
Abstract
Urine output is an important clinical measurement and oliguria may highlight the development of acute kidney injury (AKI) earlier than serum creatinine (sCr). Despite the importance of urine output monitoring, there are no definitive guidelines or recommendations for best practice. A survey was sent to healthcare professionals with a specialist interest in AKI to gather opinions of what constitutes a good standard of urine output monitoring and by corollary missed care, post- major surgery. Data was gathered from 221 respondents. Results will inform audit and improvement projects in post-operative nursing care.
Introduction
Assessment of urine output is a vital assessment for good patient care in hospitals and for the prevention of patient deterioration, including acute kidney injury (AKI). AKI affects at least 10% of general hospital admissions, and incidence is even greater in the post-operative period. 1 AKI incidence varies depending on the surgical setting, but specifically in patients after hip fracture and major abdominal surgery, incidence has been reported as high as 28%2 –5 and 35% respectively. 6 AKI is associated with increased short-and long-term morbidity and costs estimated as at least £1 billion per year in the UK NHS. 7 In 20%–30% cases, AKI is preventable 8 which has driven interest in strategies to improve early recognition and the delivery of basic elements of AKI care, including urine output monitoring.
Urine output plays an equal part in the Kidney Disease Improving Global Outcomes (KDIGO) AKI criteria, 9 but there are no definitive guidelines for best practice, including frequency of measurement. Informing the body of evidence are small, retrospective, observational studies; surveys; audits and quality improvement projects.10 –13 It is recognised that the implementation of urine output monitoring is resource intensive and may be only partially complete, if at all.11,12 This could be defined as ‘missed care’.14,15 However, in order to characterise missed care, it is necessary to gather opinions regarding optimal frequency of urine output monitoring.
Methods
