
Abstract
Objective
This study was performed to determine the association of D-dimers measured at the time of admission with the development of acute kidney injury (AKI) in pregnant women.
Methods
We retrospectively analyzed the data of 625 women who developed AKI and 628 normal pregnant women admitted to our hospital from January 2014 to December 2018. The primary endpoint of the study was the development of AKI in pregnant women, and the secondary endpoint was the development of dialysis and death in women with AKI. Univariate and multivariate analyses were conducted.
Results
The D-dimer concentration was significantly higher in patients with than without pregnancy-related AKI (PR-AKI). Multivariate logistic regression showed that a D-dimer concentration of >1108 ng/mL was an independent predictor of PR-AKI. The area under the curve of the D-dimer concentration as a prognostic indicator of PR-AKI was 0.652 (95% confidence interval, 0.622–0.683), that for patients with PR-AKI undergoing dialysis was 0.819 (95% confidence interval, 0.709–0.928), and that for patients who died was 0.828 (95% confidence interval, 0.670–0.986).
Conclusion
The D-dimer concentration is significantly associated with the development of AKI in pregnant patients and may increase the risk of dialysis and death in women with AKI.
Keywords
Introduction
Pregnancy-related acute kidney injury (PR-AKI) is an important obstetric complication that is associated with significant maternal and fetal morbidity and mortality.1–3 The incidence of PR-AKI was substantially reduced in developed and developing countries by the end of the 20th century; however, it remains unacceptably high. Moreover, a seemingly increasing incidence has been seen in the United States and Canada. This outcome may be attributed to older age and more pregnancies in patients with hypertensive disorders.4,5 Thus, PR-AKI remains an urgent public health problem.
Several renal biomarkers for early diagnosis of AKI have been studied in different clinical settings. However, their accuracy is controversial and their clinical application is limited. 6 Clinically, the diagnosis of AKI is mostly determined by the serum creatinine concentration and urine output. Thus, more practical renal markers are still required.
Increased hypercoagulability throughout pregnancy has been seen under physiological conditions. Moreover, according to previous studies, pregnancy complications such as preeclampsia and HELLP (hemolysis, elevated liver enzymes, low platelet count) syndrome, which may be major causes of PR-AKI,4,7 are associated with a more evident hypercoagulable state than in normal pregnancy. 8 Consistently, the D-dimer concentration is increased during pregnancy.8–10
D-dimers are a specific breakdown product of cross-linked fibrin and are commonly used in the diagnosis of pulmonary embolism and venous thromboembolism.11,12 A high plasma D-dimer concentration has been identified as a prognostic factor in several malignancies, joint infection, rheumatoid arthritis, and critical illness. The inflammatory response plays an important role.13,14 However, the effect of an elevated D-dimer concentrations on patients with PR-AKI has not been reported. In this study, we investigated the correlation between the D-dimer concentration and PR-AKI and evaluated the prognostic value of the D-dimer concentration for dialysis and death in patients with PR-AKI.
Methods
Study population
This case-control, retrospective study was conducted at the obstetrics department of Zhongnan Hospital of Wuhan University. Pregnant women from January 2014 to December 2018 were reviewed. Most were hospitalized for childbirth, and some were hospitalized for the occurrence of complications while giving birth in the hospital. This study protocol was approved by the Ethics Committee of Zhongnan Hospital of Wuhan University. All patients provided informed consent for participation in the study.
The inclusion criteria were a gestational age of >20 weeks, an available baseline serum creatinine concentration, and complete clinical data. The exclusion criteria were a gestational age of <20 weeks, a history of known hematologic disease affecting coagulation, a history of renal replacement therapy and nephritis, a history of elevated creatinine, hospitalization in the obstetrics department for <24 hours, and missing clinical data.
Significant hemodynamic shifts occur during pregnancy, including an increased blood volume. 15 This means that the creatinine concentration during pregnancy is lower than that during non-pregnancy, and the diagnostic criteria applicable to non-pregnancy do not necessarily apply during pregnancy. In the present study, we did not use the usual diagnostic criteria for AKI, such as the KDIGO criteria. 16 PR-AKI was defined as a 50% increase in the serum creatinine concentration versus baseline and a concentration of >70.72 µmol/L.2,7,15,17 According to this definition, we included 625 pregnant women who developed AKI during hospitalization. In addition, women without AKI were selected as controls by matching the gestational age. Overall, 625 patients with PR-AKI and 628 normal pregnant women were available for the final analysis. The inclusion process of these 625 patients with PR-AKI is shown as Figure 1.
