
Abstract
Introduction
This study investigated invasive mechanical ventilation modalities used in severe blunt chest trauma patients with pulmonary contusion. Occurrence, risk factors, and outcomes of early onset acute respiratory distress syndrome were also evaluated.
Methods
We performed a retrospective multicenter observational study including 115 adult patients hospitalized in six level 1 trauma intensive care units between April and September of 2014. Independent predictors of early onset acute respiratory distress syndrome were determined by multiple logistic regression analysis based on clinical characteristics and initial management.
Results
Protective ventilation principles were highly implemented, even prophylactically before acute respiratory distress syndrome occurrence. Early onset acute respiratory distress syndrome appeared to be associated with lung contusion of >20% of total lung volume and early onset pneumonia.
Conclusions
Predictors of early onset acute respiratory distress syndrome could help with identifying high-risk populations, potentially improving case management through specific protocol development for these patients.
Keywords
Introduction
Lung contusion, commonly caused by a high-kinetic energy chest wall impact, is the most frequently diagnosed intrathoracic injury resulting from blunt trauma. 1 It occurs in 27% of severe trauma cases having with an injury severity score (ISS) of 15 or greater. 1 Importantly, lung contusion represents an independent risk factor for pneumonia and acute respiratory distress syndrome (ARDS),2,3 and significantly worsens prognosis in major trauma patients. 4 Pulmonary contusion is also associated with greater likelihood of requiring ventilatory support, and patients admitted to the intensive care unit (ICU) with severe chest trauma and pulmonary contusion-induced hypoxemia commonly require invasive mechanical ventilation (IMV). 5
Among patients with chest trauma, intubation rates range from 23 to 75%, mainly depending on trauma severity, associated injuries such as haemorrhagic shock or traumatic brain injury, presence of underlying pulmonary disease, and intensity of ICU management.1,6 IMV improves oxygenation but can lead to ventilator-induced lung injury (VILI). 7 IMV can potentially represent a ‘second hit’ for a contused lung, aggravating initial lung damage and worsening the oxygenation. Lung-protective mechanical ventilation (LPMV), based predominantly on lower tidal volume between 6 and 8 mL/kg of predicted body weight (PBW) and positive end-expiratory pressure (PEEP) optimization, has well-established benefits both in the ICU for ARDS patients8,9 and in anaesthesia for major surgical procedures.7,10,11 However, the clinical influence of LPMV has not yet been clearly evaluated in blunt chest trauma, and little is known about guideline compliance in real-life clinical practice.
Here, we performed a retrospective multicentre evaluation of practices, specifically with regards to the IMV strategies used in French ICUs for patients with severe blunt chest trauma and pulmonary contusion. The primary objective was to characterize the ventilation strategies and associated therapeutics. As a secondary objective, we evaluated the occurrence of early onset ARDS, and its incidence, risk factors and outcomes.
Patients and methods
Study design
We performed a retrospective multicentre observational study including ICU patients with blunt chest trauma and pulmonary contusion who were hospitalized between April and September of 2014 in six level 1 trauma centres, including the university hospitals of Marseille, Lyon and Grenoble and the military teaching hospitals of Toulon, Clamart and Marseille. Eligibility criteria for inclusion were as follows: severe blunt chest trauma, with an ISS of >15, and a thorax abbreviated injury score (AIS) ≥ 3; 12 pulmonary contusion of ≥ 10% of the total lung volume, documented by admission computed tomographic scan; need for tracheal intubation and mechanical ventilation for at least the first 48 h post-trauma; and age over 18 years. Patients who died during the first 48 h after trauma were excluded. Data were extracted from existing trauma registries and from medical records of the selected institutions, and were then anonymously registered into a self-administered online survey. Participating hospitals entered their own data into the survey. The protocol of this study was approved by the ethics committee for research (CERAR) of the French society of anaesthesia and intensive care (SFAR) with the certificate of approval number IRB-00010254-2016-121, and by the French national commission on informatics and liberty (CNIL) with the certificate of approval number 1995626v0. It waived the requirement to obtain informed consent from the patient or patient's kin due to the observational and retrospective nature of the study.
