
Abstract
Background
Delirium is a common complication in patients treated in the intensive care unit (ICU). Family members can help alleviate patient anxiety and may be able to aid in the management of delirium. This study aimed to explore the perceptions of former ICU patients and their families together, regarding the involvement of family in delirium management.
Method
Nine audio-recorded, semi-structured interviews took place with former ICU patients together with a family member. Participants were interviewed after their intensive care follow-up clinic appointment in an East Midlands hospital in England. Interviews were transcribed, coded and analysed using thematic analysis.
Results
Three themes were identified: ‘understanding about delirium’; ‘influencers of delirium management: family and healthcare professionals’ and ‘family-based delirium care’. Participants expressed that family have a valuable role to play in the management of delirium in the ICU. However, education and guidance is needed to support the family in how delirium can be managed and the current treatment options available. It is important for ICU staff to gain an understanding of the patient’s life and personality to personalise delirium management to the needs of the patient and their family.
Conclusion
This study found that family presence and knowledge about the patient may be beneficial to delirium management in the ICU. Further research should investigate the effectiveness of the strategies and interventions to understand their influence on delirium management in ICU patients.
Introduction
Delirium is a neuropsychological syndrome that is a form of acute brain dysfunction, 1 affecting up to 75% of intensive care unit (ICU) patients. 2 Delirium is associated with higher mortality in hospital with increased duration of mechanical ventilation, and impaired recovery and rehabilitation. 3 Moreover, delirium is associated with accelerating cognitive decline, as well as long-term functional and neuropsychological deficits.4,5
Non-pharmacological treatment options in the literature and guidelines include the use of environmental controls such as pain management, avoidance of sleep deprivation and early mobilisation. 6 In the ICU setting, avoiding low oxygen level, low blood pressure and low glucose level can help treat delirium. 7
The importance of encouraging involvement of carers, facilitating on-going engagement and support is highlighted throughout guidelines and the literature.7–9 The PAD’s guidelines highlight that there is inadequate evidence regarding the role that families play in reducing the stress of critically ill patients and facilitating non-pharmacologic interventions to manage delirium. 10 Eghbali-Babadi et al. 11 suggest that family members who know a patient well can help in the management of delirium and provide a feeling of safety when the patient is in an unfamiliar environment. 11 Paulson et al. 12 suggest family members are an underused, valuable resource to care, and more research into the techniques to manage delirium is warranted. 12
In the current literature, there is a large focus upon delirium prevention but less on investigating the management of ICU delirium. A recent meta-analysis 13 found in analysis of twenty-six studies exploring incidence and duration of delirium that family participation resulted in a reduced incidence of delirium. They found that family involvement may play a role in altering the course of delirium; however, they suggest that further research and understanding is required into the mechanisms that influence delirium. 13 On the contrary, a pilot study investigating delirium management, through family mentoring to develop a sense of self-efficacy to intervene in delirium management, found no statistically significant difference in delirium severity. Despite this, the intervention group patients presented with better psycho-functional recovery scores when compared with the control group patients (p = 0.01). 14 In addition, the literature suggests there is potential for involvement of family to improve delirium detection and reduce adverse patient outcomes associated with unmanaged delirium.13,15 This is supported by a systematic review 16 and studies in geriatric care suggesting that family members are important partners in the detection and management of delirium.11,12 They also highlight that more research is required to further understand the family members’ needs and preferences when being involved in care. 16
An in-depth understanding of how family can help within ICU delirium management is needed to then investigate the effectiveness of interventions that involve family in delirium management. This study aimed to explore the perceptions of former ICU patients and their families together, regarding the involvement of family in delirium management.
Methods
Setting and sample
Inclusion and exclusion criteria for patient participants.
