
Abstract
In this study we report 5-year outcomes for patients who received intermittent haemodiafiltration for Acute Kidney Injury (AKI) between 2010 and 2014 in a small Scottish Intensive Care Unit (ICU). Dialysis independence and mortality at ICU discharge, 30 and 90 days, one and five years were determined. There were 1496 admissions to ICU during the study period. 12% of patient admissions required Renal Replacement Therapy (RRT). 56.3% of patients survived to ICU discharge and all were RRT independent at ICU discharge. 30 day, 90 day, 1 year and 5 year survival was 52.3%, 50.6%, 46.6% and 30.7% respectively. By 5 years, 2 patients had developed end stage kidney disease.
Introduction
Worldwide, continuous RRT are usually preferred as treatment for AKI in critically ill patients, due to more gradual fluid removal and a theoretical lower incidence of hypotension than with intermittent RRT. Despite common practice favouring continuous therapies and numerous studies exploring this issue, there is no compelling evidence that such therapies improve outcomes. 1 Continuous therapies can place a greater burden on staff and finite resources, National Institute for Health and Care Excellence has recently published guidance for RRT during the covid-19 pandemic which summarise the varying resources utilised with each modality. 2
Within Scotland, during the pandemic, to optimise resources, a number of ICUs have recently switched to intermittent RRT. 3 There may be some concern that changes to RRT modality may affect long term outcomes. In this study we report 5-year outcomes for patients who received RRT for AKI between 2010 and 2014 in Dumfries and Galloway Royal Infirmary (DGRI), a small rural ICU in Scotland, where intermittent haemodiafiltration for 4-6 hours daily is routinely practiced.
Methods
This was a retrospective observational study. All patients admitted to ICU in DGRI from 1st January 2010 to 30th November 2014 were identified using the Scottish Intensive Care Society WardWatcher. Patients who underwent RRT for AKI were identified using electronic records. If a patient was admitted more than once only their first admission was included. Patients with end stage kidney disease were excluded. Presence of co-morbidities was assessed from baseline and diagnostic coding data were available from WardWatcher. Baseline creatinine was recorded as the lowest available value in the 6 months preceding ICU admission. Severity of illness was recorded using Acute Physiology and Chronic Health Evaluation (APACHE) II scores. Dialysis independence and mortality at ICU and hospital discharge, 30 and 90 days, one and five years was determined by electronic medical record review in May 2020.
The local Caldicott guardian granted permission for this study and waived formal ethics application. Data were tested for normal distribution using a Kolmogorov-Smirnov test and visual inspection of boxplots. Normally distributed data are presented as mean (± standard deviation), non-parametric are presented as median (interquartile range, Q1–Q3). Analysis was conducted using SPSS version 27.
Results
There were 1496 admissions to ICU during the study period. RRT was required in 179 (12%) admissions. After exclusion of 3 patient-episodes for those with multiple admissions, 176 patient admissions were included in the analysis. 102 (58%) were male, mean age was 67.0 (±14.4) years. 133 (75.6%) patients had one or more comorbidity. 168 patients (95.5%) had an APACHE II score completed during their admission with a mean score of 23.7 (±8.4). Using the APACHE II score mean predicted probability of mortality was 48.3 (± 24.3)%; 56.3% of patients survived to ICU discharge, 30 day, 90 day, 1 year and 5 year survival was 52.3%, 50.6%, 46.6% and 30.7% respectively. Full baseline characteristics, survival data and renal function at 5-year follow up are presented in Table 1. All patients were RRT independent at ICU discharge; however two patients were RRT dependent by 5 years (Figure 1).
Patient characteristics and survival data.
