
Abstract
Introduction
Point-of-care ultrasound (POCUS) has an established role in the management of the critically ill. Information and experience of its use in those with COVID-19 disease is still evolving. We undertook a review of cardiac and thoracic ultrasound examinations in patients with COVID-19 on the intensive care unit (ICU). Our aim was to report key findings and their impact on patient management.
Methods
A retrospective evaluation of critically ill patients with COVID-19 was undertaken in three adult ICUs, who received point-of-care cardiac and/or thoracic ultrasound during the 2019–2020 COVID-19 pandemic. We recorded baseline demographic data, principal findings, change in clinical management and outcome data.
Results
A total of 55 transthoracic echocardiographic examinations scans were performed on 35 patients. 35/55 (64%) echocardiograms identified an abnormality, most commonly a dilated or impaired right ventricle (RV) and 39/55 (70%) scans resulted in a change in management. Nine patients (26%) were found to have pulmonary arterial thrombosis on CTPA or post-mortem. More than 50% of these patients showed evidence of right ventricular dilatation or impairment. Of the patients who were known to have pulmonary arterial thrombosis and died, 83% had evidence of right ventricular dilatation or impairment. 32 thoracic ultrasound scans were performed on 23 patients. Lung sliding and pleural thickening were present bilaterally in all studies. Multiple B-lines were present in all studies, and sub-pleural consolidation was present bilaterally in 72%.
Conclusion
POCUS is able to provide useful and clinically relevant information in those critically ill with COVID-19 infection, resulting in change in management in a high proportion of patients. Common findings in this group are RV dysfunction, multiple B-lines and sub-pleural consolidation.
Introduction
In December 2019, the first case of a novel coronavirus disease-19 (COVID-19), caused by the SARS-Cov-2 virus, was identified in Wuhan, China. 1 As of 11th December 2020, there were over 65 million cases worldwide with over 1.5 million confirmed deaths. 2 On the 4th December, 18,142 patients had been treated in UK critical care units.3,4
The management of those critically ill with COVID-19 has evolved since the start of the global pandemic in December 2019 but continues to present clinical, logistical, ethical and societal challenges. These include the difficulties inherent in physical examination and treatment posed by the need for personal protective equipment (PPE). There are also challenges associated with transfer of unstable, infectious patients for diagnostic imaging outside the intensive care unit. Thus, there has been great interest in point-of-care ultrasound (POCUS) and focussed echocardiography in this setting.
The role of focussed ultrasonography in critical care practice has become well established in recent years.5–7 In the United Kingdom, several critical care accreditation schemes and examination protocols have been developed over recent years including Focussed Intensive Care Echocardiography (FICE), Core Ultrasound in Intensive Care (CUSIC) and more recently a combined accreditation, Focussed Ultrasound in Intensive Care (FUSIC). 8 FUSIC incorporates focussed cardiac ultrasound, as well as basic thoracic and abdominal ultrasonography. In addition, more advanced accreditation in cardiac sonography is available, via the British Society of Echocardiography (BSE) or European Society of Intensive Care Medicine (ESICM).9,10 The FUSIC cardiac protocol involves visual assessment using 2D ultrasound of left and right ventricular size and function, presence or absence of pericardial fluid and presence or sonographic signs of hypovolaemia. The FUSIC lung module involves assessment of pleural sliding, alveolar interstitial syndrome, pleural effusion and consolidation. Thoracic ultrasound has a higher sensitivity and specificity than chest radiography at diagnosing interstitial syndrome and consolidation. 11 It also has the advantage of being available at the bedside to rapidly assess acutely unstable patients.
Focussed cardiac and thoracic sonography has already been used in the setting of critical illness associated with COVID-19 disease. Preliminary experience emerging from China and Europe described distinctive thoracic ultrasound findings: pleural thickening, focal, multifocal and confluent B lines, consolidation and very few pleural effusions.12–18 Echocardiographic features of COVID-19 have been published from small case series only and describe global or regional impairment of left ventricular systolic function, right ventricular impairment or dilatation and signs of pulmonary hypertension and myocarditis.19,20
NHS Lothian has two tertiary ICUs (Royal Infirmary of Edinburgh and Western General Hospital) and one district general ICU (St John’s Hospital), whose expanded critical care capacity peaked at 52 beds at the first wave of the COVID-19 pandemic. Point-of-care ultrasound is already well established in the care of our patients, with established education and governance structures to support this. We have previously reported our experience of focussed echocardiography in managing non-COVID-19 critically ill patients. 5 We set out to report our experience of using point-of-care ultrasound in a cohort of critically ill patients with COVID-19 disease and describe the principal findings and their impact on patient management.