Data recording
We collected the following data: demographics, trauma characteristics and early management, ventilation modalities from days 1 to 5, occurrence of early onset ARDS (within five days after admission), occurrence of early onset pneumonia (EOP; between days 1 and 3) or late-onset pneumonia (from day 4), ARDS characteristics and management and patient outcome. ARDS was defined using the Berlin definition,
13
with three categories based on degree of hypoxemia: mild (200 mm Hg < PaO2/FIO2 ≤ 300 mm Hg), moderate (100 mm Hg < PaO2/FIO2 ≤ 200 mmHg) and severe (PaO2/FIO2 ≤ 100 mmHg). Pneumonia was defined by the presence of at least two of the three following findings
3
:
(1) body temperature of ≥ 38℃ or < 36℃, with white blood cell count of >12 × 109 or < 4 × 109, and with the presence of purulent tracheobronchial secretions; (2) new or changing infiltrate on chest radiograph within 72 h after admission; (3) confirmation by fibreoptic bronchoscopy with bronchoalveolar lavage (BAL) and quantitative culture (>105 colony-forming units/mL).
End-points
The primary end-point of this study was to describe characteristics related to trauma and trauma-management, with particular focus on the invasive ventilation modalities used during the first two days post-trauma (tidal volumes, PEEP levels and FiO2). Patients with tidal volumes over 8 mL/kg PBW were classified as ‘non-adherent’ to LPMV principles.
The secondary end-point focused on early onset ARDS, including its management and outcome. Multiple logistic regression analysis was used to determine independent predictors of early onset ARDS based on clinical characteristics and initial management.
Statistical analysis
