
Abstract
Background
Delayed gastric emptying (DGE) is a major cause of undernutrition that can be overcome using nasointestinal (NI) feeding, but tube placement often fails. We analyse which techniques enable successful NI tube placement.
Methods
Efficacy of tube technique was determined at each of six anatomical points: Nose, nasopharynx-oesophagus, stomach-upper and -lower, duodenum part-1 and intestine.
Results
In 913 first NI tube placements, significant associations with tube advancement were found in the pharynx (head tilt, jaw thrust, laryngoscopy), stomach_upper (air insufflation, 10 cm or 20–30 cm flexible tube tip ± reverse Seldinger manoeuvre), stomach_lower (air insufflation, possibly flexible tip and wire stiffener) and duodenum part-1 and beyond part-2 (flexible tip and combinations of micro-advance, slack removal, wire stiffener or prokinetic drugs).
Conclusion
This is the first study to show what techniques are associated with tube advancement and the alimentary tract level they are specific to.
Introduction
Delayed gastric emptying (DGE) occurs in 30–46% of critically ill patients1–2 and is associated with prolonged ventilation, ICU and hospital stay and increased mortality.1,3 Although a causal link to these outcomes is not certain, DGE is associated with reduced feed and drug delivery. 1 However, early EN remains preferable to delayed nutrient intake or parenteral nutrition because it is associated with reduced mortality and infection. 4 Prokinetic drugs reduce DGE, 5 but even combined metoclopramide and erythromycin treatment is associated with tachyphylaxis. 6 Conversely, nasointestinal (NI) feeding, from duodenum part-1 to the jejunum, delivers more nutrition in patients with DGE refractory to metoclopramide treatment when compared with nasogastric (NG) feeding plus prokinetics. 7 However, aspiration risk appears to decline as NI placement becomes more distal. 8 In addition, NI feeding, rather than NG, was associated with less reflux, vomiting and ventilator-associated pneumonia 9–11
Endoscopy and fluoroscopy are highly successful in achieving intestinal tube placement, but increase clinical risk from their invasive nature, irradiation, off-ward location and exposure to infection. Guided bedside tube placement would minimise these risks and any delay to feeding. Unfortunately, published techniques for achieving intestinal placement are mostly limited to moving the tube through the pylorus. Using prokinetic drugs, combining air insufflation + right lateral decubitus position + a weighted tube or using tube rotation with a bent guide-wire, failed to reach the intestine in 8–17% and tubes only advanced beyond duodenum part-3 in 17–22%.12–14 Hawk and Valdivia 15 suggested operator skill as a reason for improved guided versus blind transpyloric tube placement.16,17 However, the success associated with guidance may only be achieved if the guidance prompts the use of techniques. 18 Manufacturer guidance for Cortrak-guided placement suggests use of IV metoclopramide, laying the patient flat (upright for a distended abdomen), an air bolus and slow tube insertion to prevent coiling. 19 However, this guidance was unsubstantiated by published citations. To address the lack of systematic evidence, we analysed techniques, tried or developed in clinical practice, to achieve tube advancement. To our knowledge, this is the first analysis of multiple techniques and their efficacy at different anatomical points.
Methods
Design and data collection
In a single UK ICU we retrospectively determined the success of our techniques for clinically required NI tube placements from 22.03.07 to 31.08.21. We acquired demographic data, tube position attained, problems of advancement, techniques and anatomical points at which they were used from a database of contemporaneous records of bedside NI tube placement. Anatomical points were cross-referenced with digital traces of the tube path. APACHE two scores were obtained from ICNARC (Intensive Care National Audit and Research Centre). All patient ID was removed and disease transformed into a general disease category prior to export to the statistical package for anonymised publication.