Methods
Between 1st April 2020 and 30th April 2020, we undertook a retrospective review of electronic and paper records for all patients with COVID-19 admitted to the critical care units of the three regional adult critical care units in NHS Lothian to evaluate the use of POCUS. This study was reviewed as service evaluation by our local quality improvement team and therefore formal ethics review was not deemed necessary.
Patients were included if they either had COVID-19 disease confirmed by SARS-CoV-2 reverse transcriptase–polymerase chain reaction (RT-PCR), or in whom there was a strong clinical suspicion despite negative RT-PCR test, and if they received a bedside transthoracic echocardiogram or thoracic ultrasound examination during their critical care admission. Our institutions did not have access to SARS-CoV-2 antibody testing during the study period although it subsequently became available. Echocardiograms were either focussed studies undertaken following the FICE/FUSIC protocol or BSE studies performed by accredited sonographers or under their supervision. 8
For all patients included in the study, we collected demographic information (age, gender, admission diagnosis, APACHE II and presence of pre-existing cardiovascular disease), indication for scanning, level of training of sonographer, image quality, significant findings and changes in management resulting from these. We also recorded data on ventilatory and cardiovascular management, duration of treatment, ICU and hospital outcome, cause of death, and post-mortem examination findings where known. Focussed echocardiography findings were reported as per the FICE protocol, with binary yes/no answers to whether there was significant LV impairment on visual assessment, LV dilatation (LV internal diameter in diastole in the parasternal long axis window more than 60 mm), significant RV impairment on visual assessment, RV dilatation (defined by FUSIC as RV basal diameter more than 2/3rd the basal diameter of the LV), presence of pericardial effusion, evidence of hypovolaemia or presence of pleural fluid. 8 In our institution, all echocardiography or ultrasound scans undertaken on the ICU are documented electronically either on the Electronic Patient Record or on the GE Echopac system using a prespecified reporting template. Comprehensive echocardiographic studies were reported in line with the British Society of Echocardiography (BSE) minimum dataset. 9 Thoracic ultrasonography was undertaken following the Intensive Care Society FUSIC protocol which includes performing a scan with the probe placed at the upper, lower and postero-lateral points bilaterally. Data were collected on the presence or absence of lung sliding, pleural thickening, more than 2 B lines per area, consolidation and pleural effusion. 8 To minimise the risk of in-hospital transmission of COVID between patients by contact with ultrasound equipment, we complied with standard COVID infection control policies in our department. This involved enhanced PPE (including FFP3 mask, fluid resistant full length gown, face shield and gloves) for the sonographer, as well as the use of ultrasound machines dedicated to scanning confirmed or suspected COVID patients. The ultrasound machine was decontaminated after each scan using a 1000 ppm chlorine solution.
Results
Patient demographic information and indication for scan.