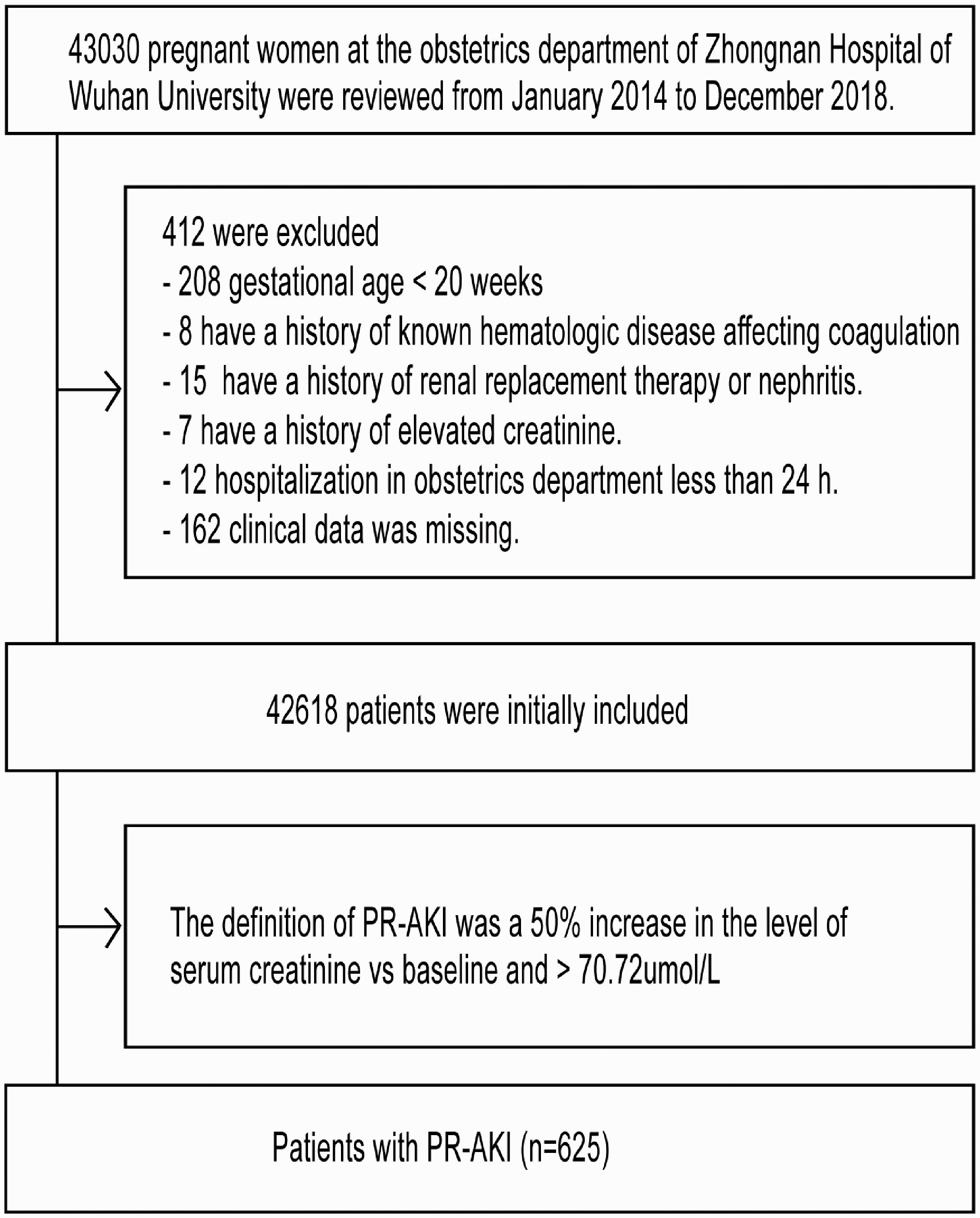
Study enrollment flow chart.
Moderate to severe PR-AKI was defined as a serum creatinine concentration of >124 µmol/L. 18 Renal recovery was defined as a decrease in the serum creatinine concentration to a normal level before discharge. Pregnancy-specific complications included preeclampsia, eclampsia, HELLP syndrome, thrombotic microangiopathy, and acute fatty liver of pregnancy. The diagnosis of these diseases was confirmed by consulting the International Classification of Diseases codes in the patients’ electronic medical records.
Data collection and statistical analysis
The patients’ D-dimer concentrations and demographic, clinical, and biochemical data were collected immediately after admission to the obstetrics department. We carefully screened the patients’ medical history to confirm the time and cause of AKI, clinical symptoms, intensive care unit hospitalization, dialysis, and death. The primary endpoint was the occurrence of PR-AKI, and the secondary endpoint was the development of dialysis and death in patients with PR-AKI.