A survey, endorsed by the European Society of Intensive Care Medicine (ESICM), was sent to ESICM members (physicians, nurses or allied healthcare professional in and around Europe) from the AKI section to gather opinions regarding expected standards of urine output monitoring in patients on hospital wards. Two post-operative periods were considered: the first 24 h, and subsequent 24–72 h following elective colorectal resection and, hip fracture surgery. Two time periods were specified as it was felt that requirements for urine output monitoring were different during the first 24 hours and subsequent 24–72 h following colorectal and hip fracture surgery. Data were collected during July and August 2022 using google forms online platform. The survey included four multiple choice questions, for which one answer could be given, as follows:
(1) In your opinion, what do you consider to be a good standard of urine output monitoring in patients on hospital wards after a period of theatre recovery, in the first 24 hours following elective colorectal surgery?
(2) In your opinion, what do you consider to be a good standard of urine output monitoring in patients on hospital wards, in the following 24–72 h following elective colorectal surgery?
Possible answers for questions 1 and 2: urine output recorded every 1; 2; 3–4; 5–6; 7–8; 9–12; 13–24 h.
(3) Missed care has been defined as care that is delayed, partially completed or not completed at all. In your opinion, in the first 24 hours following hip fracture surgery, what would you consider to be missed care with regards to urine output monitoring in patients on hospital wards?
(4) In the following 24–72 h after hip fracture surgery, what would you consider to be missed care with regards to urine output monitoring on hospital wards?
Possible answers for questions 3 and 4 were urine output recorded every; 2, 4, 6, 8, 12 h.
Results
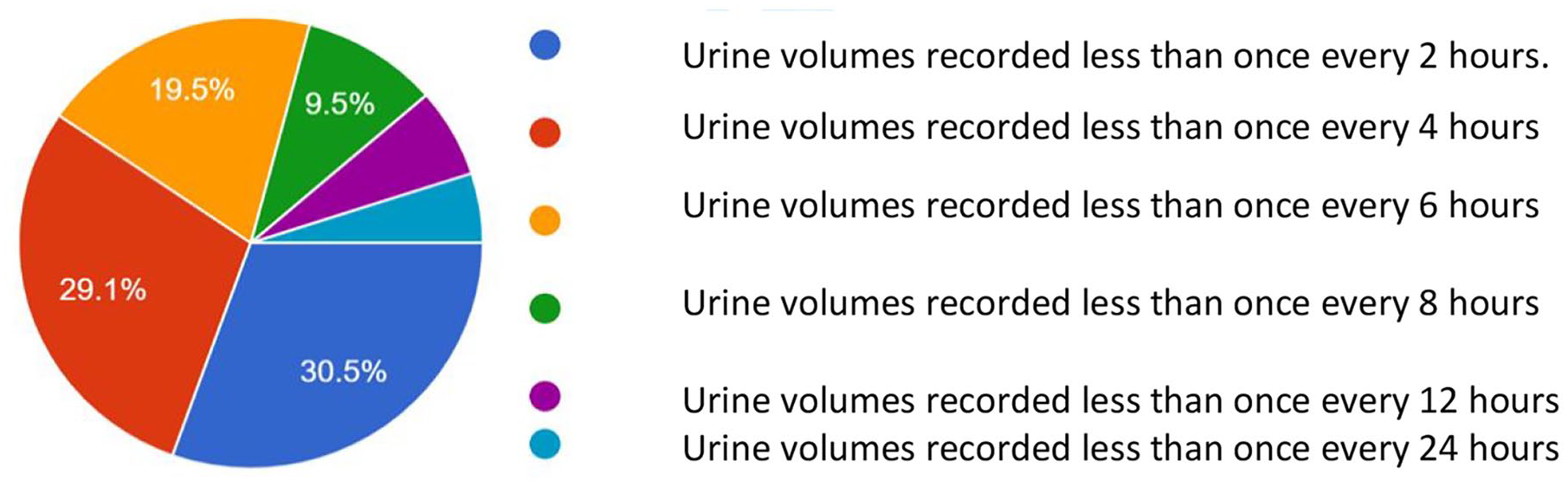
With a response rate of 53%, opinions were gathered from 221 respondents. Results showed that during the first 24 hours following elective colorectal surgery, 57% (n = 126) felt that urine output should be recorded at least every 2 h and 85% (n = 187), at least every 4 h, see Graph 1. In the first 24 hours following hip fracture surgery, care was regarded as being ‘missed’ by 60% (n = 131) of respondents, if the frequency of urine output recorded was less than every 4 h, and by 79% (n = 174) if the frequency of urine output recorded was less than every 6 h post-surgery, see Graph 2.
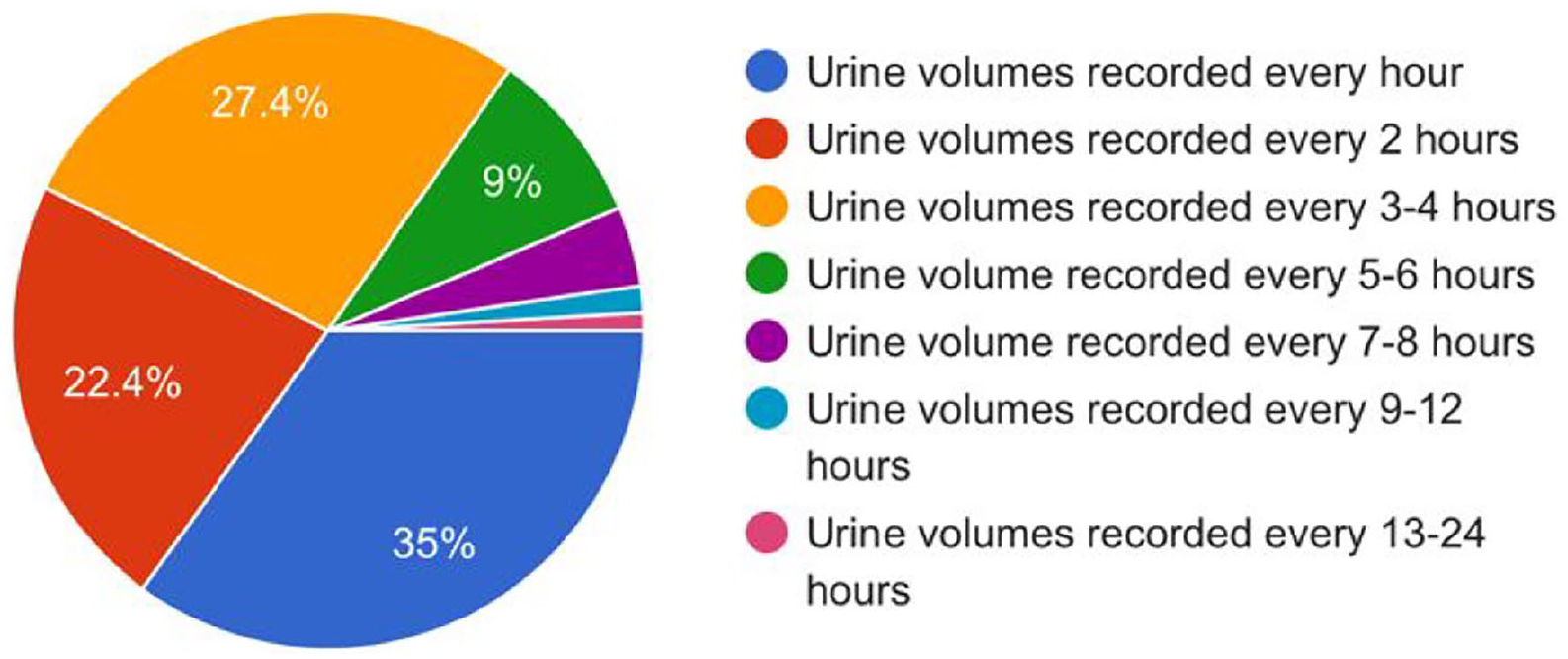
Results showing what is considered a good standard of urine output monitoring in patients on hospital wards, following a period in theatre recovery, in the first 24 hours following elective colorectal surgery.