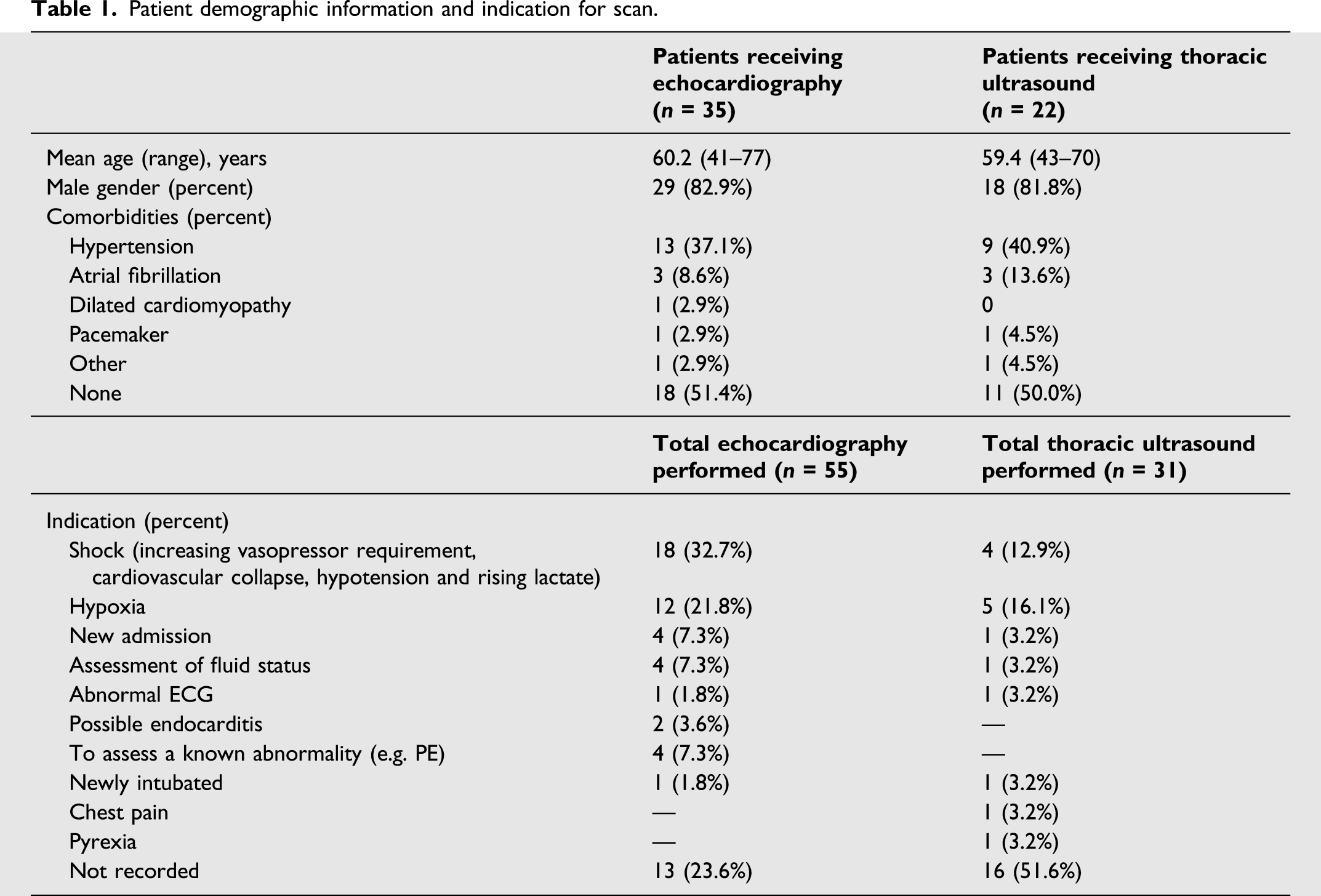
Echocardiography
Overall 35 (64%) scans identified some abnormality. The most common findings were significantly dilated or impaired right ventricular (RV) function (24 scans, 44%), followed by evidence of hypovolaemia (12 scans, 22%), evidence of pericardial fluid (8 scans, 15%), significant left ventricular (LV) impairment on visual assessment (5 scans, 9%) and pleural fluid in (1 scan, 1.8%). Additional findings included 5 (9%) scans showing echogenic structures in the right atrium; however, only 2 of these were shown to be pulmonary arterial thrombosis on CTPA. Seven patients underwent a full echocardiographic examination. Of these scans only one scan contradicted the focussed scan: an echogenic structure in the right atrium was identified as an anatomical variant.
Physiological and outcome data for patients undergoing echocardiography.