Data were analyzed using SPSS version 22.0 software (IBM Corp., Armonk, NY, USA). The results were recorded as mean ± standard deviation or median (interquartile range) for quantitative variables. The two-sample t test or the Mann–Whitney U test was used for quantitative variables as appropriate. Categorical data are presented as proportions, and the chi-square test was used for qualitative variables. A P value of <0.05 was considered statistically significant. All variables with a P value of <0.05 in the univariate analysis were entered into the multivariate model. The prognostic value of the D-dimer concentration was evaluated using respective receiver operating characteristic (ROC) curves.
Results
Patient characteristics in the PR-AKI group and control group
The baseline characteristics of women with and without PR-AKI are shown in Table 1. The two groups had similar rates of preexisting diabetes and multipara. Women with PR-AKI were significantly more likely to be older (P = 0.007) and have preexisting hypertension (P < 0.001). In addition, women with PR-AKI had a higher systolic blood pressure, diastolic blood pressure, leukocyte count, alanine aminotransferase concentration, aspartate aminotransferase concentration, and total bilirubin concentration upon admission (P < 0.05). Moreover, patients with PR-AKI had a higher prothrombin time, activated partial thromboplastin time, and D-dimer concentration (P < 0.05). The platelet count, fibrinogen concentration, and serum albumin concentration were lower in patients with than without PR-AKI. There were no significant differences in hemoglobin between the groups.
Baseline characteristics of patients with PR-AKI and without PR-AKI.

Data are presented as mean ± standard deviation, median (range), or n (%).
aP values evaluated by two-sample t tests.
bP values evaluated by chi-square test.
cP values evaluated by Mann–Whitney U test.
PR-AKI, pregnancy-related acute kidney injury; SBP, systolic blood pressure; DBP, diastolic blood pressure; ALT, alanine aminotransferase; AST, aspartate aminotransferase; TBIL, total bilirubin; PT, prothrombin time; APTT, activated partial thromboplastin time; FIB, fibrinogen; PLT, platelets.
In the PR-AKI group, 22 patients (3.52%) received renal replacement therapy and 6 deaths (0.96%) were reported. The leading cause of death was amniotic fluid embolism, followed by acute fatty liver and postpartum hemorrhage. No deaths occurred in the group without PR-AKI, and none of the patients in this group received renal replacement therapy.
Comparison of clinical variables between patients with high and low D-dimer concentrations
The patients with PR-AKI were divided into two groups according to their D-dimer concentrations: Group A (D-dimer concentration of <1108 ng/mL) and Group B (D-dimer concentration of >1108 ng/mL). We selected the cut-off by ROC curves. The baseline characteristics of each group are shown in Table 2.
Comparison of clinical variables between patients with high and low D-dimer concentrations.

Data are presented as mean ± standard deviation, median (range), or n (%).
aP values evaluated by two-sample t tests.
bP values evaluated by chi-square test.
cP values evaluated by Mann–Whitney U test.
SBP, systolic blood pressure; DBP, diastolic blood pressure; PLT, platelets; PT, prothrombin time; APTT, activated partial thromboplastin time; FIB, fibrinogen; ALT, alanine aminotransferase; AST, aspartate aminotransferase; TBIL, total bilirubin.
Group B had significantly higher values than Group A in terms of multiple pregnancy (P < 0.001), the leukocyte count (P < 0.001), prothrombin time (P < 0.001), activated partial thromboplastin time (P < 0.001), aspartate aminotransferase concentration (P < 0.001), alanine aminotransferase concentration (P < 0.001), total bilirubin concentration (P < 0.001), and serum creatinine concentration (P < 0.001). However, the hemoglobin concentration (P < 0.001), platelet count (P < 0.001), fibrinogen concentration (P < 0.001), and serum albumin concentration (P < 0.001) were significantly lower in Group B. There were no significant differences between the groups in age, gestational age, preexisting diabetes, in vitro fertilization, multipara status, preexisting hypertension, admission systolic blood pressure, admission diastolic blood pressure, or positive urine protein.
D-dimer concentration as a predictor of primary outcome
A multivariate logistic regression analysis was performed on the indicators listed in Table 1. All indicators with a P value of <0.05 were included. The results showed that a D-dimer concentration of >1108 ng/mL was associated with the development of PR-AKI in the univariate analysis (odds ratio, 4.805; 95% confidence interval [CI]. 3.544–6.515; P < 0.001). It was further proven to be an independent predictor of PR-AKI (odds ratio, 2.138; 95% CI, 1.448–3.157; P < 0.001) in the multivariate analysis after adjustment for age, comorbidities, leukocyte count, transaminase concentrations, total bilirubin concentration, coagulation parameters, and serum albumin concentration. The results are shown in Table 3. We can conclude that the D-dimer concentration is significantly associated with the development of AKI in pregnant patients.