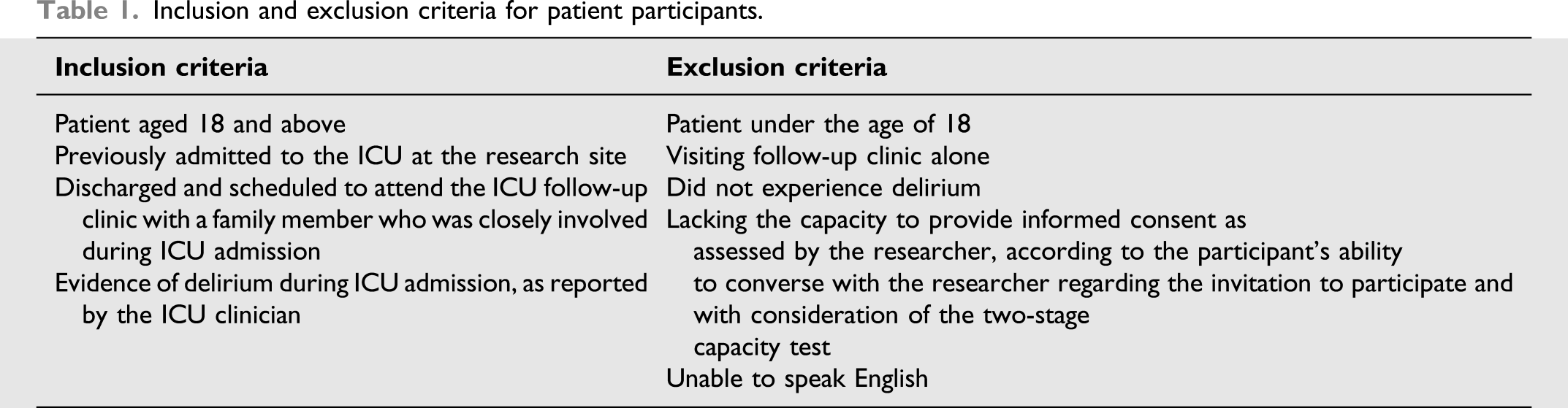
Participants were patients previously admitted to the ICU at a large teaching hospital in East Midlands, England. The ICU had a high-level of family involvement with 8 hours of visiting daily and family updates when required. However, there were no delirium detection scoring practices in place at the time of the study; these have since been implemented. A structured education programme to involve families in delirium management was not in place at the time of this study.
Provided the patient met these criteria the family members also needed to be above the age of 18, able to speak English and able to consent to participation in the study.
Appropriate approvals were given by the National Health Service, Cambridge South Ethics Committee (19/EE/0086) and the Health Research Authority.
Patients who were admitted to the ICU for a minimum of 5 days or mechanically ventilated for a minimum of 48 hours were sent an invitation letter to the ICU follow-up clinic by the direct care team. Once patients were booked in for a follow-up appointment, they were sent patient information for the interview study.
After the follow-up appointment, the clinical team asked the patient and their family member if they were interested in taking part in the study. Interviews took place immediately after the follow-up appointment. The average duration of each interview was approximately 20 minutes. Field notes were taken by the researcher to record non-verbal aspects of the interview. External psychological support was available and offered for participants that experienced distress and required additional support.
Data collection tools
The semi-structured interview followed a guide created by the researcher, which included the questions outlined in Appendix 1. The interview guide was reviewed by a group of patient and public involvement members and then piloted on non-clinical colleagues.
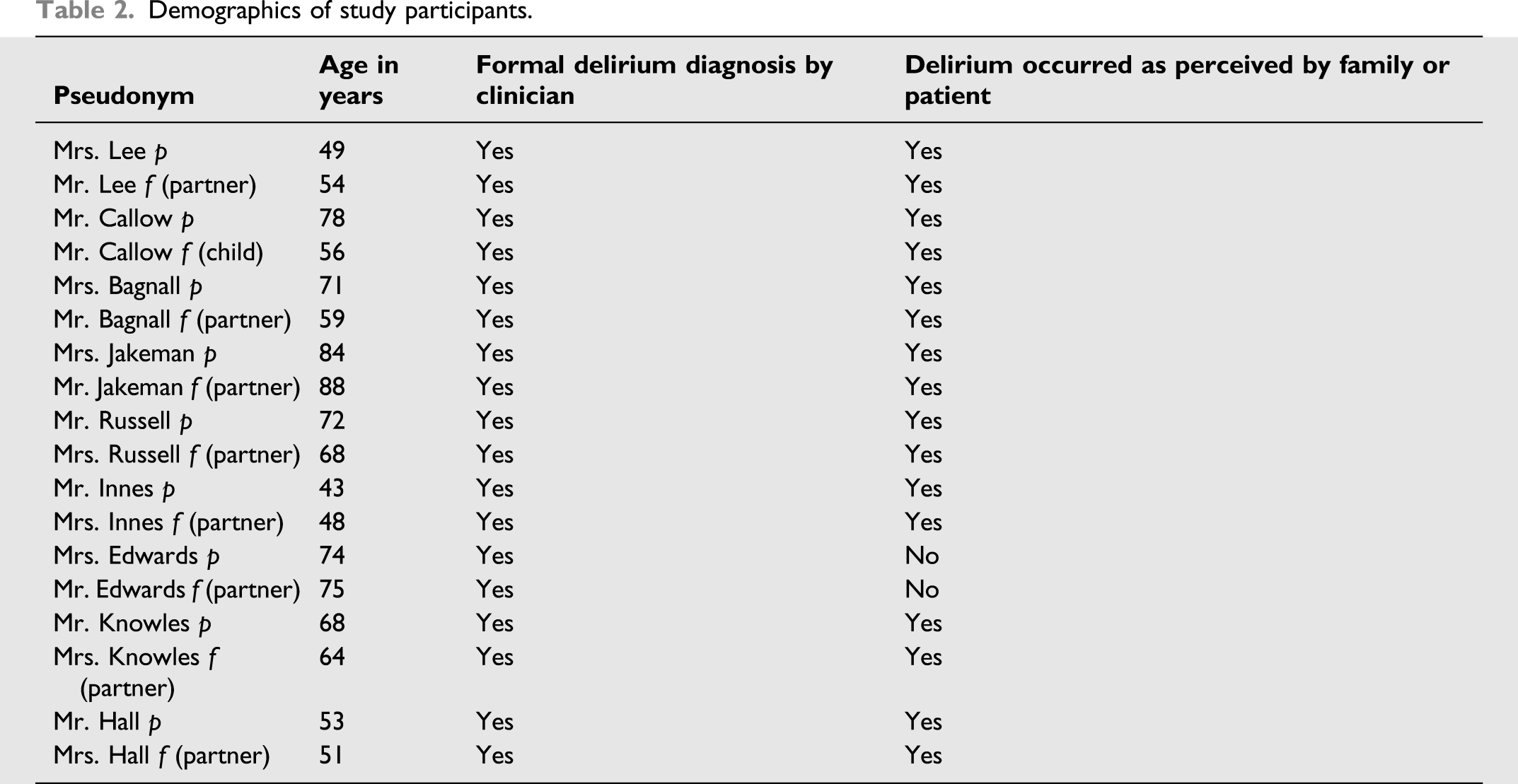
Demographics of study participants.