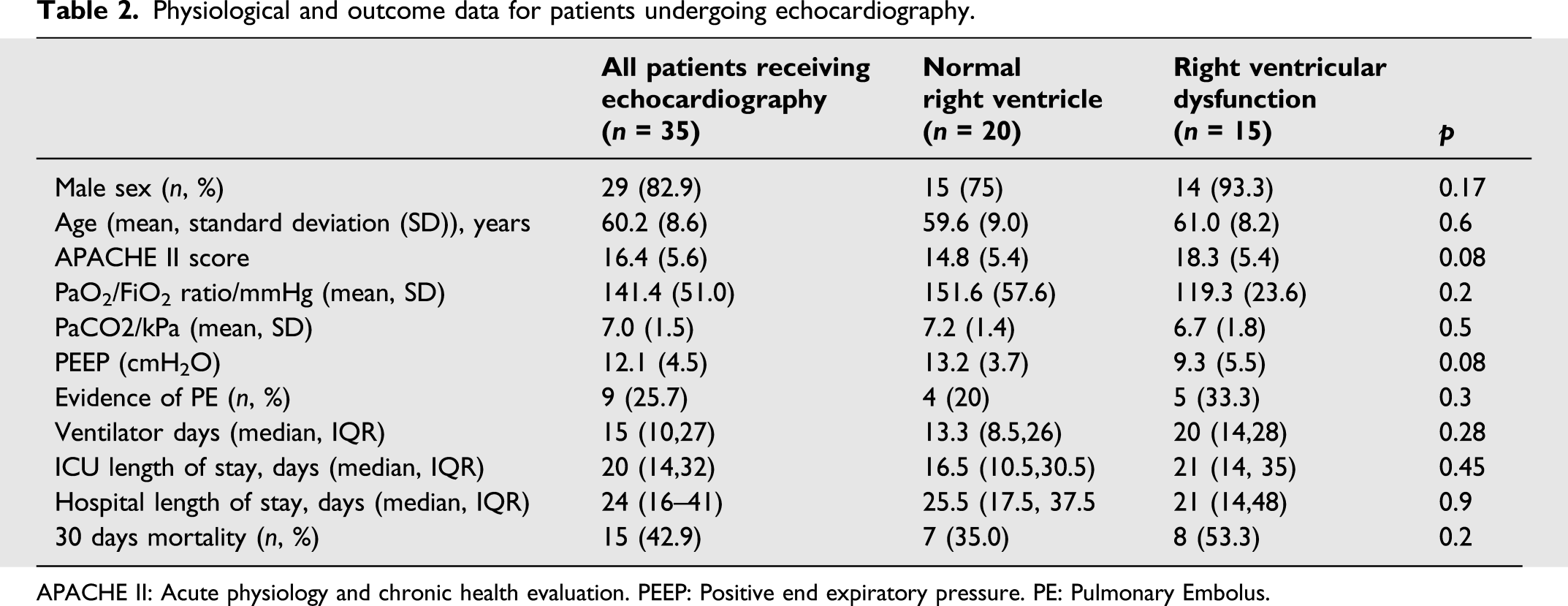
APACHE II: Acute physiology and chronic health evaluation. PEEP: Positive end expiratory pressure. PE: Pulmonary Embolus.
From the 9 patients (26%) who were found to have pulmonary arterial thrombus on CTPA or at post-mortem, 6 of them had died. Five out of these 6 patients (83%) had evidence of right ventricular dilatation or impaired function. All patients that underwent post-mortem examination or autopsy (n = 4) were found to have right ventricular dilatation and pulmonary arterial thrombosis, including one who had a normal echocardiogram and a normal CTPA prior to their death.
Four (11%) patients showed evidence of left ventricular impairment. At the end of the study period, two (50%) of these patients had died and two (50%) patients remained alive.