Techniques
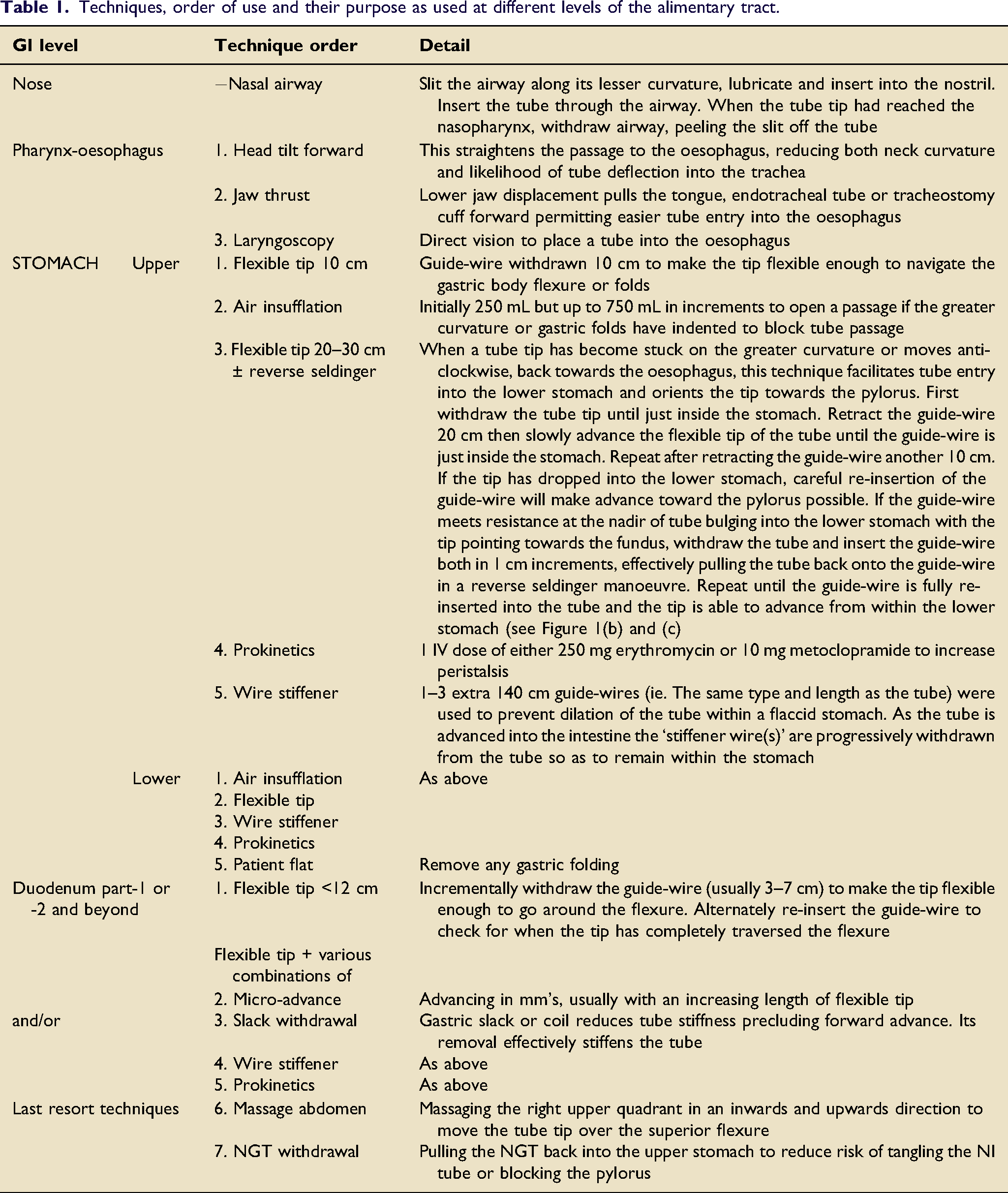
Techniques, order of use and their purpose as used at different levels of the alimentary tract.
Patients and equipment
Patients were referred for NI tube placement when suffering delayed gastric emptying (DGE), defined as a gastric residual volume ≥250 mL in a 4-h period or vomiting, that was refractory to 24-h of treatment with 10 mg IV metoclopramide or, to avoid delayed feeding, if DGE occurred on Friday. Patients who were moribund, had anatomical contraindications or refused consent were declined tube placement. Criteria for patient referral and the equipment used for tube placement remained constant. Guided placement was done using a 140 cm 10FG Cortrak™ tube (Avanos Medical Inc). Cortrak produces a real-time computer trace of the path of an electromagnet within the tube. Anatomical points were interpreted from trace characteristics, previously described.20–22 This permitted the operator, an ICU dietitian or consultant, to guide tube placement and confirm final position. Tubes left in situ were used for feeding. There were no instances of undetected lung misplacement.
Analysis
Analysis was restricted to a patient’s first tube placement to avoid over-representation by repeat placements. Using ‘R Studio Version 1.1.463′ most parameters did not meet a normal distribution (Shapiro-Wilk test) so continuous data were analysed using the 2-sided Wilcox rank sum test and presented as median (inter-quartile range, IQR). Categorical variables were analysed using Fisher’s exact test. Significance was taken as a p <0.05. These tests were used to check for missing data bias, comparing baseline parameters for patients with versus those without 'techniques' data, and in univariate analysis of associations with tube advancement.
