
Abstract
Background
The optimal airway management strategy for in-hospital cardiac arrest is unknown.
Methods
An online survey and telephone interviews with anaesthetic and intensive care trainee doctors identified by the United Kingdom Research and Audit Federation of Trainees. Questions explored in-hospital cardiac arrest frequency, grade and specialty of those attending, proportion of patients receiving advanced airway management, airway strategies immediately available, and views on a randomised trial of airway management strategies during in-hospital cardiac arrest.
Results
Completed surveys were received from 128 hospital sites (76% response rate). Adult in-hospital cardiac arrests were attended by anaesthesia staff at 40 sites (31%), intensive care staff at 37 sites (29%) and a combination of specialties at 51 sites (40%). The majority (123/128, 96%) of respondents reported immediate access to both tracheal intubation and supraglottic airways. A bag-mask technique was used ‘very frequently’ or ‘frequently’ during in-hospital cardiac arrest by 111/128 (87%) of respondents, followed by supraglottic airways (101/128, 79%) and tracheal intubation (69/128, 54%). The majority (60/100, 60%) of respondents estimated that ≤30% of in-hospital cardiac arrest patients undergo tracheal intubation, while 34 (34%) estimated this to be between 31% and 70%. Most respondents (102/128, 80%) would be ‘likely’ or ‘very likely’ to recruit future patients to a trial of alternative airway management strategies during in-hospital cardiac arrest. Interview data identified several barriers and facilitators to conducting research on airway management in in-hospital cardiac arrest.
Conclusions
There is variation in airway management strategies for adult in-hospital cardiac arrest across the UK. Most respondents would be willing to take part in a randomised trial of airway management during in-hospital cardiac arrest.
Keywords
Introduction
In-hospital cardiac arrest (IHCA) is an important health problem; current survival to hospital discharge is approximately 24% for all IHCA patients, 1 but may be closer to 10% for those requiring advanced airway management in the UK population (Couper K, personal communication, 2020). Airway management is an integral part of cardiac arrest management, and may affect patient outcome. 2 There is limited evidence on the optimal approach to airway management during adult IHCA; 2 however, an observational study from the United States documented an association between the use of tracheal intubation (TI) during IHCA and decreased survival to hospital discharge. 3
While TI has been considered the definitive technique for advanced airway management, 4 recent randomised controlled trials (RCTs) in out-of-hospital cardiac arrest (OHCA) suggest there may be advantages to using supraglottic airway (SGA) devices instead of TI.5,6
Differences in the skills and experience of the healthcare professionals responsible for airway management 7 and clinical differences between IHCA and OHCA patients make it unclear whether these advantages are transferable to the in-hospital setting.4,8–11 However, there are theoretical advantages to using a SGA over TI during IHCA: SGAs are generally quicker and easier to insert, 12 may reduce the frequency and duration of pauses in chest compression, 13 and can be inserted safely by a wider range of hospital staff. 12
The International Liaison Committee on Resuscitation (ILCOR) has called for high-quality research to determine the best approach to airway management during IHCA. 14 However, questions remain about the feasibility of conducting a trial in this area because it is unclear what proportion of IHCA calls require advanced airway management, whether there is equipoise regarding airway management strategies, and whether a trial of advanced airway management strategies during IHCA would be feasible and acceptable to practitioners.
We conducted a national survey of UK NHS staff responsible for airway management during IHCA, and follow-up telephone interviews with a selection of participants.
The aims of this project were:
To examine current airway management practice during adult IHCA To explore participants' attitudes to potential participation in a randomised trial of airway management during IHCA; To explore the feasibility of proposed aspects of trial design, and identify potential barriers and facilitators.
Methods
Approval for data collection from all hospitals was obtained from the University of the West of England, Bristol Faculty of Health and Applied Sciences Research Ethics Committee (HAS.19.10.055, 15.11.2019). Information about the study was provided to all participants before informed consent was obtained. This included a description of the purpose of the study, what would be involved in participation, details of data confidentiality and storage, a privacy notice and contact information for the study team. Written and verbal consent was obtained for all participants taking part in the interviews. Participants were required to confirm consent electronically before the first survey question was presented.
Eligible participants were anaesthetic and intensive care trainees with responsibility for adult IHCA airway management at their UK hospital site. Potential participants were identified through the Research and Audit Federation of Trainees (RAFT) – a collaborative UK-wide trainee-led research group comprising multiple regional trainee research networks.