Echocardiogram findings contributed towards a change in management in 39 (70%) scans. The most frequent management change documented was requesting further imaging which included CT pulmonary angiography, formal echocardiogram and CT abdomen. Other management decisions included alterations to fluid management with either additional fluid administration or removal of fluid using continuous veno-venous haemodialysis (CVVHD). (Figure 1). Change in management following focussed echocardiogram.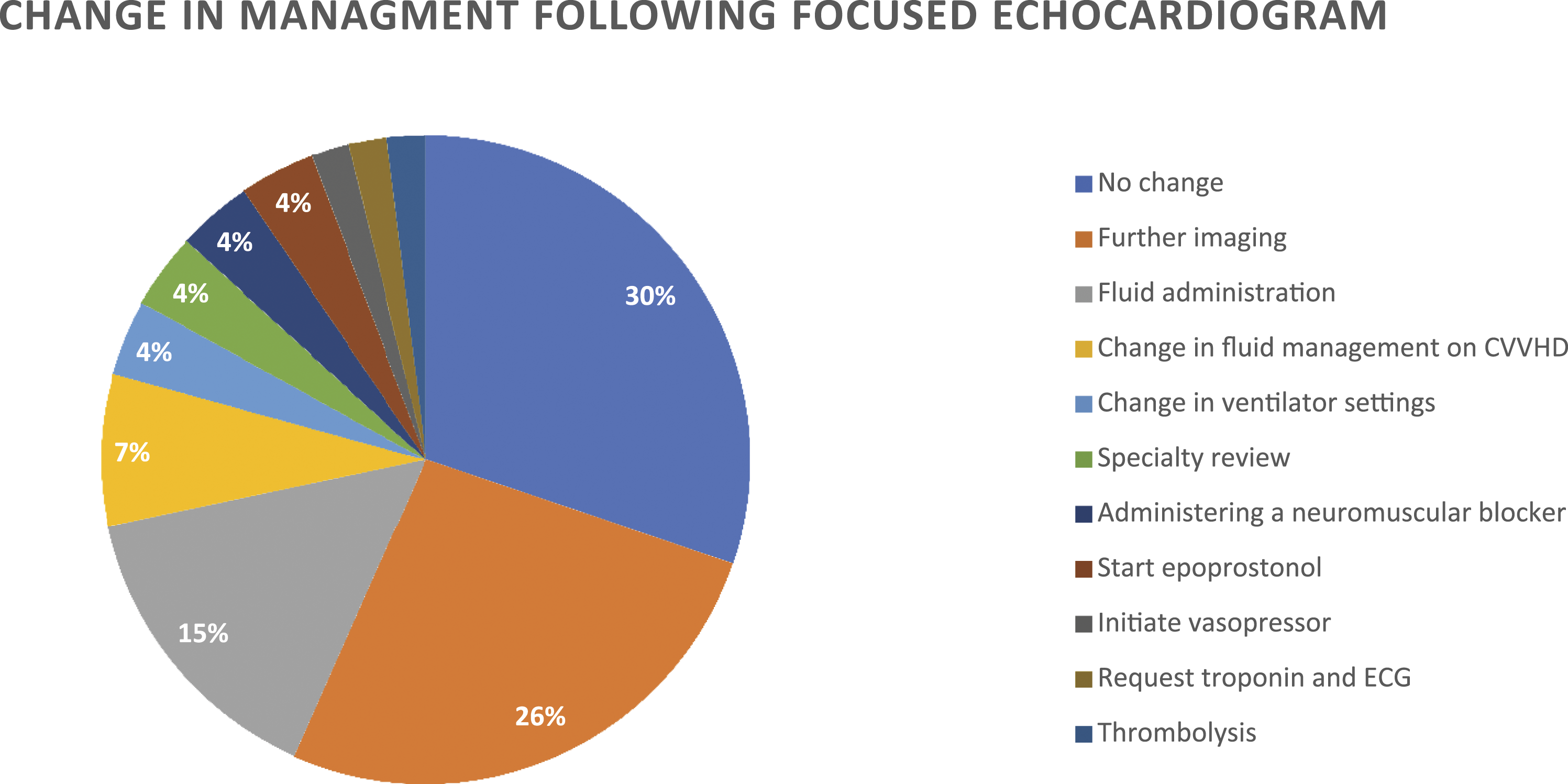
Lung Ultrasound
Both lung sliding and pleural thickening were present bilaterally in all 31 lung ultrasound studies. B-lines were present in all 31 studies. Twenty-two (71.0%) studies had multifocal B lines in all areas.