Statistical analyses were performed using SPSS version 20.0 (SPSS Inc., Chicago, IL, USA), and data distributions were checked for normal distribution. Nominal variables are presented as number (%), while continuous variables are presented as mean ±standard deviation (SD), or as median (quartile 0.25–quartile 0.75) when normal distribution was excluded. Continuous variables were compared using the Student's t test or the Wilcoxon-Mann-Whitney rank test when normal distribution was excluded. For comparisons of discrete variables, we used the χ2 test or Fisher's exact test, as appropriate. To identify the continuous and categorical variables contributing to the development of early onset ARDS (dependent variable), we performed multivariate analyses using a logistic regression model to determine the odds ratio and 95% confidence interval. Variables that were significantly associated in univariate analysis (P value < 0.20) were entered into the model and retained through forward selection (P < 0.05). Since some variables may be surrogate markers of others, we carefully appraised the selected variables to prevent colinearity. To assess the calibration of the logistic model, we used the Hosmer-Lemeshow goodness-of-fit test to evaluate the discrepancy between observed and expected values. For all tests, P < 0.05 was considered to indicate statistical significance.
Results
Patient and trauma characteristics
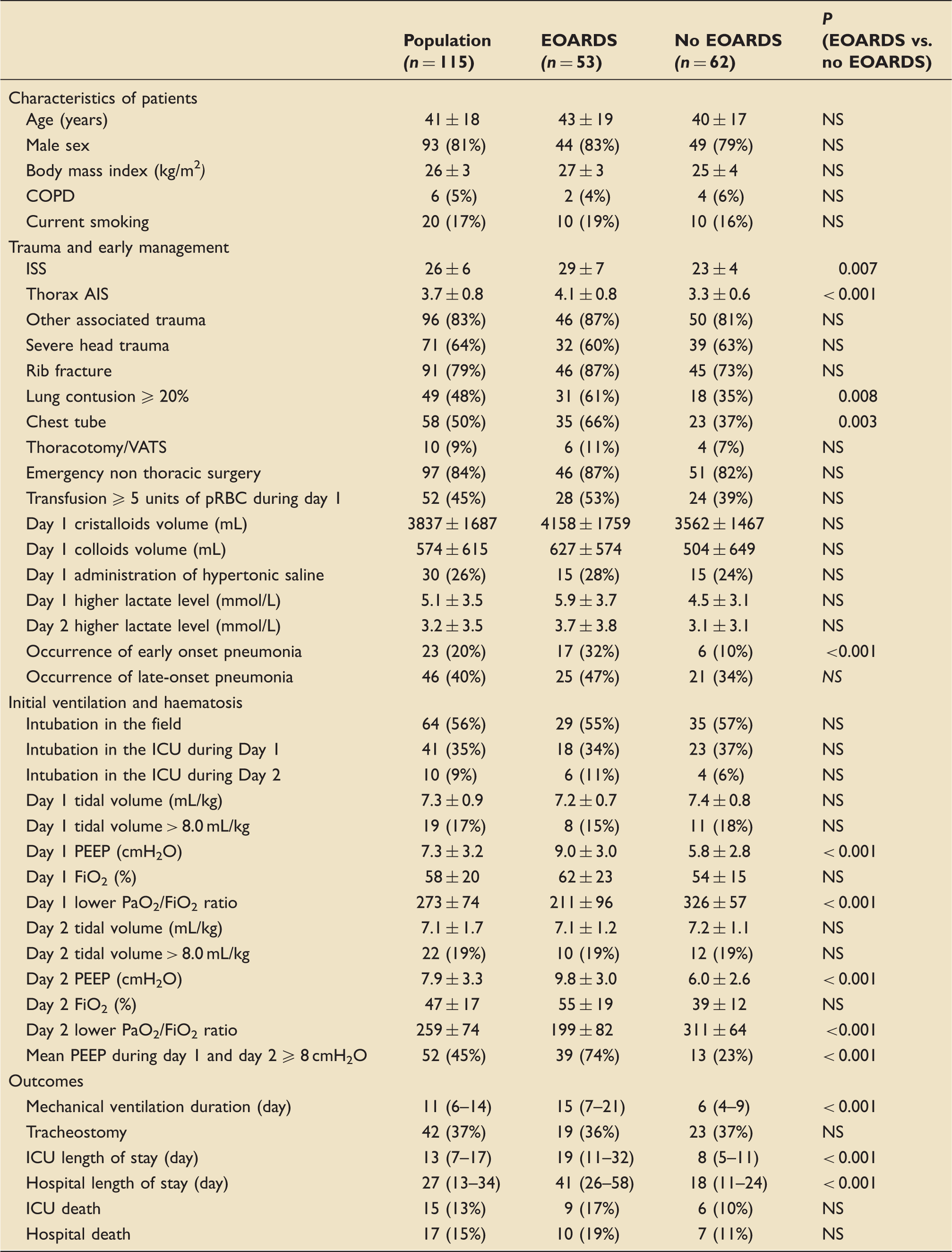
During the study period, 147 severely injured patients were admitted with severe blunt chest trauma, 115 of them met the inclusion criteria (Figure 1). Table 1 reports the main characteristics of the overall study population, trauma characteristics, early management and outcomes. The patient population was 81% males, with an average age of 41 ± 18 years. The mean ISS was 26 ± 6, and mean thorax AIS was 3.7 ± 0.8. Most were polytrauma patients (83%). In 49 (48%) patients, the contused lung volume was >20% of the total lung volume, and 58 (50%) patients had haemothorax and/or pneumothorax requiring chest tube insertion. EOP was diagnosed in 23 (20%) patients, and late-onset pneumonia in 46 (40%) cases.
Flow diagram of the study. Characteristics of patients with or without early onset ARDS.