Univariate and multivariate regression analysis for pregnancy-related acute kidney injury.

OR, odds ratio; CI, confidence interval; SBP, systolic blood pressure; DBP, diastolic blood pressure; ALT, alanine aminotransferase; AST, aspartate aminotransferase; TBIL, total bilirubin; PT, prothrombin time; APTT, activated partial thromboplastin time; FIB, fibrinogen; PLT, platelets.
Comparison of clinical characteristics between patients with high and low D-dimer concentrations
Table 4 shows the clinical characteristics of Groups A and B. Four patients (1.0%) in Group A and 18 patients (7.9%) in Group B received renal replacement therapy (P < 0.001). A significantly higher percentage of patients in Group B than in Group A had edema symptoms (P = 0.043), mechanical ventilation therapy (P < 0.001), and the possibility of staying in the intensive care unit (P < 0.001). Moreover, renal nonrecovery (P < 0.001) and death (P = 0.025) were significantly more common in Group B than in Group A.
Clinical characteristics of patients with PR-AKI.

Data are presented as mean ± standard deviation, median (range), or n (%).
aP values evaluated by two-sample t tests.
bP values evaluated by chi-square test.
cP values evaluated by Mann–Whitney U test.
PR-AKI, pregnancy-related acute kidney injury; HELLP, hemolysis, elevated liver enzymes, low platelet count; ICU, intensive care unit.
Prognostic value of D-dimer concentration for secondary outcome
The prognostic value of the D-dimer concentration was evaluated using ROC analysis. Figure 2 shows the ROC curves plotted using independent predictors of PR-AKI. The area under the curve (AUC) of the D-dimer concentration was 0.652 (95% CI, 0.622–0.683; P < 0.001), showing a moderate predictive value.

ROC curves of D-dimers, AST, admission SBP, admission DBP, and leukocytes as predictors of PR-AKI.
Figure 3 shows the prognostic value of the D-dimer concentration in patients with PR-AKI. The AUC of the D-dimer concentration as a prognostic indicator for dialysis was 0.819 (95% CI, 0.709–0.928; P < 0.001). The cutoff of the D-dimer concentration that maximized the sensitivity and specificity for predicting dialysis was 2389 ng/mL. The sensitivity was 77.3% and the specificity was 84.4% when we used a D-dimer concentration of 2389 ng/mL as a cutoff, and there was a significant difference between the two groups (P < 0.05) (Figure 4).

Prognostic value of D-dimer concentration in patients with pregnancy-related acute kidney injury. (a) D-dimer concentration as a prognostic indicator for dialysis (AUC, 0.819). (b) D-dimer concentration as a prognostic indicator for death (AUC, 0.828). (c) D-dimer concentration as a prognostic indicator for renal non-recovery (AUC, 0.631). (d) D-dimer concentration as a prognostic indicator for adverse outcomes (AUC, 0.657).

Among patients with pregnancy-related acute kidney injury, a significant difference was found in the number of patients undergoing dialysis between those with a D-dimer concentration of >2389 and <2389 ng/mL.
The D-dimer concentration as a prognostic indicator for other outcomes is shown in Figure 3. The AUC values of the D-dimer concentration for predicting death, renal failure, and adverse outcomes in patients with PR-AKI were as follows: death (AUC, 0.828; 95% CI, 0.670–0.986; P = 0.006), renal failure (AUC, 0.631), and adverse outcomes (AUC, 0.657) (adverse outcomes = intensive care unit hospitalization + dialysis + death + renal failure). In conclusion, the D-dimer concentration may increase the risk of dialysis and death in women with AKI.
Discussion
In this case-control study, we found that the D-dimer concentration was associated with the development of PR-AKI. A D-dimer concentration of >1108 ng/mL was an independent predictor of PR-AKI, and the prognostic value of the D-dimer concentration for PR-AKI was moderate. When patients with PR-AKI were divided into two groups based on their D-dimer concentrations, the serum creatinine concentration and percentage of moderate to severe PR-AKI were significantly higher in Group B (D-dimer concentration of >1108 ng/mL) than in Group A (D-dimer concentration of <1108 ng/mL). In addition, in patients with PR-AKI, the D-dimer concentration was significantly associated with renal replacement therapy and in-hospital mortality. The AUC of the D-dimer concentration for dialysis and death was 0.819 and 0.828, respectively.