Sub-pleural consolidation was bilateral in 23 (74.1%) studies, unilateral in 6 studies (19.4%) and not present in 3 (9.7%) studies. Pleural effusion was present in only 3 studies (9.7%) performed on 3 separate patients. Thoracic ultrasonography led to a change in management in 11 studies (35.5%). (Figure 2). It was particularly useful in ruling out other causes of hypoxia such as pneumothorax, new consolidation or one-sided lung ventilation due to migration of the endotracheal tube. A decision was made to prone four patients after thoracic ultrasound could demonstrate no cause for hypoxia other than severe COVID-19 disease. Two patients had classical appearances of COVID-19 and so were treated as such until their RT-PCR result was available. Change in management following thoracic ultrasound.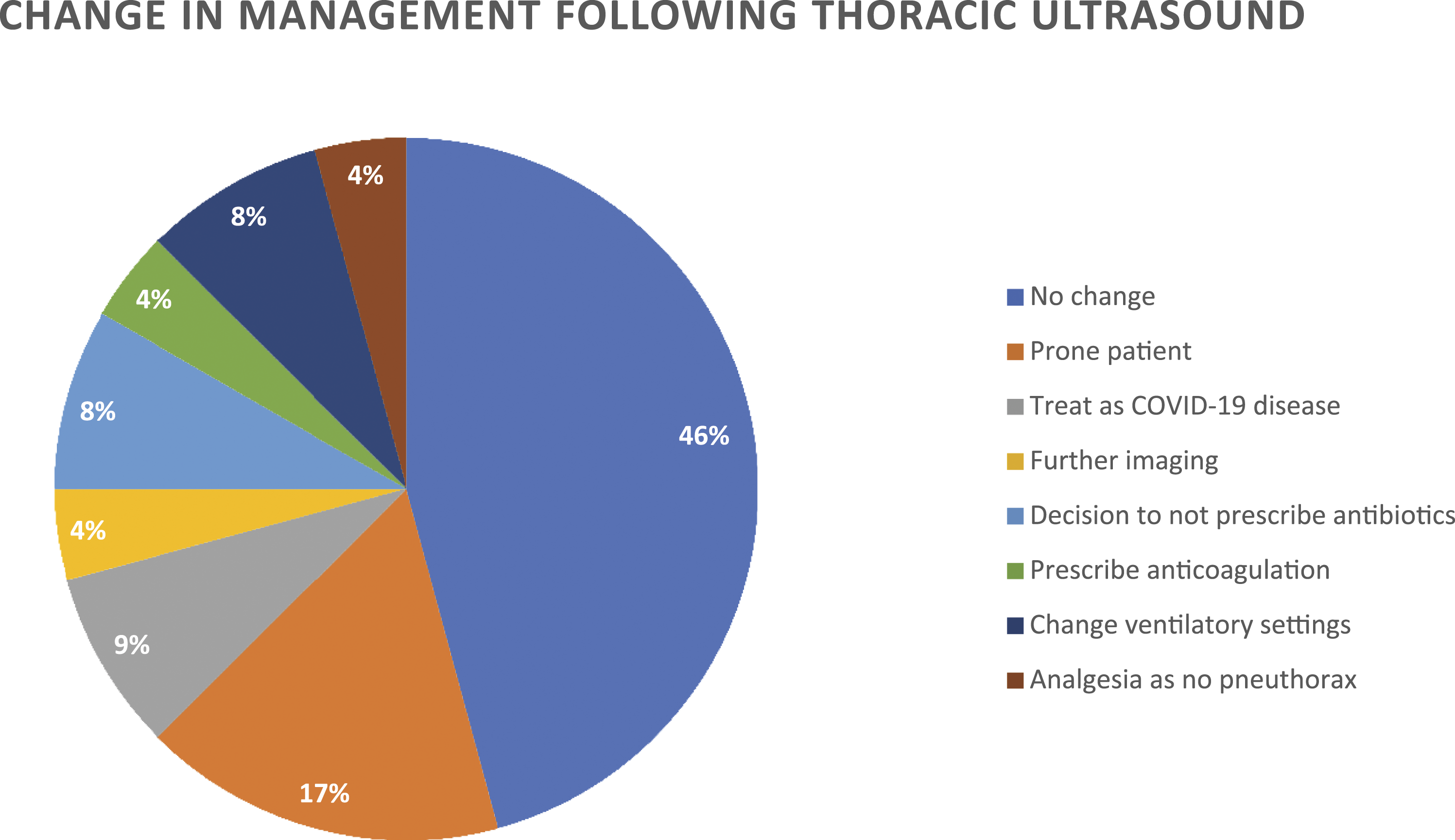
Discussion
We report the first combined study of focussed echocardiography and thoracic ultrasound in critically unwell patients admitted to ICU with confirmed or suspected COVID-19 disease. Echocardiogram abnormalities were demonstrated in 64% of scans and contributed towards a change in management in 70% of all scans undertaken. Common changes in management made on the basis of information gained from POCUS included fluid therapy, further imaging and commencing new therapies such as vasoactive drugs or thrombolysis.