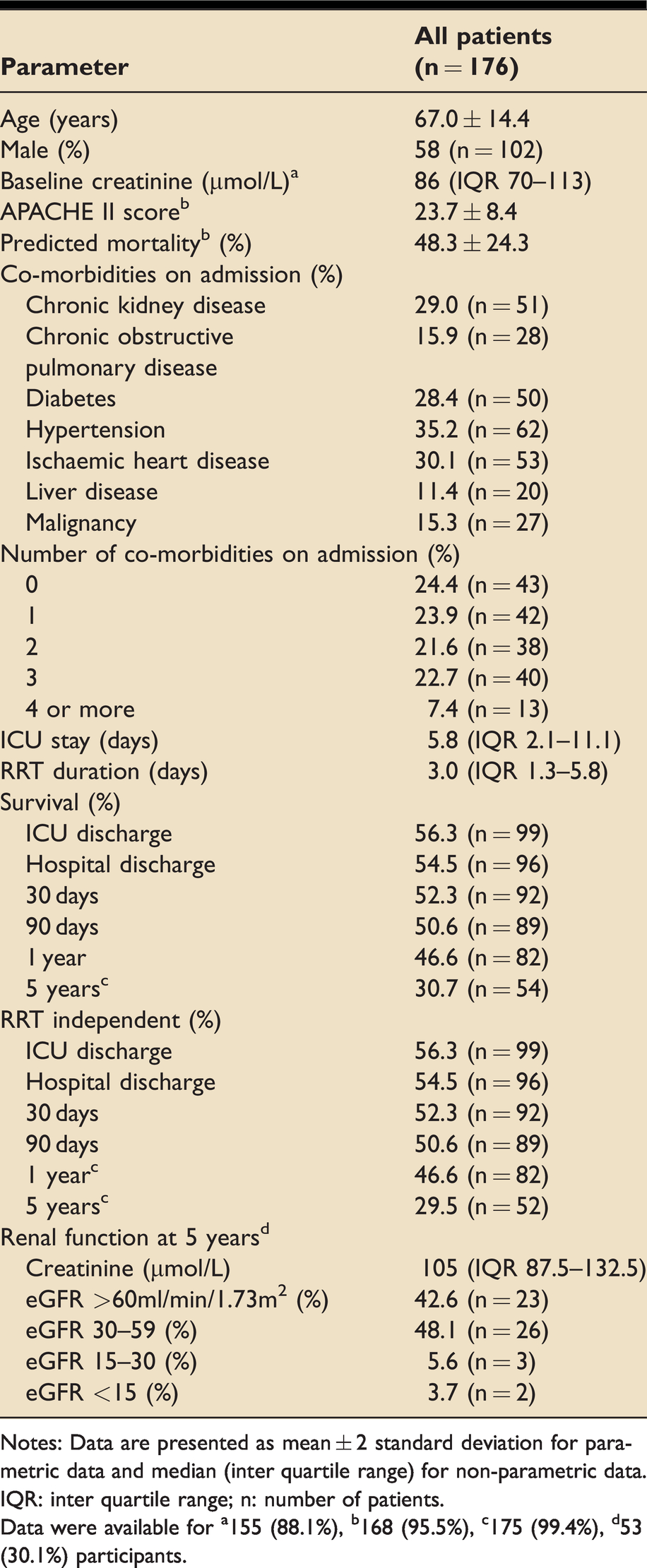
Notes: Data are presented as mean ± 2 standard deviation for parametric data and median (inter quartile range) for non-parametric data.
IQR: inter quartile range; n: number of patients.
Data were available for a155 (88.1%), b168 (95.5%), c175 (99.4%), d53 (30.1%) participants.
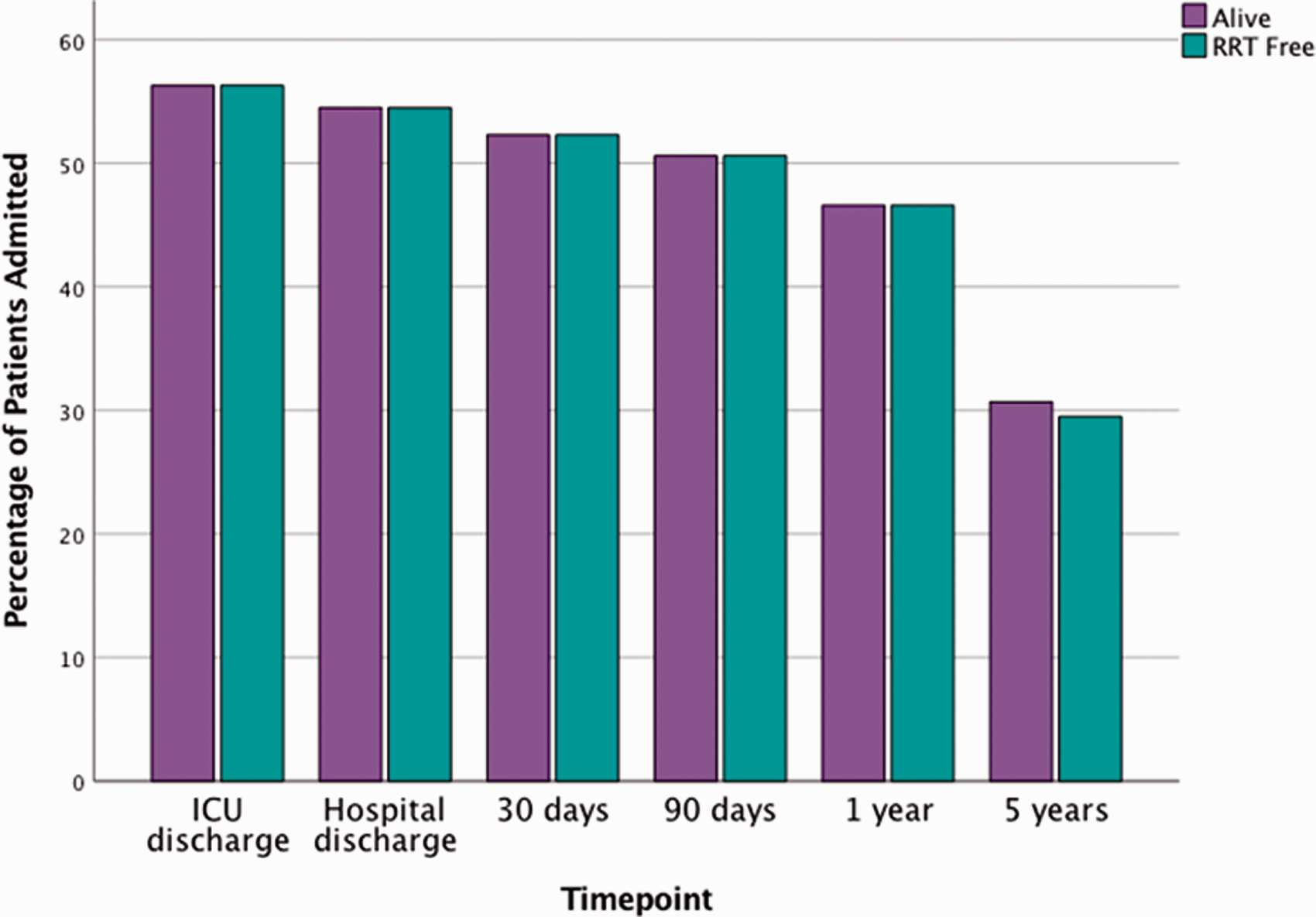
Bar chart showing percentage of patients surviving and those free of RRT following their AKI episode.
Discussion
Mortality is high amongst patients admitted to ICU who require RRT for AKI. The published literature demonstrates a crude in-hospital mortality rate of 44-79% amongst this patient group.4–7 In our study 43.7% of patients died whilst in ICU, which was in line with the standardised predicted mortality calculated using APACHE II scoring (predicted mortality 48.3 ± 24.3%). In Scotland, the Intensive Care Society Group publishes annual audit data which confirm that our rates of RRT (12%) and our standardised mortality ratios, are in line with national averages for the study period. 3
A 2012 audit of Scottish ICUs revealed the majority of units within Scotland (15 of 18) favoured continuous RRT strategies. 8 This may be due to a perception that continuous therapies offer haemodynamic or renal survival advantage over intermittent therapies. However, a 2002 meta-analysis found no evidence to support this, 9 a finding confirmed in a large multicentre observational study and supported by international guidelines.1,10 Intermittent haemodiafiltration is the standard RRT used in our unit. Renal survival was good within our study with 50.7% of survivors having an Estimated Glomerular Filtration Rate (eGFR) greater than 30 ml/min/1.73 m2 five years after their ICU admission. Despite the single centre observational nature of this study, our results may offer some reassurance to similar centres that have switched from continuous to intermittent therapies in view of demands placed upon them during the unprecedented pressures of the covid-19 pandemic.
Conclusion
In our study, in keeping with national data, 43.7% of patients requiring RRT for AKI did not survive to ICU discharge. In survivors, long term renal survival was excellent – there was no evidence to suggest intermittent RRT had a negative effect on renal or survival outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.