
Abstract
Background
Critical care survivors face physical, psychological and socio-economic burdens. Peer support is acknowledged as a way individuals can face, accept and overcome the challenges arising from a stressful event. We sought to examine the provision and benefits of peer support to critical care survivors in the UK.
Method
We distributed a survey, devised by the patients and relatives committee of the Intensive Care Society and ICUsteps, to contacts in 163 UK Trusts/hospitals with critical care departments. The benefit to individuals was assessed by seeking the views of attendees of two support groups.
Results
A response was received from 91 (56%) of the critical care departments. Of these, 46 (48% of respondents) have patient support groups. Our analysis of comments from 30 people is that support groups greatly benefit service users and staff.
Conclusions
Attendees of patient support groups gave highly positive comments about the service yet provision of patient support groups in the UK is not universal.
Recommendations
We make a series of recommendations for consideration by UK health care providers.
Introduction
It is known that survival after critical care poses significant physical, psychological, economic and social burdens on patients and their families. 1 Many have continuing problems with pulmonary, neuromuscular and physical function and suffer from anxiety, depression and post-traumatic stress symptoms for months or years after critical care admission.2–5 Patients may be unable to return to work, find it difficult to communicate with their families and feel socially isolated.
Peer support groups allow people with shared experiences to give and receive support to each other. Peers help each other learn about how best to manage feelings and experiences that are difficult. 6 The first critical care peer support groups in the UK were set up by the patient charity ICUsteps, who continue to run a number of groups around the country. 7 Other units have set up peer support groups independently of this network. Some UK critical care support groups were funded by the Thrive international collaborative under the umbrella of the US Society of Critical Care Medicine (SCCM). Peer support groups may be led by patients or facilitated by clinicians such as nurses, doctors or psychologists. They may have a mental health, educational, practical or social focus, and be held in hospitals or in the community. 8