The most common abnormality found on echocardiogram was right ventricular dilatation or significantly impaired function which was seen in 44% of scans, in contrast to a previous study within the general ICU population that demonstrated only 7% of scans identified right ventricular dilatation or impaired function. 5 All thoracic ultrasound scans demonstrated the classical reported findings of COVID-19 disease including pleural thickening and widespread B lines. A large proportion of scans also demonstrated sub-pleural consolidation but very few had any evidence of pleural effusions, similar to other recent reports.12–16 Other studies have shown that sonographic appearances appear to correlate well with the described thoracic CT imaging in COVID-19 and with the advantages of being portable, no radiation exposure and easily repeatable, thoracic ultrasound is an important tool in the management of COVID-19 disease.13,14,17
COVID-19 disease has been reported to cause pulmonary and vascular inflammation with impaired gas exchange, increased pulmonary vascular resistance and the presence of pulmonary thrombosis. There has been a high incidence of venous thromboembolic complications reported with COVID-19 with cohort studies finding 35–45% of ICU patients with COVID-19 had CT evidence of pulmonary arterial thrombosis.21–23 This is significantly higher than the previously reported rate of thromboembolic events in critically unwell patients of 5–15%. 23 25% of patients in this series were found to have pulmonary thrombosis in either CTPA or post-mortem, and more patients with RV dysfunction were found to have radiological or post-mortem evidence of pulmonary thrombosis although this was high in both groups and not statistically significant. Not all patients in our series underwent computed tomography pulmonary angiography (CTPA) or post-mortem examination and it is therefore possible some cases were missed. We found fewer cases of left ventricular impairment in COVID-19 patients in comparison to the non-COVID-19 critically ill patients in our previously published cohort who were assessed by point-of-care echocardiography using the same FICE/FUSIC protocol. 5 We also found no cases of cardiomyopathy or myocarditis, which had been described elsewhere in the literature.19,20
In this study, the presence of RV abnormalities was associated with a higher admission APACHE II and therefore may reflect more severe disease. RV dysfunction did not seem to be associated with differences in oxygenation or pCO2. A trend towards lower PEEP was observed, and this finding was of uncertain significance. It may have reflected a reluctance to use higher levels of PEEP due to haemodynamic compromise associated with RV dysfunction or could also be that some of these patients had derecruited and had higher hypoxic pulmonary vasoconstriction and/or higher pulmonary vascular resistance due to atelectasis.
The key limitations of this study were that it is a retrospective observational study of a relatively small number of patients. The results should therefore be interpreted with caution. It is possible that those patients who clinicians were more concerned about, had a higher severity of illness or were deteriorating had therefore had more scans performed during their admission. This may have increased the incidence of findings and mortality recorded. The clinicians performing the scans and reporting the findings were not blinded to whether the patient had COVID-19, and it is possible that this affected the likelihood of certain findings being reported. All clinicians were trained to a minimum of FICE or CUSIC level training and a prespecified template was used for reporting.
However, we report experience of both echocardiography and lung ultrasound in cohort of patients critically unwell with COVID-19 from 3 ICUs and report the typical findings and utility of POCUS in this setting. Experience with POCUS in this setting is still evolving, and COVID-19 disease appears to have distinctive features which are different from the general critically ill population.
In conclusion, we have shown that echocardiography and thoracic ultrasound is able to provide clinically useful information which can aid decision-making and result in changes in management. Right ventricular dilatation and impairment predominates over the left ventricular impairment more typically seen in an unselected ICU population. We found a high incidence of pulmonary thrombosis diagnosed on CTPA or at post-mortem. Typical lung ultrasound findings are large numbers of confluent B-lines and sub-pleural consolidation, consistent with other preliminary work.
Footnotes
Author’s Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Helen Jordan, Hannah Preston, Hugh Gifford, David Hall and Michael Gillies. The first draft of the manuscript was written by Helen Jordan and Hannah Preston, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and material
All analysed data are reported in the manuscript. Anonymised data can be shared on request.
Take Home Message
Echocardiography and thoracic ultrasound is able to provide clinically useful information which can aid decision-making and result in changes in the management of patients with COVID-19 disease in intensive care. Right ventricular dilatation and impairment predominates over left ventricular impairment and there is a high incidence of pulmonary thrombosis in comparison to the unselected ICU population.