a
AIS: abbreviated injury score; ARDS: acute respiratory distress syndrome; COPD: chronic obstructive pulmonary disease; EOARDS: early onset acute respiratory distress syndrome; FiO2: fraction of inspired oxygen; ICU: intensive care unit; IQR: interquartile range; ISS: injury severity score; NS: not significant; PEEP: positive end expiratory pressure; pRBC: packed red blood cells; SD: standard deviation; VATS: video-assisted thoracoscopic surgery. Day 1 and Day 2 denote the first and second days after trauma, respectively. Data are presented as number (%), mean ± SD, or median (IQR: 25th–75th percentile). Statistical significance was accepted at P < 0.05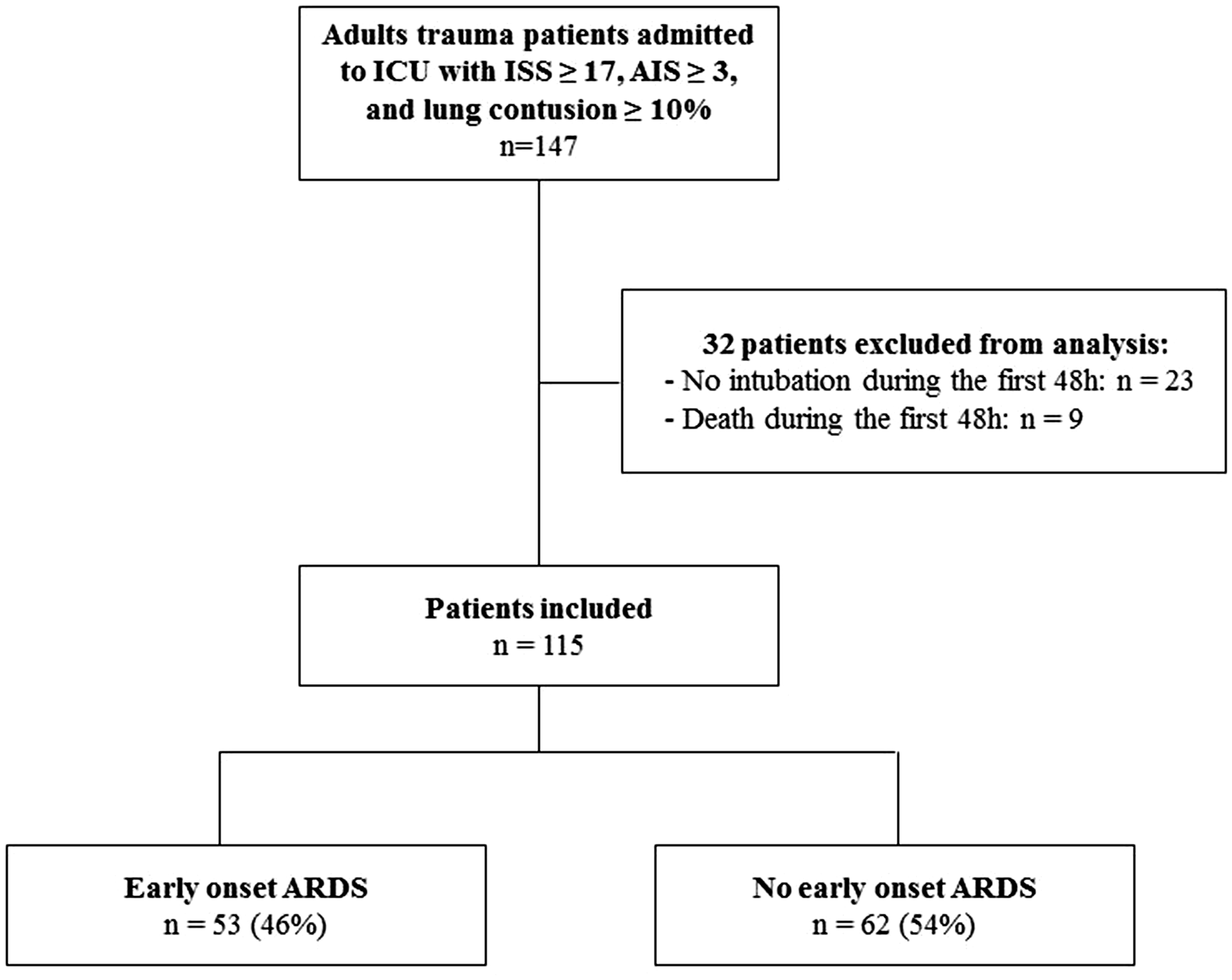
Patterns of mechanical ventilation during the first two days
A total of 64 (56%) patients underwent tracheal intubation in the field, 41 (35%) were intubated during their first day in the ICU, and 10 (9%) were intubated during their second day in the ICU. Table 1 reports mean tidal volume, number of patients with tidal volumes over 8 mL/kg PBW, mean PEEP and mean FiO2 during the first two days.