An online survey (Supplemental Appendix 1) was designed and piloted by the study team and prepared in Qualtrics (Provo, Utah). It was then piloted again for usability and technical functionality. One response was sought per hospital site; RAFT distributed the survey link via email to one eligible trainee at each hospital site covered by the RAFT UK network (n = 168). Trainees completed the survey between December 2019 and January 2020. The survey comprised 12 questions with a mixture of multiple-choice answers and free text responses. A maximum of four items were displayed on any one survey page, and the full survey was distributed over approximately seven pages. A progress bar was shown at the top of the page as the respondent was completing the survey. Questions explored: responsibility for airway management during IHCA (specialty, grade); the availability and use of different airway management techniques; estimated incidence of IHCA; the proportion of IHCA patients who receive advanced airway management; whether there was equipoise for the research question; willingness to participate in research comparing different methods of airway management during IHCA.
Between January and February 2020, a sub-set of trainees (n = 17) were selected using a representative sampling approach (one participant per geographical trainee regional network), and invited to take part in a semi-structured telephone interview at a time convenient to them. An interview topic guide (Supplemental Appendix 2) was designed to explore barriers and facilitators to the design and conduct of a randomised trial of airway management during IHCA. Interviews lasted approximately 10 min and were conducted by authors LG, BS and SV and recorded using Skype for Business.
Data were analysed using a modified ‘following a thread’ 15 approach, beginning with an initial analysis of each dataset to identify key concepts requiring further exploration.
Quantitative survey data were collated using Qualtrics and exported to Microsoft Excel, where duplicate and incomplete responses were removed. Data were then analysed and presented using simple descriptive statistics. Free-text responses to the online survey were exported to Microsoft Excel and coded into categories for analysis.
Two researchers independently listened to the audio recordings from the telephone interviews, made notes on emerging concepts, and recorded verbatim quotes in a Microsoft Word document. Concepts and quotes were shared between the researchers, and reviewed collaboratively to discuss interpretation of the data.
Concepts from one dataset were then followed across to the other to create a thread of findings, which integrated the focus and specificity of the quantitative data with the richness of the qualitative data.
Results
A total of 140 responses to the survey were received, and after exclusion of partial (n = 1) and duplicate (n = 11) responses there were 128 completed surveys: a response rate of 76%. There was representation from all constituent countries of the UK, with a reasonable spread of responses geographically (Figure 1), apart from the East of England where RAFT is not represented. Survey data can be found in the supplementary materials. Seventeen trainees participated in individual semi-structured telephone interviews.
Map of hospital sites from which responses were received.*
Current airway management practice during IHCA
Grade of practitioner with responsibility for airway management during adult IHCA at all participating UK hospital sites.
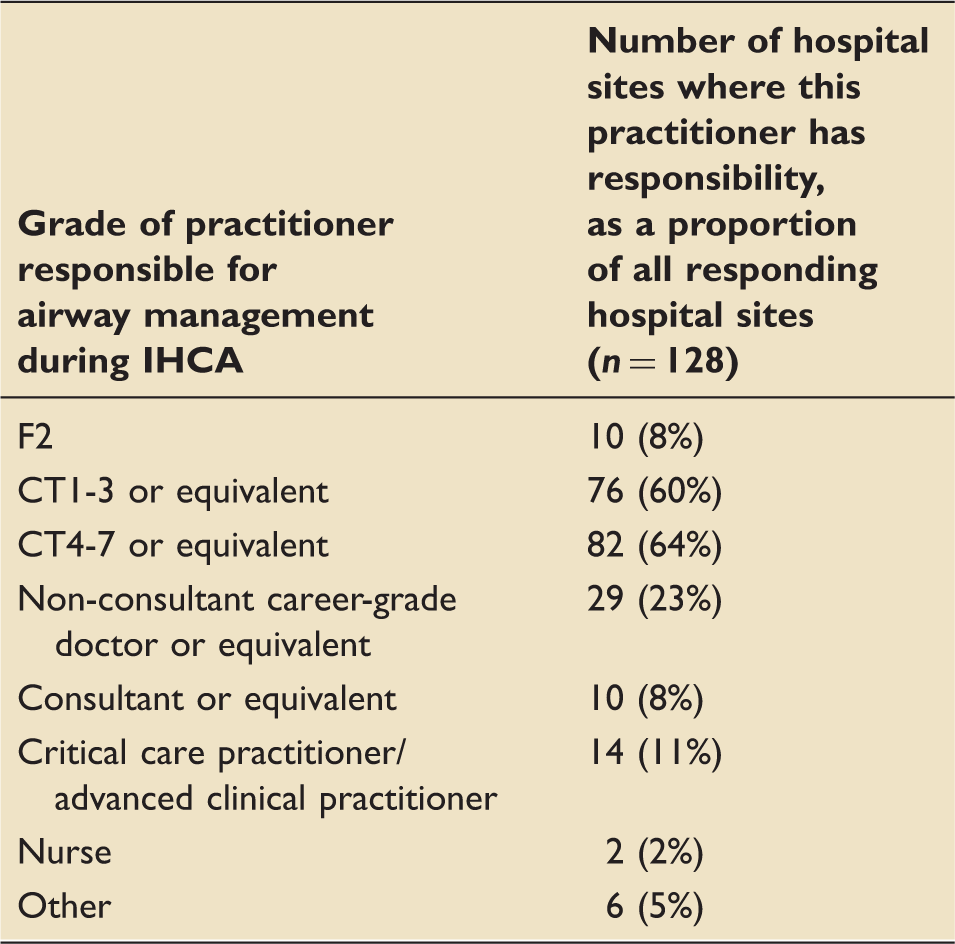
At many sites, more than one practitioner may have responsibility for airway management during adult IHCA.