Physiological hypercoagulability is usually present in a normal pregnancy and is indispensable for reduction of postpartum hemorrhage. However, our study showed that women with PR-AKI exhibited higher D-dimer concentrations than women with normal pregnancy. To our knowledge, few studies have focused on the relationship between the D-dimer concentration and PR-AKI. Godara et al. 19 enrolled 57 patients with PR-AKI and observed that higher D-dimer concentrations were more common in patients with renal non-recovery than in those with renal recovery.
Although the mechanisms linking the D-dimer concentration to PR-AKI are unclear, previous studies have revealed some clues. The D-dimer concentration is a useful biomarker of hemostasis and fibrinolysis. In recent years, however, evidence has emerged to suggest that the D-dimer concentration is likely to rise in the setting of systemic inflammation and infection. The predictive value of the D-dimer concentration in critically ill patients has been confirmed. In 2002, Shorr et al. 20 found that the presence of D-dimers may reflect an imbalance between proinflammatory and anti-inflammatory cytokines. With an increase in D-dimers, the tumor necrosis factor-alpha, interleukin-6, and interleukin-8 levels increase and the incidence of multisystem organ failure and death also increase in critically ill patients. Similarly, Shitrit et al. 21 noted that the D-dimer concentration was correlated with the organ system failure index. To exclude the interference of complications, we adopted a multivariate regression analysis to adjust for possible confounding factors, and the results showed that a rise in the D-dimer concentration can be used as an independent predictor of PR-AKI (P < 0.001) (Table 3).
In the field of pregnancy, the D-dimer concentration has been studied in patients with gestational hypertensive disorders (GHDs). Baboolall et al. 22 performed a retrospective observational cohort study of 443 women and concluded that the D-dimer concentration might predict severe preeclampsia (AUC, 0.828). Similarly, Kim et al. 23 performed a retrospective cohort study of pregnant women with GHD and noted that patients with severe GHD had significantly higher D-dimer concentrations than those with non-severe GHD. The authors attributed these results to formation of multiple microthrombi in the placenta, resulting in the release of circulating factors into the maternal circulation and consequent endothelial dysfunction and inflammatory response. Therefore, activation of inflammatory cytokines and coagulation pathways may play an important role between the D-dimer concentration and PR-AKI.
The causes of PR-AKI are diverse and include septic abortions, severe hemorrhage, sepsis, and pregnancy-specific complications, all of which may affect the inflammatory and coagulation systems to varying degrees.4,10,17 Preeclampsia has been associated with a hypercoagulable state. 24 Thrombotic microangiopathy comprises thrombotic thrombocytopenic purpura and atypical hemolytic uremic syndrome. Their common characteristics are occlusion of small arteries and capillaries and platelet aggregation. Activation of coagulation pathways may influence inflammation by producing inflammatory factors. 25 In contrast, a persistent inflammatory response can lead to a hypercoagulable state.
In routine prenatal examinations and care, we can screen out most patients with high-risk pregnancies who are usually prone to AKI, such as patients undergoing dialysis, patients with nephritis or abnormal renal function, and patients with autoimmune diseases such as systemic lupus erythematosus. For women without the above-mentioned high-risk factors, however, the possibility of developing AKI during pregnancy cannot be ruled out. Based on the findings of the present study, we conclude that an increased D-dimer concentration is an independent risk factor for AKI in pregnant patients and can increase the risk of dialysis and death. Therefore, evaluation of the D-dimer concentration in pregnant women can help to identify higher-risk groups, and close monitoring of their renal function and urine output can help clinicians to take appropriate intervention measures.
This study has two main strengths. First, to the best of our knowledge, this is the first study to report the relationship between the D-dimer concentration and PR-AKI. Second, we assessed the usefulness of the D-dimer concentration as a predictor of dialysis and in-hospital mortality.
Our study also has several limitations. First, we did not serially evaluate the D-dimer concentration during pregnancy, although the D-dimer concentration gradually increases during pregnancy. However, we reduce this error by matching the gestational age. Second, we failed to compare the D-dimer concentration with other renal injury markers. This is mainly because this was a retrospective study and some data were missing. Finally, this was a single center study, and the results do not necessarily apply to other centers. Prospective, large-sample clinical studies are required.
Conclusions
Our research suggests that a D-dimer concentration of >1108 ng/mL is an independent predictor of AKI in pregnant women and that an elevated D-dimer concentration increases the risk of dialysis and death in women with AKI. Thus, we should closely monitor the renal function when the D-dimer concentration is high and ensure timely intervention.