equates to approximately 700 bed days or two ICU beds per year. These data support the need to expand the capacity of our weaning service to maintain patient flow.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.