Early onset ARDS
ARDS characteristics. a
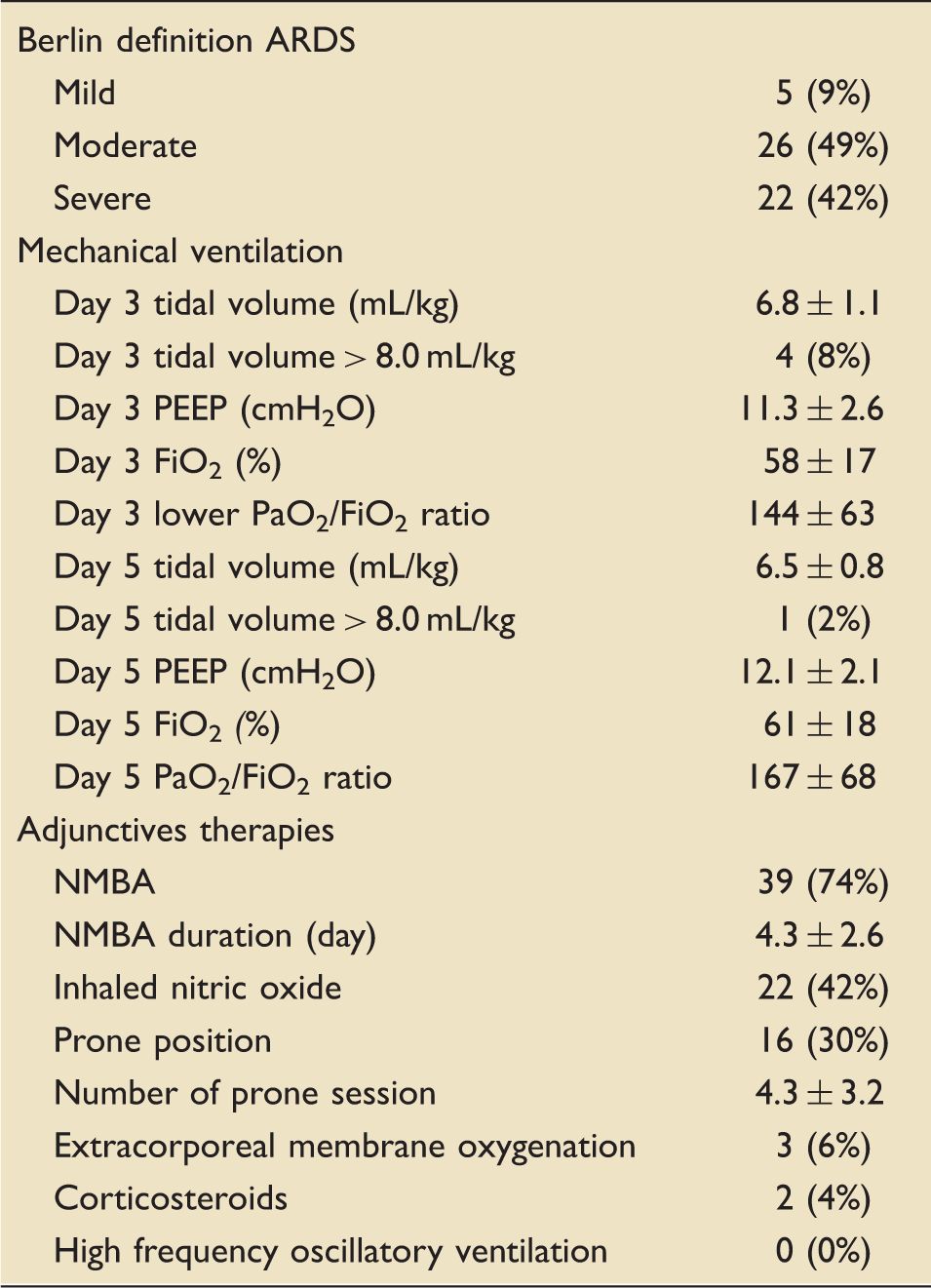
ARDS: acute respiratory distress syndrome; FiO2: fraction of inspired oxygen; ICU: intensive care unit; NMBA: neuromuscular blocking agent; PEEP: positive end-expiratory pressure; SD: standard deviation.
Data are presented as number (%) or mean ± SD.
Risk factors of early onset ARDS
Results of multivariate analysis of the independent risk factors for early onset ARDS.