The majority (123/128, 96%) of respondents reported the availability of both TI and SGAs for airway management during IHCA. Of the 126 sites with TI available during IHCA, 30 (24%) reported the availability of videolaryngoscopes. Of the 125 sites with SGA devices available during IHCA, 120 (96%) reported availability of the i-gel, 44 (35%) reported availability of the laryngeal mask airway (LMA), and 7 (6%) reported availability of the laryngeal tube. The majority (81/125, 65%) reported that only one type of SGA device was available during adult IHCA; for 77 (62%) respondents this was the i-gel and for 4 (3%) respondents this was the LMA.
When asked about additional aids during adult IHCA, a skilled assistant was immediately available to 61/128 (48%) respondents, 95 (74%) had an intubating bougie immediately available, colorimetric capnography was available to 38 (30%), and waveform capnography was available to 67 (52%). Fifteen of the 128 respondents (12%) reported that none of these aids were immediately available during adult IHCA, and free-text answers suggested a disparity of equipment availability between wards: ‘[only] some areas outside ICU do have waveform capnography and videolaryngoscopy. Sometimes I take the [videolaryngoscopy] from ICU to arrests with the transfer bag.’
Respondents also suggested that available equipment was not always suitable for the patients they were attending; one respondent commented ‘our Trust only provides size 4 i-gel on cardiac arrest trolleys.’ Others reported that the full range of airway management techniques, including fibreoptic scopes and front of neck access, were ‘available to anaesthesia, but are not available on the standard arrest trolley.’
The use of different airway management techniques was compared by the percentage of respondents using the technique either ‘very frequently’ or ‘frequently’; bag-mask was chosen ‘very frequently’ or ‘frequently’ by 111/128 (87%) of respondents, followed by SGAs (101/128, 79%) and then TI (69/128, 54%). Free-text responses emphasised the importance of patient history, underlying diagnosis and patient co-morbidity in decisions regarding which airway management technique should be used. The ‘perception of whether or not patients would be a candidate for ICU’ was also cited as influencing this decision, along with factors including airway soiling and adequacy of the SGA seal.
When asked to estimate the number of IHCA patients who currently undergo TI prior to achieving a return of spontaneous circulation, or the cessation of resuscitation attempts, the majority (60/100, 60%) estimated this to be 30% or fewer, while 34 (34%) estimated this proportion to be between 31% and 70%, and 6 (6%) estimated this at more than 70%.
Taking part in a trial of airway management during IHCA
Attitudes towards a randomised trial of airway management strategies during IHCA were largely positive; the majority (102/128, 80%) of survey respondents said they would be either ‘likely’ or ‘very likely’ to take part in this type of study. Respondents who said they were ‘unlikely’ (5/128, 4%) or ‘very unlikely’ (2/128, 2%) to take part indicated ethical concerns with randomising patients to one airway management technique or another. There were also concerns about the practicality of individual patient randomisation, availability of equipment and the need for a definitive airway in patients who would require ongoing care.
Interview data reflected survey results; 16 of the 17 interviewees reported that they would participate in a trial of airway management strategies and felt it was an important research question to address.
There's nothing great in the literature on whether or not one's better at securing the airway during a cardiac arrest than the other. There's different skill sets involved [in using each strategy]. So obviously if an SGA is deemed to be comparable to TI then that's probably for the better. Interview 3
Participants also confirmed that there is considerable variation in how airway management decisions are made, and that having a ‘best practice’ standard would aid this decision-making.