Difficulty in tube advancement and the techniques used to overcome it were analysed at six anatomical points: (1) Nose, (2) Pharynx when attempting to enter the oesophagus, (3) Stomach_upper (4) Stomach_lower, (5) Duodenum part-1, particularly the superior flexure and (6) Intestine from duodenum part-2 to jejunum, particularly the duodenuo-jejunal (DJ) flexure.
For each anatomical point, analysis: (1) Only included difficult placements, based on operator comment and/or use of a technique to overcome difficulty and/or failure to advance; (2) Omitted placements where an alternative technique had been used but; (3) Coded as ‘failed placement’ when techniques, additional to the one being analysed, were later used.
Univariate analysis was conducted for each technique within its sub-set of placements. If a higher proportion of tube advancement was associated with use of the technique (p < 0.05) or the median or proportion of baseline parameters differed depending on use of the technique (p < 0.2) these variables were entered into a logistic regression model. Because techniques used at subsequent anatomical points might affect final tube position, these models were binary, reporting associations with advancement, or not, at a specific anatomical point. The exception was the use of ordinal logistic regression to analyse tube advancement from duodenum part-2 to parts -3, -4 or jejunum when using ≥3 techniques where further techniques would not be added. Small sample sizes and/or a zero value for an option sometimes caused logistic regression to fail to separate effects of independent variables and made statistical output unreliable. For this reason we present p-value, OR and 95%CI for univariate analysis, but note where LR failed or where the apparent association between technique and tube advance may be confounded. In all other analyses, even where baseline parameters showed a significant association to technique use, the association between technique and tube advance remained statistically significant. Co-linear variables (variance-inflation factor >5) were omitted from the model.
Baseline parameters included demography (age, estimated or actual height, weight and body mass index [BMI] and gender) and clinical parameters (APACHE two score, disease category, airway and consciousness). Analysis was done in the order techniques were used at a particular anatomical point.
Ethics
Data collection was done as part of a registered UK quality improvement project (QI71316), using standard practice, and therefore did not require ethics board approval.
Results
Study group
913 of 947 primary NI tube placements were analysed; all baseline parameters were similar to the 34 placements with missing data (Appendix 1), including tube placement day (p = 0.5) and operator (p = 0.1). The referral policy and contemporaneous records for tube placement remained constant during this period, but specific techniques were added over time. Most placements (83.7%) were undertaken for DGE refractory to 24 h of metoclopramide treatment; the remainder were placed for DGE where prokinetic drugs were contraindicated, previously failed or to permit peri-operative feeding.
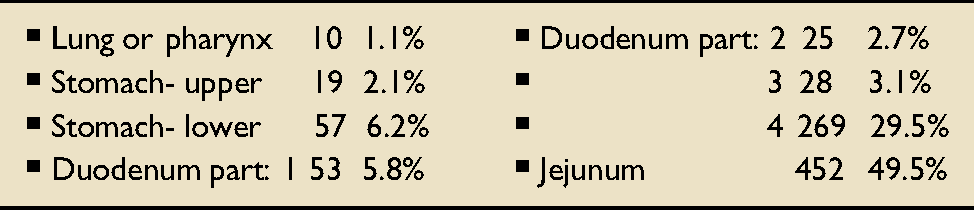
Lead operator and tube position
Techniques
Associations between technique and tube advancement beyond each anatomical point.
