
Abstract
Point-of-care ultrasound (POCUS) is the use of bedside ultrasonography by the treating clinician, incorporating those images into direct clinical decisions. While there are a number of different techniques and training pathways in this relatively new modality, there has been little discussion around the logistics of integrating POCUS into the standard critical care “business day” of ward rounds, procedures and meetings. This article explores some of these aspects and presents data from an online survey of POCUS practitioners.
Introduction
Imaging technology is ubiquitous in the care of the critically ill, with ultrasound standing out due to its real-time nature and absence of radiation risk. Termed “point-of-care ultrasound” (POCUS) and encompassing such techniques as focused abdominal sonography in trauma and focused cardiac ultrasound, it is now possible to rapidly deploy at the bedside of a deteriorating patient, with an increasing evidence base supporting this strategy.1,2
Since the 2011 consensus statement on the use of POCUS in critical care, 3 a number of national and professional societies have developed various training programmes to deliver and support colleagues in acquiring, developing and maintaining these skills. In the UK, the Intensive Care Society has developed focused intensive care echocardiography and core ultrasound in intensive care covering focused echo and POCUS, respectively. 4 Despite this, barriers remain to the seamless delivery of POCUS 24/7. 5
However, the increasing number of accreditation programmes and training courses means that more clinicians are developing this skillset. Coupled with technological advancement in developing portable and handheld devices, intensivists and other acute physicians are increasingly able to perform diagnostics in the critically ill without the delays/risk associated with patient transfer.
The best time to perform a POCUS examination is when the patient requires it. The convenience does come at the cost of taking up clinician time and interrupting the workflow of the day and ward round; this interruption is particularly relevant since not all clinicians are currently competent in POCUS. With clinicians’ time increasingly being stretched, a way of balancing the inherent benefits of POCUS and drawbacks is crucial. How does one fit bedside imaging into daily practice and the ward round? The old intensive care unit (ICU) adage of “just because you can, doesn’t mean you should” still rings true.
Methods
The authors, accredited POCUS practitioners and educators, informally surveyed their clinical community regarding their current practice. A poll was also conducted via Twitter over a one-week period, where individuals who used POCUS on their ICUs were asked about their preferred method of incorporating it.
The poll was titled “how would you implement POCUS in your ICU ward rounds?” and had three options:
After rounds During rounds Other.
With the option for free text comments.
Results
The Twitter poll was sent to the followers (approximately 4000 individuals) of one of the authors (OO). On hundred and sixty-four individuals engaged in the tweet, of whom 132 voted. Voters were from a varied international background: American, Australian, Canadian and UK critical care practitioners from a broad range of unit sizes.
Forty-three percent of individuals perform POCUS after the ward round; 45% perform POCUS during the ward round (Figure 1). The remaining 12% voted “other” and responded in a variety of ways, most using a combination of both techniques as they saw fit.