I think that to get a general answer [on which strategy to use] would certainly be useful. And I think probably a randomised controlled trial is the best way of doing that, and is going to give us the best answer. Interview 6
However, a minority of participants expressed concerns that a trial might constitute a change in practice at their hospital. One such concern was that randomisation could place increased burden on the intensive care unit (ICU), as ‘[the] tube commits people to ICU.’ Another participant stated that they would have to call a second person if they were going to insert a tracheal tube at an IHCA. These additional requirements led participants to suggest that there would need to be ‘buy-in’ from ICU and senior members of staff to facilitate a potential trial.
When reflecting on additional barriers and facilitators to the design of a potential trial, participants suggested that the ability to use clinical judgment where appropriate should be emphasised, in order to increase the acceptability of a randomised trial design.
The urgency with which resuscitation needs to commence was noted by participants as a potential barrier to randomisation of patients, as the method of randomisation would need to be straightforward and rapid.
Once you arrive you have got to get involved quite quickly, so it would have to be something you could do very quickly … because as soon as you arrive, someone expects for you to take over the airway. Interview 4
There was also discussion regarding the timing of randomisation; while some participants suggested that this should happen on the way to an arrest call, others felt it was appropriate to randomise a patient once an arrest had been confirmed.
Some participants proposed that another staff member, such as a resuscitation officer or research nurse, could support recruitment either by randomising patients themselves or by reminding the recruiting doctor to do so.
Discussion
We identified considerable diversity in airway management practice for IHCA across the UK; the grade and speciality of the individual responsible for airway management varied significantly across hospital sites. This has implications for airway management during IHCA because the choice of technique may depend on the skill of the provider, and the support available to them. 2 Tracheal intubation may therefore be used more frequently in hospitals where more experienced clinicians are responsible for airway management during IHCA.
Our findings indicate that both TI and SGAs are commonly available to those responsible for airway management during IHCA, and that airway management technique is dependent on operator choice and judgement. While SGAs were indicated as being used slightly more frequently than TI, it is unclear whether this is due to personal preference, related to practitioners' individual skill and experience, or whether practitioners insert an SGA before moving on to TI in a step-wise approach. A stepwise approach to airway management is recommended in current guidelines for both IHCA and OHCA. 16 However, during interviews with paramedics who took part in a trial of advanced airway management for OHCA, some indicated that they would always use this stepwise approach, while others described using their professional judgement and clinical skills to decide which technique to use depending on the clinical situation.17,18
Both survey and interview participants suggested it would be feasible and acceptable to conduct a randomised trial of airway management during IHCA, and a number of suggestions were made about the design of a potential trial. As TI and SGA devices are both readily available and used with similar frequency, participants felt there was equipoise in relation to this research question. Randomisation would not cause substantial divergence from usual practice and would therefore not be ethically controversial. This is important, as previous literature suggests that for research to be successful the enrolment of patients into a research study must be simple and integrated into current practice as far as possible. 19
Respondents' willingness to take part in emergency care research is supported by findings from prehospital literature, where practitioners have expressed positive attitudes towards taking part in trials, both in general, 19 and specifically of airway management during cardiac arrest. 17 In a follow-up study of paramedics who took part in the AIRWAYS-2 trial, both survey respondents and interview participants were comfortable with enrolling critically unwell patients into a randomised controlled trial using either deferred or a waiver of consent. 17
There are some limitations to our study. Only one response was sought per hospital site and these responses were based on participants' reports and not externally validated. As such, there is the possibility of recall bias. However, all responses were from anaesthetic and intensive care trainees with responsibility for airway management during IHCA, who would therefore be best placed to provide accurate information on this topic. The participants of this study were identified by members of RAFT, which is a research organisation. It is therefore possible that this sample of trainees would be more willing to take part in an RCT than those who are not research active.
To the best of our knowledge, this is the first survey of current airway management strategy for adult IHCA in the UK, with a high response rate and excellent representation of UK geographical training regions. As such, we suggest that the survey findings are a reliable description of current practice in the UK.
In conclusion, our study demonstrates considerable variation in current airway management during IHCA in the UK. The majority of respondents felt that a randomised trial of airway management for IHCA was important and would be willing to take part in such a study.