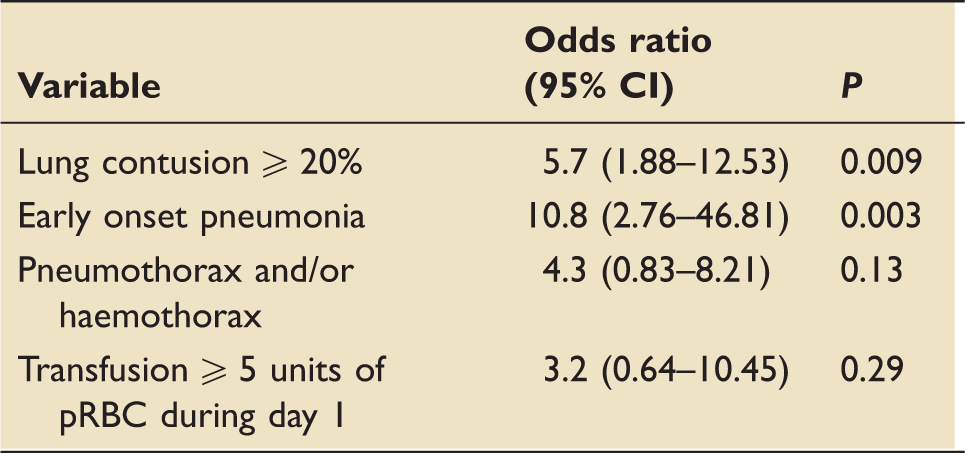
ARDS: acute respiratory distress syndrome; CI: confidence interval.
Discussion
In patients with severe chest trauma, acute respiratory failure is frequent and multifactorial, mainly involving pulmonary contusions, pleural effusions, and parietal injuries with alterations of respiratory mechanics and pain-induced hypoventilation. Tracheal intubation and IMV can be indicated after noninvasive ventilation failure, 14 or as first-line therapy due to hypoxemia severity or associated injuries.
Invasive ventilation of contused lung
In the setting of chest trauma, IMV could constitute a theoretical two-hit model that may potentiate initial alveolar damage and a post-traumatic inflammatory response. The nonhomogeneous character of contused lung makes ventilation challenging, and injured lungs are particularly vulnerable to VILI. 1 Non-protective ventilator settings – especially high tidal volume (>10–12 mL/kg PBW), very low PEEP (<5 cmH2O), or no PEEP – may cause alveolar overdistension and repetitive tidal recruitment, leading to alveolar damage with interstitial oedema through alveolo-capillary membrane destruction. 15 In ARDS, mechanical ventilation induces stress and strain on lung parenchyma, promoting a lung inflammatory response that compounds the initial lesions. 16 LPMV is based on lower tidal volume and PEEP optimization, with the aim of avoiding VILI occurrence. Cornerstone of ARDS management, LPMV is now considered a routine strategy for ventilation of patients even without ARDS, particularly since a meta-analysis showed that low tidal volumes were associated with better clinical outcome in a population without ARDS. 17 This concept has been gradually extended to the operating room environment, with LPMV used for healthy lung ventilation during anaesthesia, where it can reduce postoperative pulmonary complications.7,10,11,18
Our present study in a retrospective cohort represents the first evaluation of practices with regards to IMV parameters used in trauma ICUs in France. The obtained results reveal a high rate of compliance with the lung protective tidal volume criteria, including less than 20% of ‘non-adherent’ patients. It appears that intensivists prophylactically apply the LPMV recommendations with relative homogeneity within this specific population of severe chest trauma patients. Over the first two days post-trauma, the mean tidal volumes ranged from 7.3 to 7.2 mL/kg of PBW, and PEEP levels from 7.3 to 7.9 cmH2O. These data contrast with previous findings regarding compliance with clinical guidelines in a one-day audit at 66 French adult ICUs in 2009. 19 Indeed, that study found poor compliance of only 37% with the recommended ventilator setting in ARDS. The presently determined trend towards progressive improvement is likely to be a global phenomenon.