Data analysis
The interview audio was transcribed verbatim by the researcher and external transcribers from the University of Lincoln. All participants were informed of this and that data would be anonymised. Interview transcripts were read and checked against the audio-recordings for accuracy and to allow familiarisation with the data. Following this, codes were generated and collated with the relevant extracts from the data, supported by field notes taken by the researcher during the interview. This allowed important aspects of the interviews to be acknowledged regarding non-verbal communication and expression of emotion.17,18
The codes and interview data were analysed using thematic analysis. An inductive thematic analysis was implemented. 17 Thematic analysis was utilised as it is a useful method for examining the perspectives of different research participants. 18 To enhance trustworthiness, an experienced research supervisor supported research rigour, at all stages of the study and analysis.
Nine interviews were conducted based on the occurrence of thematic saturation. The researchers observed repetition occurring within interviews and additional interviews were not adding new information.
Findings
Nine interviews took place with former ICU patients and their family members. 18 participants were interviewed of which nine were former patients, paired with either their partner or child. All were above the age of 40 and lived in the United Kingdom. The demographics and delirium diagnoses are presented in Table 2, in which pseudonyms have been assigned; p denotes former patient, and f, family member. All patients had a delirium diagnosis by the clinician; however, one patient and their partner did not believe delirium occurred during this ICU admission, but it had occurred in a previous ICU admission.
Upon coding of the interview data, three themes emerged: (1) understanding and education about delirium, (2) influencers of delirium management, and (3) family-based delirium care.