How respondents utilised POCUS.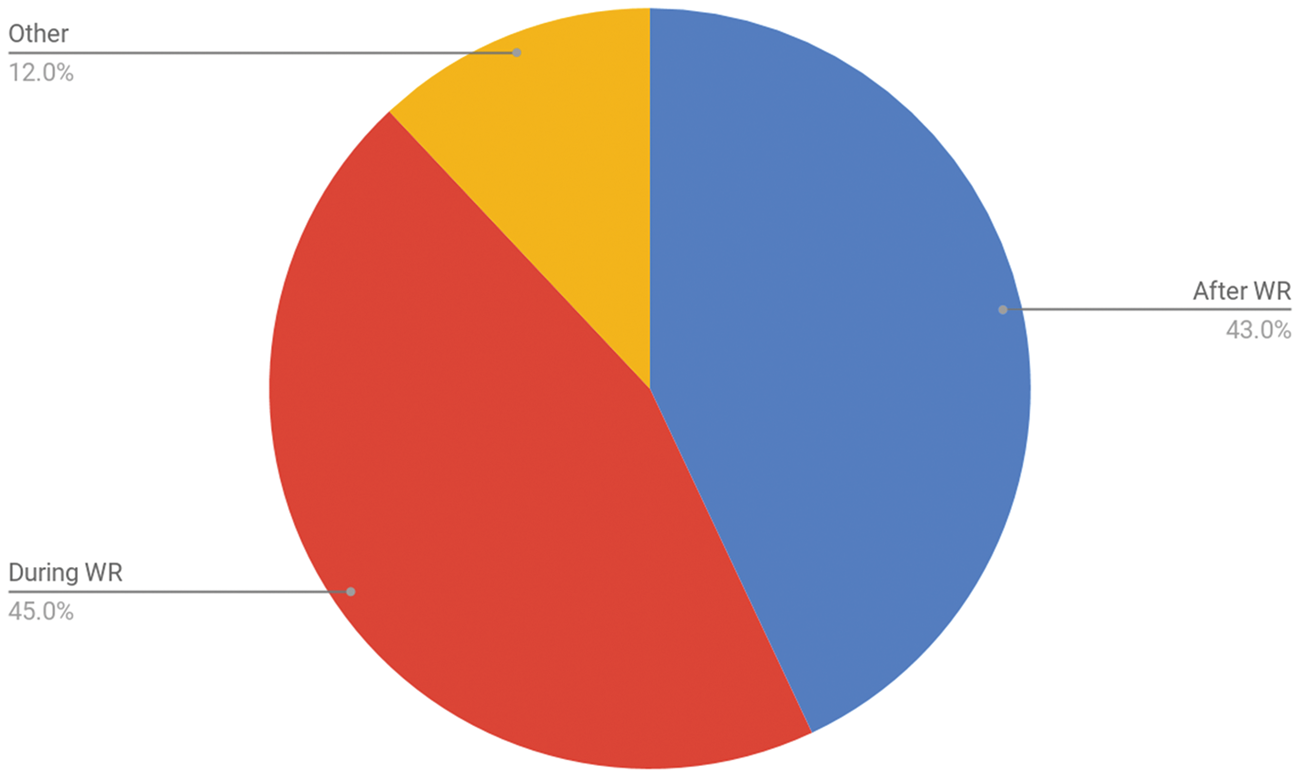
Three main themes emerged:
Performing the scan post-ward round. This treats the ultrasound scan as a task to be performed outside of the ward round. Patients who require scanning are identified during bedside reviews; these scans are performed and interpreted, with the results available for action by the evening ward round or night review. The asynchronous scan by a dedicated member of the team. Some ICUs are fortunate enough to have one or more dedicated POCUS practitioners in the form of a consultant who has a day scheduled to scanning, clinical fellows/junior doctors training in ultrasound or a dedicated sonography technician team.
These POCUS practitioners will routinely scan patients on the unit who present with certain indications or upon request by clinicians.
Scanning at the bedside during the round. In this variant, the assessing clinician(s) are the POCUS practitioners. The machine follows the ward round, with real-time scanning while the patient is reviewed by the team.