Guidelines from the Intensive Care Society (ICS)9 and Faculty of Intensive Care Medicine (FICM) (2019) and the National Institute for Health and Care Excellence (NICE, 2009)10 both highlight the need for providers to deliver both patient support groups and critical care follow-up clinics. There is no current data on the availability or nature of critical care peer support groups in the UK. In view of this, the Patients and Relatives Committee of the Intensive Care Society (ICS), in conjunction with ICUstep, decided to survey NHS providers to assess current provision.
Methods
The Patients and Relatives Committee, with input from ICUsteps and help from the Scottish Intensive Care Society (SICS), devised and distributed a survey via Survey Monkey to nursing and allied health professional (AHP) members of the ICS. After the initial mailing we enlisted the help of ICNARC (Intensive care national audit and research centre) who distributed the link to the questionnaire to the lead nurse in each of the units in their audit program. Where replies were received from more than one individual in an organisation, only the first response was analysed.
Critical care survivors attending ICUsteps peer support groups were asked to give written feedback on the benefits or otherwise of attending the groups. Their comments have been collated by theme.
Prior to circulation, this survey was considered by both the Council of the ICS and the Board of ICUsteps.
Results
Questionnaire survey
Questions and responses to the UK critical care peer support survey.
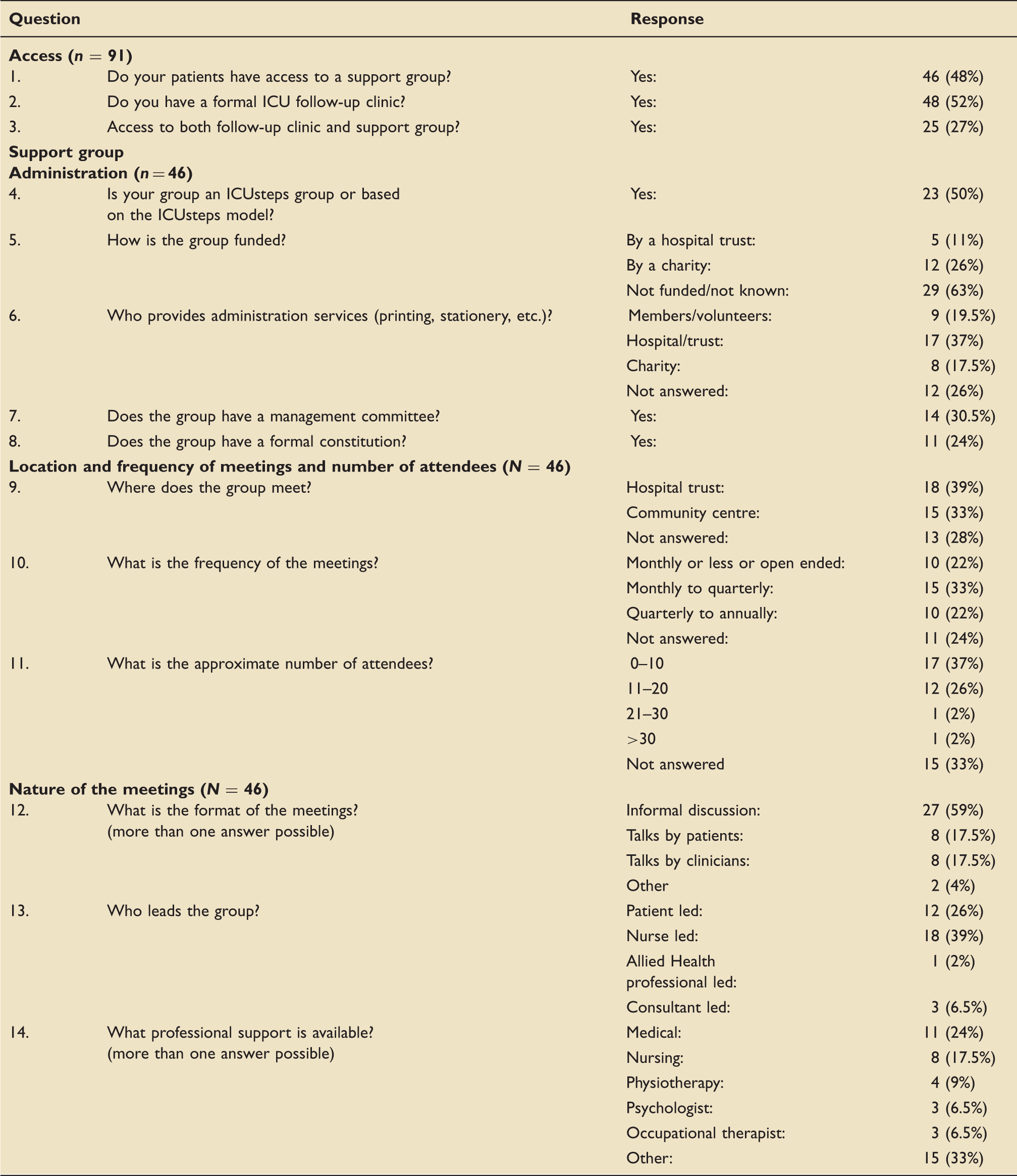
Only a minority of groups – 17 (37%) receive funding, the majority from charitable sources. Administrative services are provided mostly by the hospital, but sometimes by members or charitable sources. Just under a third of groups have management committees including ex-patients and/or carers. About half have a formal constitution.
There is a wide range in the frequency of meetings, with the most common frequency being between 3-and 6-monthly. Groups mostly meet in hospitals or community centres. There is also a wide range of group attendance with several groups reporting less than five attendees per meeting, and one group reporting over 30.
Groups are mostly led by nurses, although eight are patient-led. The majority of the groups (27) have an informal discussion format. Eight organise talks by medical staff and eight have patients talking at their meetings. There was professional support available at most of the groups.
Patient feedback
Service user and staff comments about patient support groups.
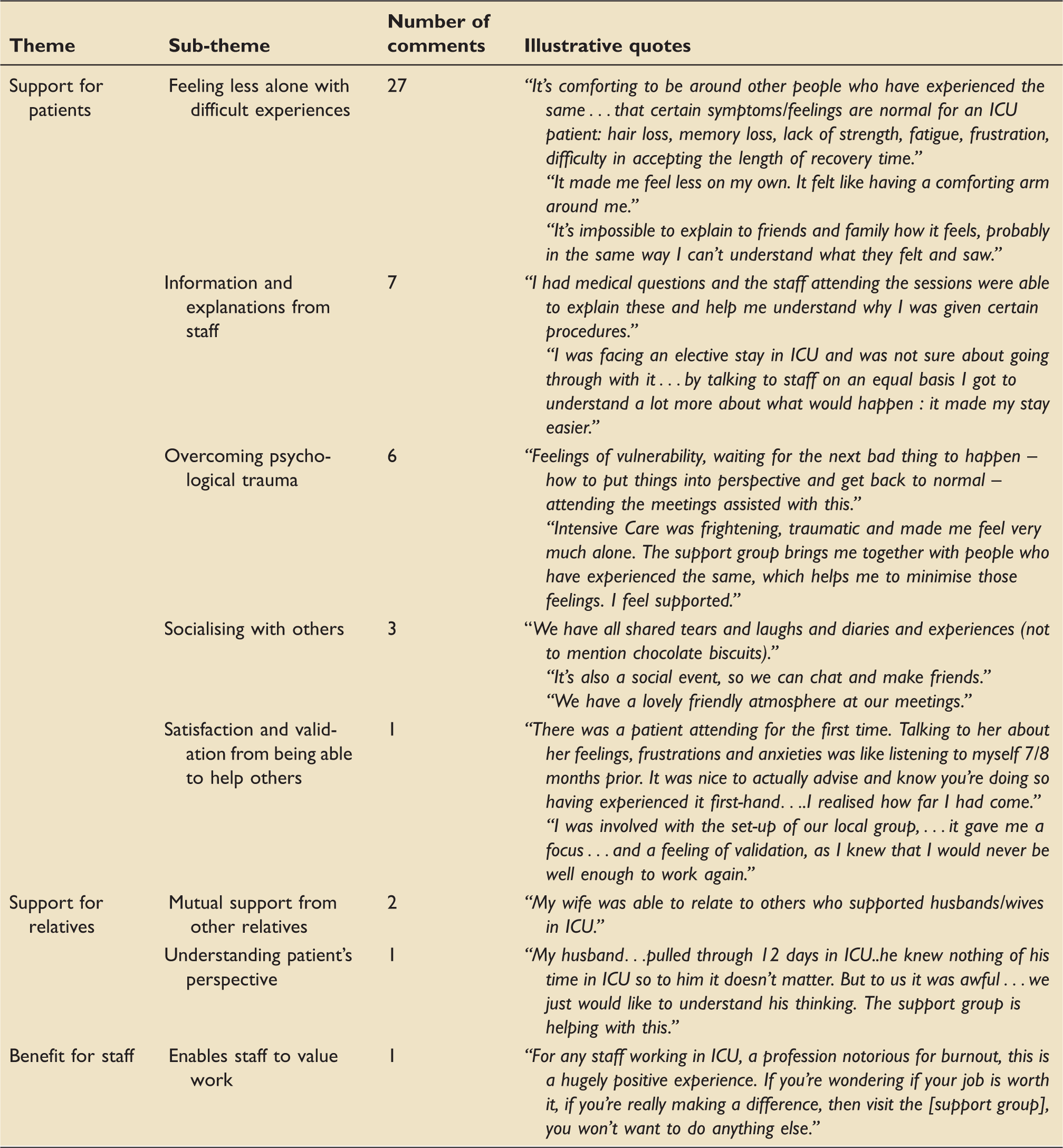
The overriding views of those commenting were positive.