Understanding about delirium
All participants shared that they did not understand what delirium was or how it could be managed. In addition, family participants felt generally unaware of what was happening with the patient and their condition throughout their critical illness, even after discharge from the hospital. It was at the follow-up appointment where they received more information and understood about delirium and what the patient had gone through. This was particularly distressing as family members were not able to fill in the gaps for the time the patient had lost as they did not fully understand what had happened. One family member expressed that if they had been told more about delirium and the patient’s clinical condition, the patient would have benefited in the long term, as making a psychological recovery was difficult without an understanding of what had happened: ‘It was a bit concerning, when she started saying things like that…. and you wondered whether…she’d been starved of oxygen and her brain has been affected….. explanation at the time as to what’s happening to her … to understand it, and then to explain to her, (the patient) so it reassures her. That would help us both’. Mr. Bagnall f.
It was raised by family participants that support was needed beforehand for the family to prepare themselves before seeing the patient experiencing delirium. One family participant shared that lack of awareness of delirium and the critical illness made this unduly difficult: ‘Teach them, explain to them the situation and educate them on how to act around their loved one, actually if we don’t know how to react we think what’s wrong, is he crazy now’. Mrs.Hall f
One participant expressed the need for regular meetings to update and educate the family. One family member participant described that education would be best done as a conversation with the family, supported with written information.
Influencers of delirium management: family and healthcare professionals
Family members directed the interviews responses, as they were able to recall events in comparison to the patient, who in most cases has minimal recollection of events.
Participants shared conflicting views about the involvement of ICU staff in the management of delirium. Two patient participants specifically spoke about how much it helped when ICU staff took time out and spoke with them, helping them to realise moments in which they were not experiencing delirium: ‘Somebody who’s qualified should come round every so often and even if you’re not delirious it could make you maybe understand that you’re not delirious cause they can’t make you understand when you are delirious’ Mr. Russell p.
On the other hand, one patient experienced hallucinations involving ICU staff. This had created fear around ICU staff, which worsened their delirium and overall psychological state: ‘He identified with them as they’re the enemy, which they’re not but in his world he said they’re taking me out to this lake’. Mrs. Innes p.
Furthermore, it was expected by some participants that medication had a role to play in management. One participant described unnecessary suffering that had occurred due to delirium only being treated when the patient became agitated. Consequently, they felt that an earlier intervention was required: ‘He was getting more visibly anxious… heart rate was over 200…. trying to get out the bed… they were saying it’s okay just try and calm down you’re in ITU. He was like yeah okay but really he was just getting worse...the delirium was untreated till it became severe enough to require medication’ Mrs. Innes f.
Family-based delirium care
Overall, seventeen of the eighteen participants felt that family had a vital role to play in psychological care and delirium management. These participants all stated that anxiety and agitation could be alleviated by the family’s presence and knowing the patient well was important for delirium management. One patient suggested that a family member should be present during mobilisation or extubation from mechanical ventilation, to provide a familiar face during anxiety-provoking activities.
One family participant shared that it was difficult to get involved or ask questions as they did not want to get in the way of the bedside nurse, but they would have liked to be supported to get involved in any way possible.
Patients reported that visits from family were beneficial for their psychological wellbeing, to stop them from being delirious, as they elicited positive emotions and boosted morale. They needed someone to talk to, which visitors provided. This included being told about normal life outside of the hospital: ‘I’d talk to him about the normal day to day stuff like the kids...it wasn’t about what was going on around him it was just about life and trying to distract him’ Mrs. Hall f (partner).
One patient mentioned that photographs of the location he walks his dogs every day were particularly helpful as a ‘trigger’ to bring him back to reality and out of a delirious state. Moreover, the patient expressed that personal aspects of an individual’s life may have the potential to improve delirium: ‘Once I knew where they were, something flashed. I could remember, I could recall it. I knew exactly what it was. Then the next couple of photographs she showed me, I knew exactly where they were’ Mr. Knowles p
Family-member participants suggested that more effort should be made to involve and direct the family in delirium care as well as to find out more about the patient and how delirium can be managed using this knowledge. Likewise, one family-member participant highlighted that they would have liked to be asked about the patient’s personality or their normal life: ‘ I can’t remember anybody asking me as a person, what her attitude was, was she this abrupt before…that might have really helped her’ Mr. Lee f
Discussion
This semi-structured interview study found that family members were viewed to have a valuable role to play in the management of delirium in the ICU. This study found that there was a lack of understanding about delirium amongst family members and how they could have supported delirium management. Family education about delirium is needed early and regularly, with written information offered to all families. These findings are consistent with studies investigating delirium prevention activities. Smithburger et al. 19 found that in investigating perceptions around delirium prevention, families want more education and direction from ICU staff.