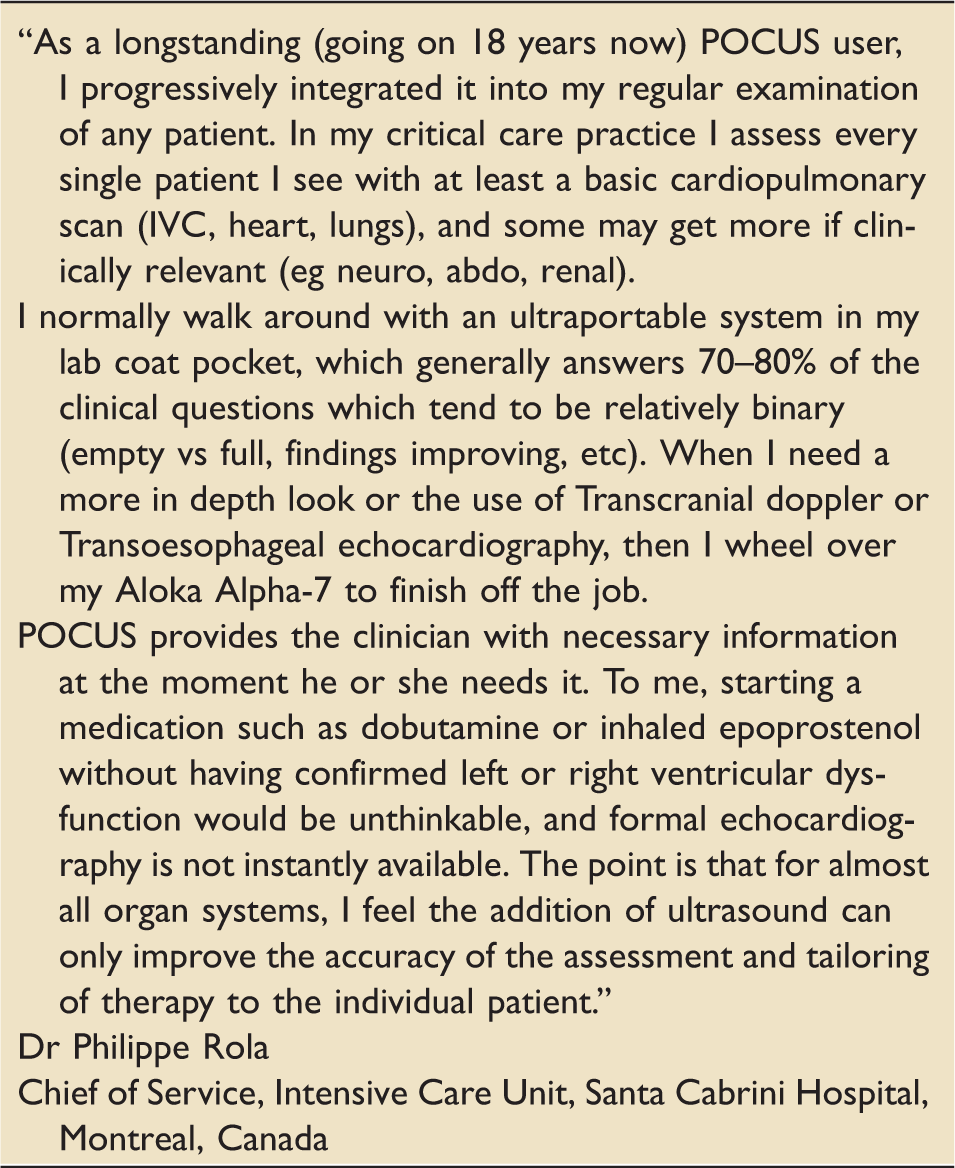
A description of daily practice from an advanced POCUS practitioner.
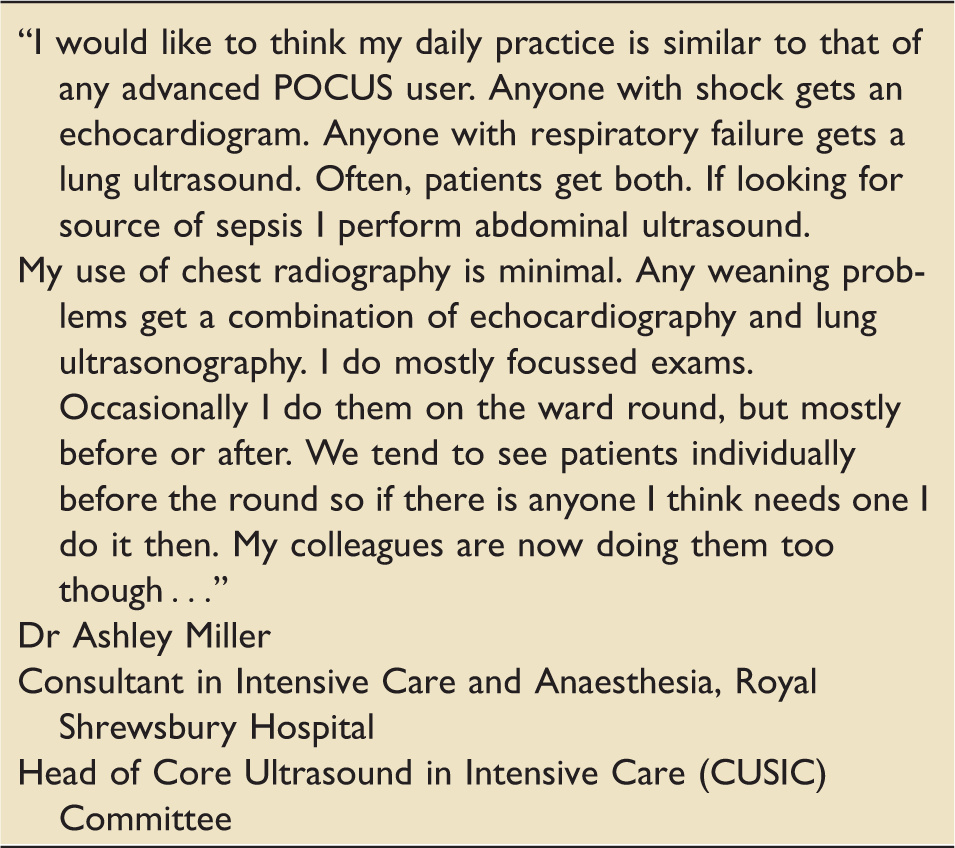
A second description of advanced POCUS practice.
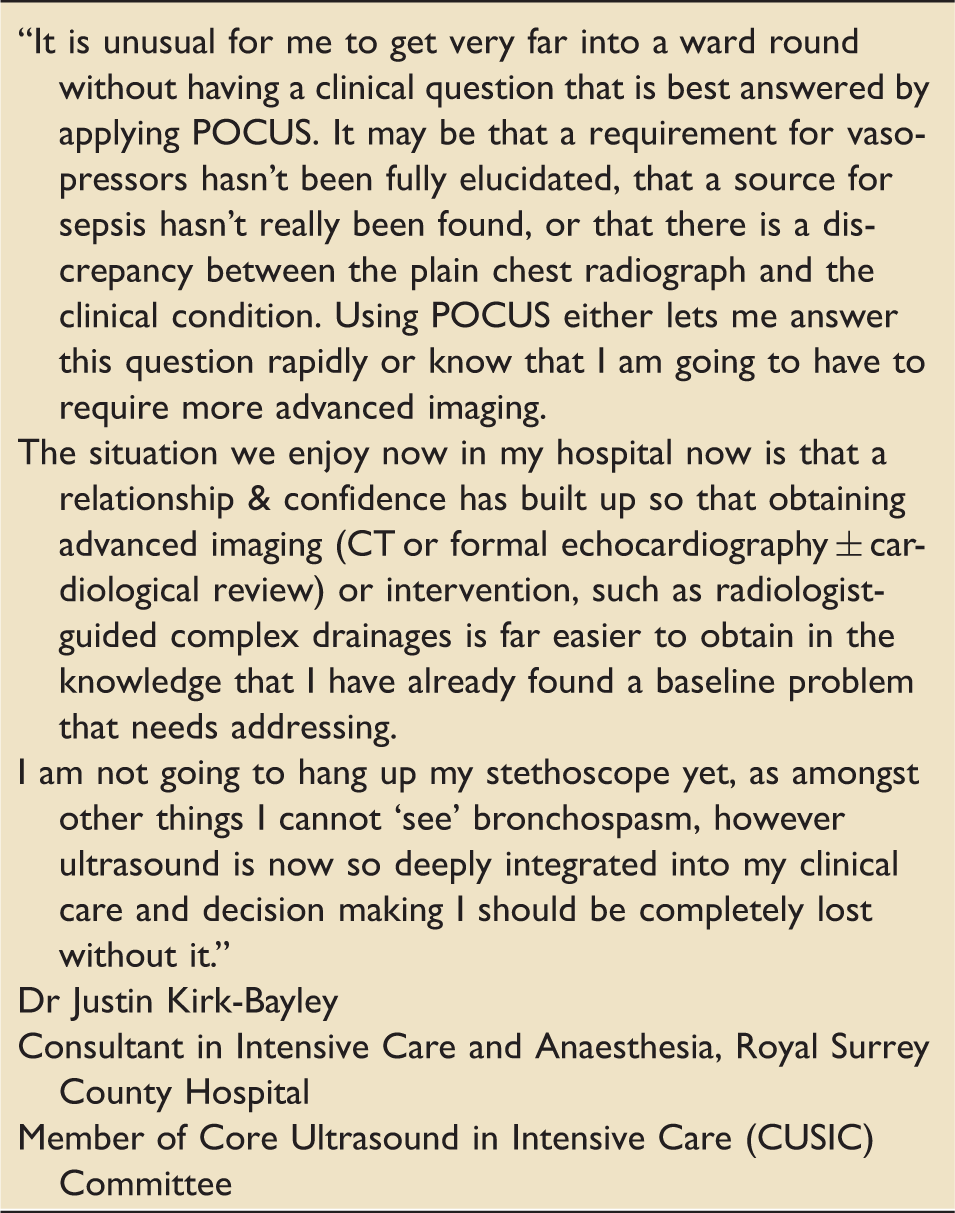
A third description of advanced POCUS practice.
Discussion
In resuscitation and emergent scenarios, POCUS can be an immensely useful skill for health professionals in urgent care, with significant potential benefit to patients.
This article focuses on incorporating POCUS into the ICU ward round, where limitation of training opportunities and impact on efficiency continue to challenge its implementation. Echocardiography, be it focused or detailed, has been gradually introduced in many ICUs in the UK and the other modules of POCUS should be no different. The key to this is to increase the mass of healthcare professionals performing bedside POCUS to the point where every ICU has access to a practitioner at all times.
Strengths and weaknesses of different approaches to POCUS.
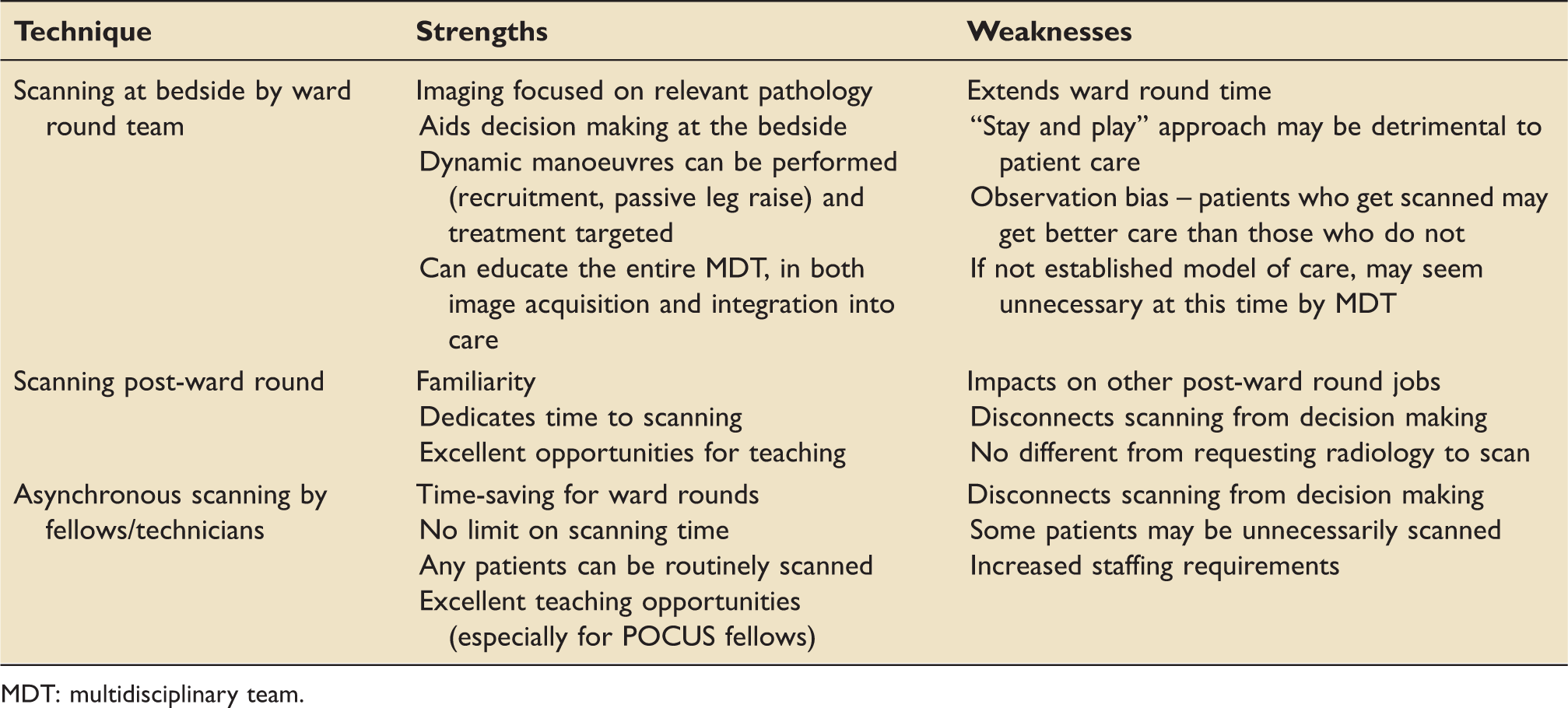