Early onset ARDS
As a secondary objective, our present study aimed to identify risk factors for early-onset ARDS and to describe ARDS management and outcome among patients with mechanically ventilated severe thoracic trauma. In 2016, trauma was identified as constituting at least 4.2% of cases in the general population of patients with ARDS. 20 In our present cohort, 46% of patients developed early onset ARDS within the first five days after admission. Early onset ARDS was independently associated with two variables: lung contusion of > 20% total lung volume and EOP. These both factors had been previously identified as having predictive value.2,3,21–23
Contused lung volume on initial CT scan
Measuring contusion volume at admission enables an accurate early estimation of risk for subsequent ARDS development. Contusion volume is the first available parameter during patient management, and its predictive value has been identified in previous studies.2,21–23 Indeed, the percentage of contused lung volume evaluated at initial CT scanning is a major factor in determining the need for IMV, 21 and is the best predictor of severe respiratory failure. 22 At a contused volume of over 202 or 21.5%, 22 the risk of ARDS development significantly increases, with a predictive value of 82%. The presence of a contusion volume exceeding 20% is also correlated with increases in the length of stay in the ICU, mechanical ventilation duration and risk of pneumonia development. 23
Early onset pneumonia
Here, we reported a 20% EOP incidence during the first 72 h after admission, which was in accordance with previous results. 3 Michelet et al. demonstrated that EOP was associated with prolonged mechanical ventilation duration, longer length of ICU stay and late mortality. 3
Early onset ARDS management and outcomes
We found that protective ventilation settings were prophylactically applied in the early post-traumatic stage, as well as used during ARDS treatment. A 2012 review of ARDS occurrence among injured patients concluded that lung protective ventilation was the most beneficial therapy. 24 Bellani et al. recently published an international multicentre study of patterns of care in an ICU population of 2377 ARDS patients, including 557 patients categorized as having severe ARDS. 20 They reported the following rates of adjunctive therapies in the ‘all ARDS’ and ‘severe ARDS’ groups, respectively: neuromuscular blocking agents (NMBA) (22 and 38%), prone positioning (8 and 16%), inhaled vasodilators (8 and 13%), ECMO (3 and 7%), high frequency oscillatory ventilation (1 and 2%) and high-dose corticosteroids (18 and 23%). In our present cohort, the preferred adjunctive therapies were as follows: NMBA (74% of patients), inhaled nitric oxide (42%), prone positioning (30%), ECMO (6%) and corticosteroids (4%). These high utilization rates indicated aggressive patterns of ARDS care. The more frequent use of inhaled nitric oxide compared to prone positioning could be related to the presence of associated injuries, such as brain or spinal injuries, which could prohibit any postural manoeuvres.
Limitations
This observational cohort was recruited from only six level 1 trauma ICUs, and likely does not reflect the practice of all ICUs in the country. Despite being a multicentre study, the population was fairly small, limiting the power of our results. Moreover, because of participating hospitals entered their own data into the survey, this may explain potential weaknesses in data entry and the apparent strong adherence to LPMV. The design does not allow us to establish conclusions regarding the benefits of any type of ventilator modality. Additionally, although our focus was on patients with severe chest trauma, many included patients exhibited multiple traumas, implying the presence of others' injuries. It is difficult to determine the mechanisms of ARDS occurrence, and the specific contribution of the lung contusion, in a multiple trauma population with several confounding factors. Lastly, diagnose a pneumonia is difficult in this context, given that several of the used criteria will be generated by trauma even in the absence of infection.
Conclusions
In trauma care, it remains a challenge to provide optimal ventilation in cases of severe blunt chest trauma with lung contusion. The present evaluation of practices with regards to IMV strategies observed a high rate of implementation of protective ventilation recommendations, even prophylactically before ARDS occurrence. Early onset ARDS appeared to be associated with a lung contusion of >20% of the total lung volume and EOP. Identifying high-risk populations could lead to improved case management through the development of specific protocol for such patients.
Footnotes
Abbreviations
abbreviated injury score acute respiratory distress syndrome confidence interval chronic obstructive pulmonary disease extracorporeal membrane oxygenation early onset acute respiratory distress syndrome early onset pneumonia inspired oxygen fraction high frequency oscillatory ventilation intensive care unit invasive mechanical ventilation injury severity score lung-protective mechanical ventilation non-invasive ventilation neuromuscular blocking agents not significant odds ratio positive end-expiratory pressure predicted body weight standard deviation ventilator-induced lung injury
Acknowledgements
The authors deeply thank Dr A. Loundou for statistical analysis (Department of Public Health, Medicine School University, Marseille, France).