The clinical manifestation of delirium, particularly hyperactive delirium, can cause the family severe distress. 20 This is supported by O’Malley et al. 21 who suggested that delirium can cause families severe distress, so ICU staff must be able to support family and encourage family-based interventions. 21 Our study found that there were a variety of perspectives between participants on whether delirium can be managed and how. Family members may expect that medication exists to easily manage delirium; therefore, family must be informed of the current treatment options available. 23
Similar to the findings in the literature, our study found that families were keen to be involved in delirium and wanted ICU staff to facilitate their involvement.21,23 Furthermore, our study found that increased family involvement during anxiety-provoking moments such as extubation or mobilisation could be beneficial in supporting the patient and helping better manage their delirium due to the presence of a familiar face. Similarly, the literature supports that increased family presence through unrestricted visiting hours can reduce a critically ill patient’s anxiety and agitation. 25
An unexpected finding from our study was that families also wanted to better understand the clinical events that occurred throughout the ICU admission prior to discharge, as this was essential to help with long-term psychological recovery. 25 This is supported by Stayt et al. 26 who emphasise the importance of family in helping patients to make sense of what they experienced. This was associated with the psychological recovery process, as family play a critical role in helping the patient fill the gaps and sort the real from the unreal. 27 However, Gay et al. 28 found that family meetings fail to occur in a timely manner for most patients in ICUs despite the established benefits of early and effective communication. 29
It is also important to consider that the increase in involvement of family members can also lead to additional workload for ICU staff. Lloyd et al. 30 found that barriers to family-centred care include the staffing constrains, high staff workload and time pressures. This reduces the ability for ICU staff to be able to provide education and be involved with the patient’s family 31 ; hence our study found that not all family members were asked about the patient’s life and personality. A meta-analysis of 16 studies found an association between flexible visiting policies and reduced frequency of delirium. Although this increased family member’s satisfaction, it found to be associated with higher burnout levels. 26 On the contrary, Rosa et al. 24 found no significant reduction in the incidence of delirium in ICU patients with the implementation of flexible family visitation policy versus standard restricted visiting hours. Although, this may be because the interactions to involve family in delirium management have more influence on delirium than increasing visitation hours alone. Furthermore, this trial excluded a large portion of patients with increased risk for delirium, who may have benefited from increased family presence. 28
Interventions such as video-ICU delirium education have been found to be effective in educating family members about delirium management, at their own pace, without creating an increase in workload for staff. Future work is needed to find out how these interventions impact delirium management and reduce incidence, length, and severity of ICU delirium. 22
Interestingly, within our study we found that one patient and their partner did not agree with the clinician’s ICU delirium diagnosis. This was only mentioned in the interview once, but it would have been interesting to explore this contradicting finding. The literature suggests that family members can add value in detection of ICU delirium. 32 Therefore, future work into family-centred delirium detection may be of significance in improving delirium care.
We hypothesise that the increased involvement of family members in delirium care may improve delirium management by reducing delirium length and severity. Appropriate interventions should be developed considering the needs of the families and ICU staff. Future research implementing specific family-based intervention versus standard of care is needed to support the current literature in understanding the impact family members have on delirium management.
Strengths and limitations
This study has captured the experiences of former patients and family within the ICU that experienced delirium and allowed an understanding of how the family can be involved in delirium management. The confirmability of this study was supported by the reflexive research process through regular corroboration between the authors to discuss the methods, and developing findings. 30 However, a limitation to this study was that the participants invited to the study were limited to those who chose to attend the follow-up clinic appointment. Many patients do not choose to attend and therefore the perspectives gained from the interviews in this study may be subject to participant bias. Although data saturation was achieved, no new themes emerged from the data; it is difficult to determine data saturation within interview studies, as even after a large number of interviews a single additional interview could potentially reveal new information despite no new ideas arising in all the prior interviews. 32
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was supported by NIHR (granted by NIHR bronze award internship).