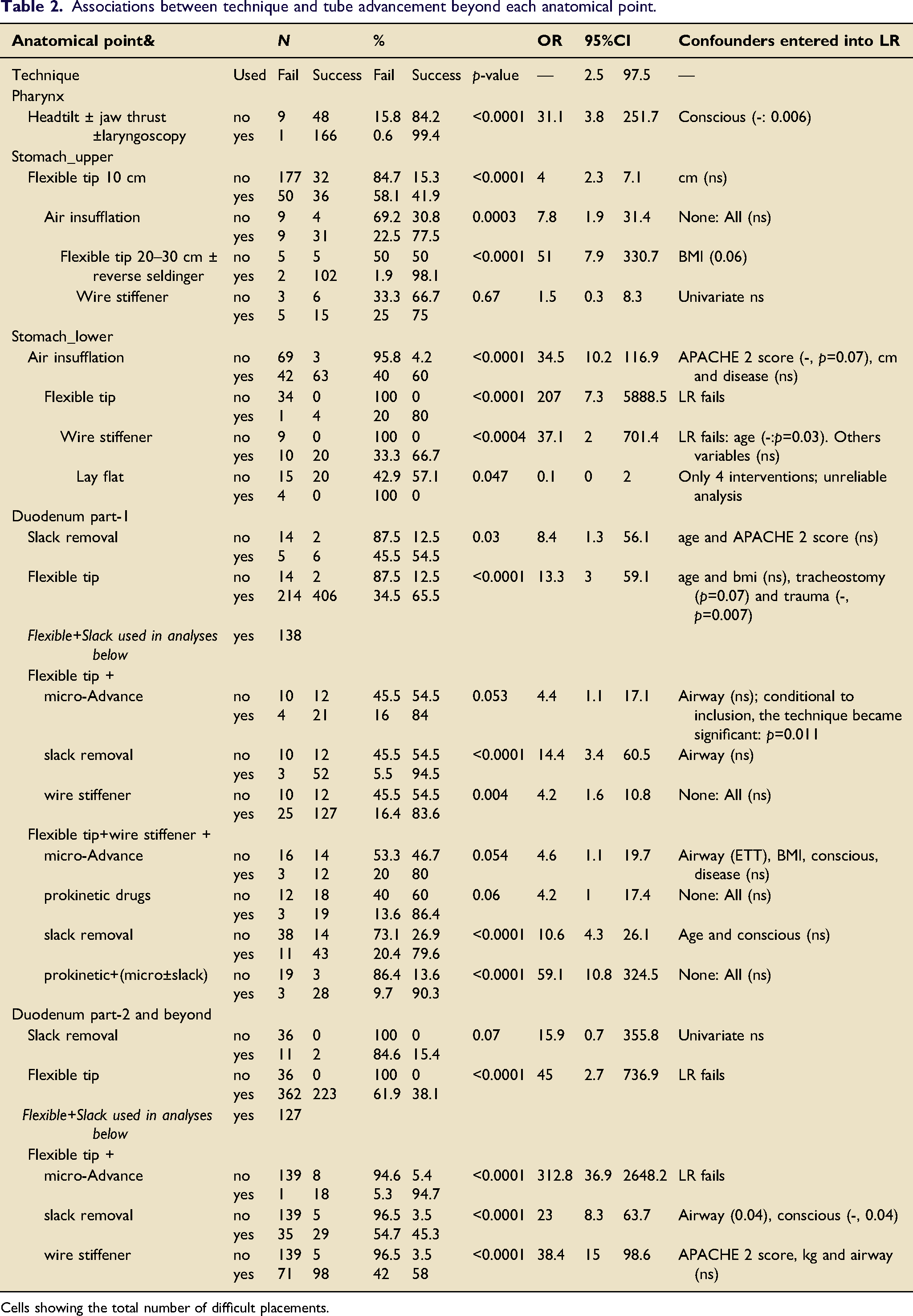
Cells showing the total number of difficult placements.
Of tubes reaching the upper stomach, advancement was difficult in 295 of 903 (32.7%) of placements; 2.1% failed. Sequential use of flexible tip (10 cm) or, where that failed, air insufflation and when that failed a 20–30 cm flexible tip ± reverse Seldinger manoeuvre were all significantly associated with tube advancement (p < 0.001) independent of BMI (trend) and other baseline parameters. Prokinetic drugs were not used and use of a wire stiffener was of marginal benefit to tube advancement.
Tubes reaching the lower stomach presented difficulty to advancement in 177 of 884 (20%) of placements; 6.2% failed. In univariate analysis, air insufflation, a flexible tip or stiffener wire were all associated with tube advancement. However, using logistic regression, only air insufflation was independent of the negative association with APACHE two score. Logistic regression including a flexible tip or wire stiffener failed due to small samples and zero successes when not using a technique; confounding is therefore possible for these variables. There were too few interventions of laying the patient flat or prokinetic drug use to analyse these techniques of last resort.