Results showing what is considered to be missed care with regards to urine output monitoring in patients on hospital wards in the first 24 hours following hip fracture surgery.
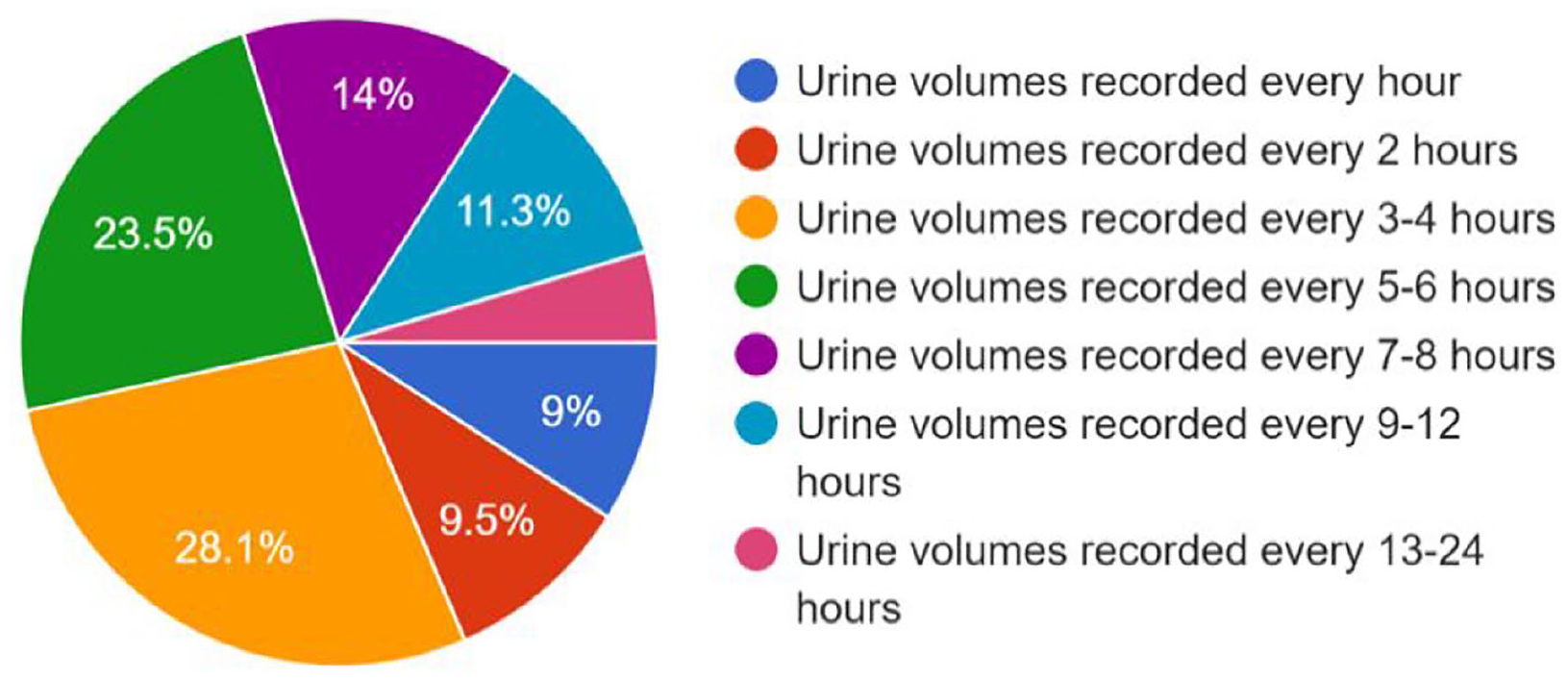
In the subsequent 24–72 h following elective colorectal surgery, 70% (n = 155) of respondents felt that urine output should be monitored at least every 6 h, see Graph 3. Missed care was considered by the majority (51%; n = 113), if the frequency of urine output monitoring was less than every 6 h post-surgery and by 72% (n = 158) if the frequency of urine output measurements were less than every 8 h post- hip fracture surgery, see Graph 4.
Results showing what is considered a good standard of urine output monitoring in patients on hospital wards, in the following 24–72 h following elective resection surgery.