Discussion
Many, if not all organisations, provide informal support to critical care survivors, with post unit visits by outreach teams and an ‘open door’ after discharge. However rehabilitation programmes form an important part of the management of both the physical and psychological aftermath of critical illness, and peer support groups can be a helpful part of these programmes. Encouragingly, patients and families from 46 organisations (48% of respondents) had access to a critical care support group. Increased recognition of the psychological impact of critical care during the COVID-19 pandemic may lead to more groups being set up.
Existing groups appear to be run with minimal formal funding, though most (85%) have support from, or are led by, hospital staff, and many have use of hospital facilities and some administrative services. There was a striking heterogeneity in both the number of attendees, from less than 5 to more than 30, and also in the frequency of meetings, from monthly to annually.
Our analysis suggests that critical care support groups are valued by service users. The overwhelming benefit for patients was receiving empathy, understanding and support from others who had been through the same experience. Knowing that they were not alone helped them to come to terms with their critical care stay. Meeting staff who could answer questions demystified the critical care episode, and in some cases helped patients overcome psychological trauma. Patients also felt validated by supporting other patients and helping to run groups.
For relatives, the support group offered the chance to meet other relatives with similar traumatic experiences, as well as helping them understand what patients had been through (both patients and relatives mentioned that families and friends found it hard to understand patients’ experience of critical care). The meetings also proved positive for attending healthcare staff, giving them a rare chance to meet recovering patients.
Despite the recommendations from both NICE (2009)10 and the ICS/FICM (2019), 9 the provision of follow-up clinics remains low, with only half of the responders stating there was provision for their patients.
Strengths
The survey was sent out to all adult UK ICUs using the networks of three national organisations; the ICS, Scottish ICS and ICNARC. As well as quantitative data regarding provision of peer support groups, qualitative data, to describe the benefits of support groups to patients, relatives and staff, were collected in the form of comments from support group users.
Limitations
While the response rate of 56% is well above average (33%), a higher rate would be optimal. We also received multiple responses from 16 organisations that were not always internally consistent. Our decision only to use the first response may have led to errors, as may have self-reporting. In view of this, and because of the high proportion of unanswered questions, reported results, such as the frequency of meetings and number of attendees, without access to formal registers, were at best a good estimate.
Conclusions
From the data we have collected we conclude that the provision of patient support groups and critical care follow up clinics are available to around half of patients discharged from critical care units in the United Kingdom. The patients and relatives committee of the ICS and ICUsteps endorse the following standards and make the following recommendations.
Standards
All patients with identified rehabilitation needs who are discharged from critical care should have access to a rehabilitation programme which includes follow up within three months of discharge (NICE, 2009).
10
To help deal with the psychological consequences of a critical care stay patients and family members of ICU survivors should be offered the opportunity to access information in written format and peer support, as outlined in GPICS (2019) and the NICE post-traumatic stress disorder guideline (2018, section 1.4).9,11
Recommendations
Peer support groups should be based on a sustainable model. Health care providers should either offer facilities, staff and administrative support to peer support groups or strongly support third-sector provision. Health care providers should consider allocating nursing, medical and AHP staff (including psychologists) to peer support groups. Patients should be able to decide when to access peer support. Those with significant physical or psychological problems may prefer individualised care (e.g. cognitive behavioral therapy for PTSD) before they are ready to benefit from peer support groups.
Footnotes
Acknowledgements
The authors acknowledge Intensive Care National Audit and Research Centre, ICUsteps, Scottish ICS, Royal Berkshire Hospital patient support group.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Jeremy Groves https://orcid.org/0000-0002-8413-8837 Dorothy Wade ![]()