Of tubes reaching duodenum part-1, 785 of 827 (94.9%) of placements presented some difficulty to further advancement; 5.8% failed. Independent associations with tube advancement were found for slack removal (p = 0.03) and use of a flexible tip (p = 0.0001), after accounting for tracheostomy use (+: p = 0.07) and trauma (-: p = 0.007). In placements where a flexible tip failed, adding a secondary technique was associated with tube advancement: Micro-advance only reached a trend (p = 0.05) but use of slack removal (p < 0.0001) or a wire stiffener (p = 0.004) were independently associated with tube advancement. When combining a flexible tip and wire stiffener failed, tube advance was independently associated with adding a third technique: Micro-advance (p = 0.05) or slack removal (p < 0.0001). Addition of prokinetic drugs (erythromycin in all but one), after failure of two or three techniques, was independently associated with tube advancement (p < 0.0001). It may be noteworthy that erythromycin was used as a last resort and given as a 20 min IV infusion as advancement was re-attempted 1–2 h later.
Association between technique and the distance the tube advances.
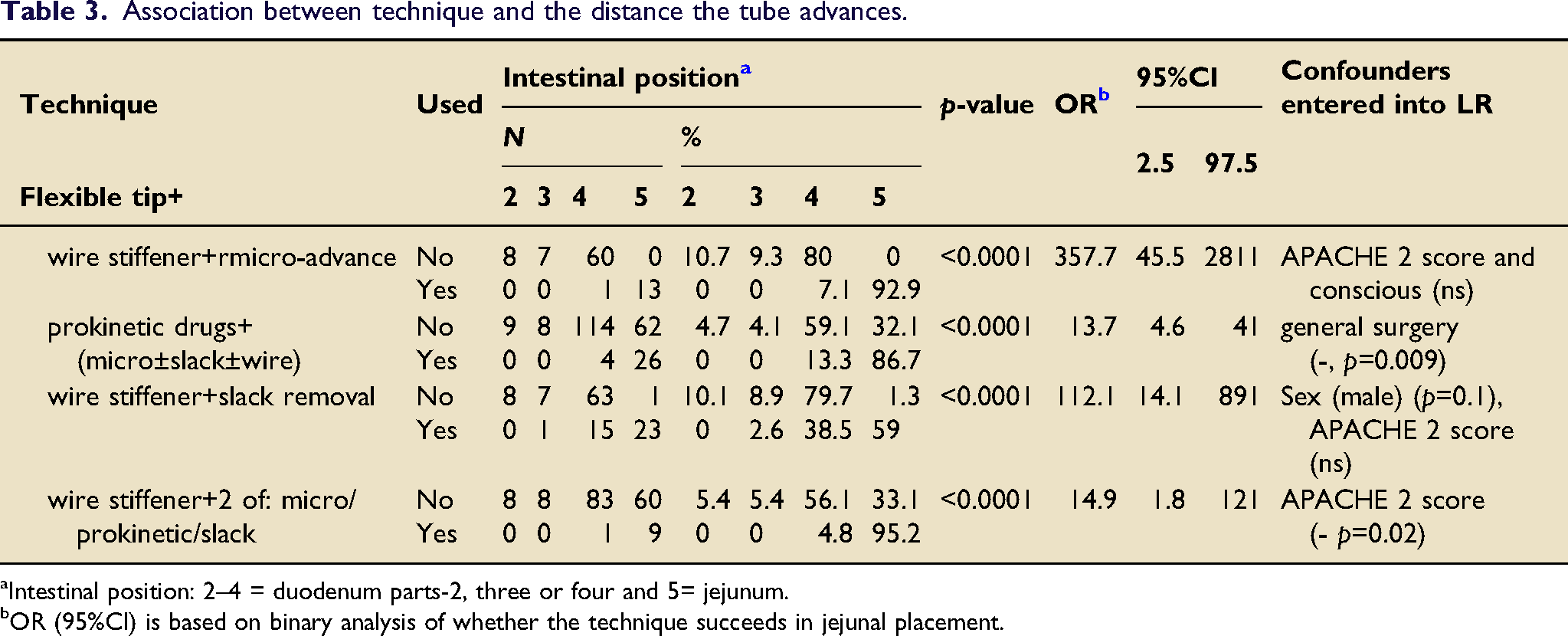
aIntestinal position: 2–4 = duodenum parts-2, three or four and 5= jejunum.
bOR (95%CI) is based on binary analysis of whether the technique succeeds in jejunal placement.