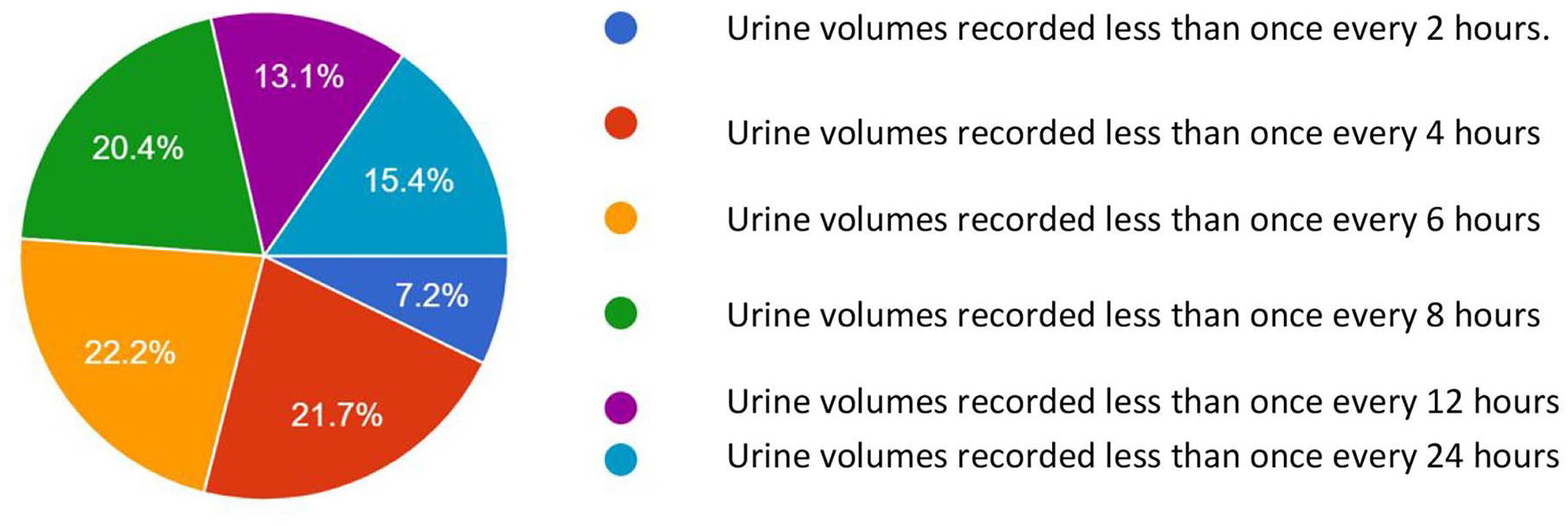
Results showing what is considered to be missed care with regards to urine output monitoring in patients on hospital wards in the following 24–72 h after hip fracture surgery.
Discussion
To our knowledge, this is the first work to gather health professionals’ opinions regarding appropriate urine output monitoring in the post-surgical setting as well as to define missed care, for urinary output monitoring, in this patient group. Urine output as an easily available biomarker of kidney function that directly effects kidney perfusion 16 but evidence suggests, that its importance is often overlooked.11 –13 With clearer guidance and enhanced monitoring on hospital wards post-surgery, low urine output and oliguria, could be used for the early detection of AKI, potentially improving patient outcomes from AKI. Current evidence suggests that oliguria may detect AKI earlier than serum creatinine (sCr)17 –19 and even in the absence of a sCr rise, oliguric AKI is associated with increased use of kidney replacement therapy,18,20,21 longer ICU and hospital stay20,22 and increased mortality.16,18,21,23 –25 These results provide a useful reference standard for future quality improvement studies in this area.
Strengths
This was a large sample, multi-national survey with opinions from healthcare professional across multiple disciplines and healthcare settings worldwide. The surveys gathered opinions regarding standards of urine output monitoring in patients following hip fracture and colorectal surgery, populations that are commonly encountered in hospital settings, and so aiding generalisability. These opinions will be used to inform further research, where there are currently no guidelines for best practice.
Limitations
The survey was sent by the ESICM to all members of the AKI section and responses were received via google forms. As a result, we were unable to ascertain who completed the survey, and thus if this was a truly representative sample. All respondents, as members of the ESICM, were physicians, nurses or allied health professionals with a specialist interest in AKI, but further details regarding individuals’ professions, or countries of practice were undetermined. The proportion of respondents working in critical care settings was also unknown, but the expectations of these staff for more frequent urine output monitoring may have been greater. The survey was conceptualised and compiled by the authors, and with no previous guidelines for best practice, the survey questions were based on consensus opinions.
Footnotes
Acknowledgements
I would like to thank the Mr Guy Francois at the ESICM for organising endorsement of the survey and for sending out to the members of the AKI section. An excellent response rate was achieved as a result.
Authors’ contributions
HB, LH, LF, MW, CK were involved in the conceptualisation of the survey. HB drafted the letter. LH, LF, MW and CK reviewed and edited the letter.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was undertaken as part of an ARC KSS funded PhD awarded to the first author.
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Availability of data and materials
Data and materials are available on request