MDT: multidisciplinary team.
Reasons why POCUS scans are not performed immediately.
On one hand, specific questions on the ICU ward round can be answered immediately with the first approach, examples of which include the presence of pneumothorax, hypovolaemic volume status and hydronephrosis. In these situations, waiting until the end of the ward round (or for technicians who may be busy scanning elsewhere) can delay recognition of pathology with potential deleterious effects on patient care.
A further aspect is the identification of the “best” practitioner available to perform the scan; is it more beneficial (less harmful) to wait for a detailed scan by an experienced technician rather than to perform a focused scan to address the specific issues at hand? By prioritising the POCUS scan as an actual task rather than an add-on “for interest” only, the later approach will embed POCUS more firmly within the ICU working culture and consolidate its strengths and value over time.
While there are multiple international recommendations on “how” to scan, there are no recommendations that currently exist on “when” to scan. The first article to address some aspects of this has recently been published by the Mayo Clinic ICU; 6 this was a small randomised rontrol trial comparing two different approaches to incorporating POCUS in the assessment of the acutely unwell patient. Our article is the first in our knowledge to address the question of POCUS during intensive care rounds.
It is the authors’ opinion that scanning in real time while assessing the patient on the ward rounds is best practice. The ultrasound machine should be available at the bedside during the round, and clinical conundrums which POCUS can solve can be assessed and answered immediately leading to dynamic changes in bedside management. If the ethos of intensive care is delivering essential interventions in a timely manner, the immediacy of POCUS would allow that. The results of the survey echo our thoughts with practitioners using POCUS in exactly that manner.
Future directions in this area revolve around POCUS timing and its impact on patient-centred outcomes. In light of recent data from the MIMIC 3 database 7 suggesting that echocardiography within 24 h of admission with septic shock improves mortality, and NHS England’s Seven Day Services Clinical Standards (Standard 5) released in September 2017 that mandates critically ill patients should have an echocardiogram within an hour, 8 we believe formal trials addressing this issue would be very helpful.
In summary, this article highlights several modes of applying POCUS into daily ICU care. Ultimately, different ICUs adopt different techniques based on staffing, working shift patterns, experience and availability of POCUS practitioners, number of ICU/HDU beds, workload, ready access to a suitable ultrasound machine. There is unlikely to be a single best method and the most practical and realistic way of incorporating POCUS into the working culture, training and patient care on the ICU is probably a combination of all three.
Footnotes
Acknowledgement
The authors would like to thank Drs Rola and Miller for contributing their vignettes to this article.