Discussion
Main findings
Successful tube advancement is highly associated with use of certain techniques. Baseline parameters were similar between placements analysed and the 3.6% for which data were missing. Techniques that may aid tube advancement were analysed only for placements that were difficult: Nose (3.3%), pharynx (24.5%), stomach_upper (32.7%), stomach_lower (20%), duodenum part-1 (94.9%), intestine (98.3%). There were too few techniques used and placement failures to analyse technique efficacy at the level of the nose. However, advancing from the pharynx to the oesophagus appeared to be aided by use of a head tilt, jaw thrust, laryngoscopy or combinations of these. Specific techniques were associated with tube advancement in the stomach_upper (10 cm flexible tip, air insufflation and 20–30 cm flexible tip ± reverse Seldinger manoeuvre), stomach_lower (air insufflation, possibly a flexible tip and wire stiffener) (Figure 1(a)–(d)) and for duodenum part-1 or beyond duodenum part-2 (flexible tip alone or combined with 1–3 techniques: micro-advance, slack removal, wire stiffener and prokinetic drugs when previous techniques failed) (Figure 1(e) and (f). Techniques: (a–c) Upper stomach, (d) Lower stomach, (e) Duodenum part-1, and (f) Intestine. [© Stephen Taylor-with permission].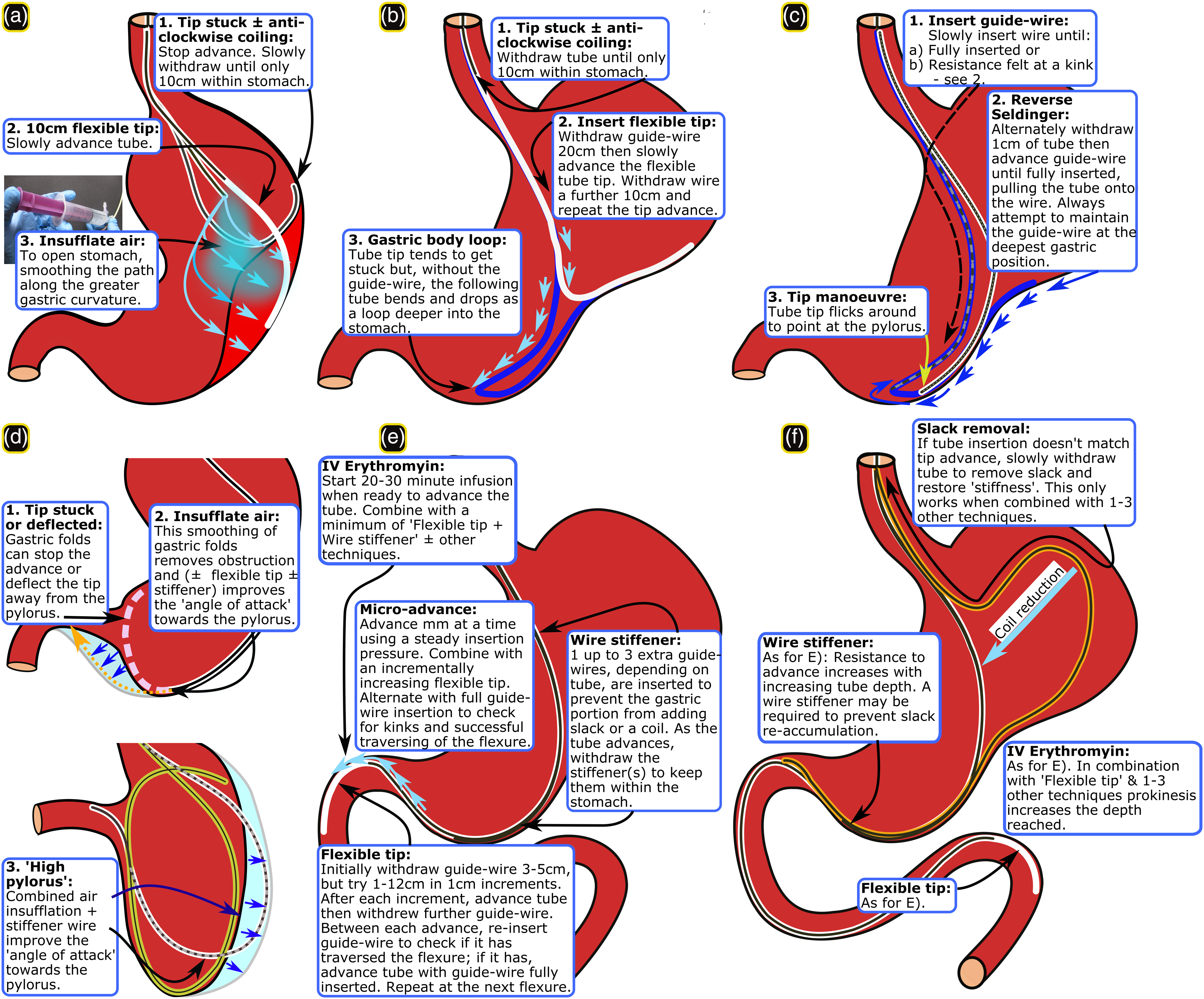
Confounding variables
Baseline parameters that were associated with technique use (p < 0.2) in one or more analysis were BMI, and presence of an ETT or tracheostomy. Past study has shown that placement can be particularly difficult at GI flexures when a patient’s BMI is low, hence a higher BMI may favour easier placement, 23 possibly because flexures are less acute. In addition, presence of an ETT or tracheostomy may be surrogates of deep sedation which improves patient tolerance during prolonged tube placement. Age, APACHE II score, being conscious and trauma were negatively associated with tube advance. APACHE II score was previously associated with advancement failure24,25 potentially paralleling its association with DGE. 3 In DGE the fundus is typically distended and flaccid causing tube advancement to stall or move anti-clockwise towards the oesophagus. Being conscious reduced patient tolerance while age and trauma may pre-dispose to poor gastric tone and reduced peristalsis.
Technique efficacy by GI level
Stomach_upper
Air insufflation13,26 and use of a 10 cm or 20–30 cm flexible tip with or without a reverse Seldinger manoeuvre, widen the stomach and permit the flexible tube to deflect past any gastric indentation, respectively. This facilitates movement of the tube tip into the lower stomach.
Stomach_lower
Again, air insufflation appears to help tube advancement by opening a collapsed stomach. Numbers were small, but a flexible tip or wire stiffener may aid tube advancement by deflecting past obstruction or changing the ‘angle of attack’ towards the pylorus, respectively. We did not employ the right lateral decubitus position or a cork-screwing (tube rotation) manoeuvre with a bent guide-wire.13-14 This was because a Cortrak receiver unit’s position would be difficult to maintain and the electromagnetic wire easily breaks, respectively. These techniques require testing using different guidance equipment. Too few patients were lay flat or given prokinetic drugs to know their effect.
Duodenum part-1
It appears that use of a flexible tip facilitates tube advance through duodenum part-1 and specifically enabled the tube to slide over the, often acute, superior flexure. When this fails adding one or more of micro-advance, slack removal or wire stiffener appears to aid advance. Micro-advance enables the flexible tip to move around the flexure without kinking and, along with adding one or more wire stiffeners up to the level of the lower stomach, reduces the risk of accumulating a slack loop in the stomach. Removing slack restores the guide-wire rigidity to facilitate forward pressure. Erythromycin infusion started when re-attempting passage of the superior flexure initiates increased peristalsis. 27 Use of 3–4 of the above techniques appear to succeed when single or dual techniques fail. Use of abdominal massage or NG tube removal were too rare to analyse. However, when NG tube insertion was >70 cm, its withdrawal to 50 cm immediately led to NI tube advancement on a few occasions, suggesting that it was blocking duodenum part-1.
Intestine
Successful tube advancement into the jejunum appeared to be aided by the same single, dual and triple techniques as for duodenum part-1 with the exception that slack removal alone only reached a trend. The latter may be due to small numbers. In addition, resistance to advance increases the deeper the tube moves into the intestine. Hence, slack removal alone may not restore enough rigidity to the tube within the stomach to prevent repeated collapse into a coil. Combinations of 3–4 techniques or prokinetic drug use with two or more other techniques was associated with tube advance further into the intestine, regardless of whether the tube reached the jejunum.
Limitations
Tube placement results were from a single hospital, mostly by two operators, with differing experience, over different time periods. It was therefore not possible to exclude the effect of subtle operator-specific differences of technique. However, patient referral criteria and placement equipment were constant, mitigating temporal bias. Most important, except where small sample size or zero values prevented analysis, specific techniques were highly significantly associated with placement success, independent of baseline parameters. These results do not guarantee success or failure of different techniques at specific levels of the alimentary trace, even on the same patient. Rather, the associations are a ‘try list’ guide for operators. There will be exceptions and techniques often require several attempts even after previous failure. Most of this guidance applies to active tube advancement, not to ‘peristaltic’ tube placement where prokinetic use may be essential. 28 The predominant use of in-procedure IV erythromycin but not metoclopramide related to metoclopramide use and tachyphylaxis prior to tube placement; others found similar efficacy for these drugs regarding transpyloric migration. 29 Aside from patient position, all discussed techniques could be used in a prone position with two cautions: (a) Head tilt downwards and jaw thrust are more difficult when aiding tube movement into the oesophagus; (b) If using Cortrak™ electromagnetic guidance (EMG), the anterior and lateral traces must be interpreted as mirror and inverted images, respectively; ENvue® EMG doesn’t require this. Lastly, the techniques were tested using a 10FG, 140 cm Cortrak tube and may require adaptation where tube characteristics differ. For example, traversing flexures may be more difficult with a wider-bore or stiffer IRIS (Kangaroo™) feeding tube but easier with the more pliant ENvue guide-wire. Conversely lack of stiffness at the level of the stomach more often necessitated stiffening with extra guide-wires. Good internal tube lubrication is essential to manoeuvre the guide-wire. Real-time guidance is needed for timely application of these techniques and has also been used with an IRIS direct vision tube 30 but ENvue is not yet available or tested within the UK.
Description of placement techniques, especially manoeuvres, is largely absent from manufacturer guidance. Operators therefore require clinical permissions to use these techniques within their healthcare settings. However, similar techniques are used during endoscopy. Substitution of the manufacturer guide-wire with a specialist guide-wire, often of different stiffness, is common during fluoroscopic feeding tube placement. Specifically, moving a ‘stiffener wire’ within a tube would be similar to re-tracing tube position using a near identical Cortrak guide-wire, something that is part of manufacturer guidance.
Conclusion
This is the first study to specify the anatomical level at which single or combined placement techniques may facilitate NI tube placement. Future investigation may examine the efficacy of patient position, flexible tip and wire stiffener use in lower stomach and abdominal massage close to the pyloric, superior duodenal and DJ flexures.
(1) Delayed gastric emptying (DGE) is common, can be overcome by NI feeding, but tube placement often fails. (2) Nurses, dietitians, radiographers and medics require expertise to succeed in NI tube placement. (3) To our knowledge, this is the first paper to determine the efficacy of NI tube placement techniques for each stage of the placement and explicitly describe them in order to disseminate expertise and encourage wider use. (4) We identify single or combined techniques that may significantly increase the likelihood of tube advancement at each anatomical level.Impact
Footnotes
Acknowledgements
We thank other members of the NJ team (Rowan Clemente, Danielle Milne, Francis Greer) and ICU nursing and medical staff for advice and support without which this work could not have been done. Thank you to Danielle Milne and Katie Williams for critiquing the MS.
Author contributions
S.J. Taylor equally contributed to the conception and design of the research; S.J. Taylor and K. Sayer contributed to the acquisition of the data; P. White and S.J. Taylor contributed to the analysis and interpretation of the data; S.J. Taylor drafted the manuscript. All authors critically revised the manuscript, agree to be fully accountable for ensuring the integrity and accuracy of the work and read and approved the final manuscript.
Declaration of conflicting interest
ST served on a Corpak consultation committee once in 2007 and directed a lecture fee to the Tear Fund Syrian charity 2014.2. ST and KS undertook studies sponsored by Cortrak (now Avanos Medical Inc, 2012–14) and Cardinal Health (2020- current) through North Bristol NHS Trust, but these companies had no part in the planning, execution or publication of the projects.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IMPORTANT: The UK Health Research Authority recognise this study as an audit not requiring Ethics Board approval. Their email is below and they are willing to be contacted. However, if ICCN still require IRB, please decline the submission and inform me. Because of COVID it would take many months to obtain an IRB approval.
Demography,disease,treatment characteristics and NI day: Technique data missing vs obtained.
Parameter
Detail
Technique data
p-value
Missing
Obtained
Median or n
*IQR or %
Median or n
*IQR or %
Number
(n)
34
3.6
913
96.4
-
Age
Years
56
40–68
53
37–68
0.8
Sex
Male
24
75
655
72
0.5
BMI
kg/m2
25
23–28
25
23–29
0.9
Height
Cm
174
164–180
175
167–180
0.2
Weight
Kg
76
63–84
78
68–89
0.3
APACHE 2
Score
17
9–23
15
9–21
0.5
Disease*
Medical
10
29
259
28
0.3
Neurosurgical (non-trauma)
1
2.9
121
13
—
Surgery (general)
9
27
223
24
—
Trauma
14
41
310
34
—
Conscious
—
2
6.1
138
15
0.2
Airway
Normal
4
12
129
14
0.9
Endotracheal
24
71
639
70
—
Tracheostomy
6
18
145
16
—
NI day
—
5
4–7.3
5
3–8
0.5