Research data
sj-xlsx-1-inc-10.1177_1751143720949458 - Supplemental material for Airway management during in-hospital cardiac arrest in adults: UK national survey and interview study with anaesthetic and intensive care trainees
Supplemental material, sj-xlsx-1-inc-10.1177_1751143720949458 for Airway management during in-hospital cardiac arrest in adults: UK national survey and interview study with anaesthetic and intensive care trainees by Laura Goodwin, Katie Samuel, Behnaz Schofield, Sarah Voss, Stephen J Brett, Keith Couper, Doug Gould, David Harrison, Ranjit Lall, Jerry P Nolan, Gavin D Perkins, Jasmeet Soar, Matthew Thomas, Jonathan Benger and in collaboration with the Research and Audit Federation of Trainees (RAFT) network: on behalf of the UCC-SMART Study Group in Journal of the Intensive Care Society
Supplemental Material
sj-pdf-2-inc-10.1177_1751143720949458 - Supplemental material for Airway management during in-hospital cardiac arrest in adults: UK national survey and interview study with anaesthetic and intensive care trainees
Supplemental material, sj-pdf-2-inc-10.1177_1751143720949458 for Airway management during in-hospital cardiac arrest in adults: UK national survey and interview study with anaesthetic and intensive care trainees by Laura Goodwin, Katie Samuel, Behnaz Schofield, Sarah Voss, Stephen J Brett, Keith Couper, Doug Gould, David Harrison, Ranjit Lall, Jerry P Nolan, Gavin D Perkins, Jasmeet Soar, Matthew Thomas, Jonathan Benger and in collaboration with the Research and Audit Federation of Trainees (RAFT) network: on behalf of the UCC-SMART Study Group in Journal of the Intensive Care Society
Supplemental Material
sj-pdf-3-inc-10.1177_1751143720949458 - Supplemental material for Airway management during in-hospital cardiac arrest in adults: UK national survey and interview study with anaesthetic and intensive care trainees
Supplemental material, sj-pdf-3-inc-10.1177_1751143720949458 for Airway management during in-hospital cardiac arrest in adults: UK national survey and interview study with anaesthetic and intensive care trainees by Laura Goodwin, Katie Samuel, Behnaz Schofield, Sarah Voss, Stephen J Brett, Keith Couper, Doug Gould, David Harrison, Ranjit Lall, Jerry P Nolan, Gavin D Perkins, Jasmeet Soar, Matthew Thomas, Jonathan Benger and in collaboration with the Research and Audit Federation of Trainees (RAFT) network: on behalf of the UCC-SMART Study Group in Journal of the Intensive Care Society
Supplemental Material
sj-pdf-4-inc-10.1177_1751143720949458 - Supplemental material for Airway management during in-hospital cardiac arrest in adults: UK national survey and interview study with anaesthetic and intensive care trainees
Supplemental material, sj-pdf-4-inc-10.1177_1751143720949458 for Airway management during in-hospital cardiac arrest in adults: UK national survey and interview study with anaesthetic and intensive care trainees by Laura Goodwin, Katie Samuel, Behnaz Schofield, Sarah Voss, Stephen J Brett, Keith Couper, Doug Gould, David Harrison, Ranjit Lall, Jerry P Nolan, Gavin D Perkins, Jasmeet Soar, Matthew Thomas, Jonathan Benger and in collaboration with the Research and Audit Federation of Trainees (RAFT) network: on behalf of the UCC-SMART Study Group in Journal of the Intensive Care Society
Supplemental Material
sj-pdf-5-inc-10.1177_1751143720949458 - Supplemental material for Airway management during in-hospital cardiac arrest in adults: UK national survey and interview study with anaesthetic and intensive care trainees
Supplemental material, sj-pdf-5-inc-10.1177_1751143720949458 for Airway management during in-hospital cardiac arrest in adults: UK national survey and interview study with anaesthetic and intensive care trainees by Laura Goodwin, Katie Samuel, Behnaz Schofield, Sarah Voss, Stephen J Brett, Keith Couper, Doug Gould, David Harrison, Ranjit Lall, Jerry P Nolan, Gavin D Perkins, Jasmeet Soar, Matthew Thomas, Jonathan Benger and in collaboration with the Research and Audit Federation of Trainees (RAFT) network: on behalf of the UCC-SMART Study Group in Journal of the Intensive Care Society
Footnotes
Acknowledgements
We are grateful to the Research and Audit Federation of Trainees (RAFT) network who assisted with identifying participants, and to the following individuals who assisted with data collection: I Abdelkhakek, M Alexander, T Alexander, D Barretto, B Baxter, R Berwick, AJ Boulton, K Bull, A Chamberlain, F Cook, J Cronin, C Couzens, J Eady, A Evans, J Fletcher, AJ Gardner, S Gilliland, M Gudipati, S Goodhand, WM Hare, A Hassan, R Hawes, R Ibrahim, M Ince, K James, M Jarvis, N Jones, P Keane, S Lee, A Lim, N Littley, S Marsden, J Mathiszig-Lee, C Maxwell, S May, V McAllister, J McCarter, T Moody, R Mudie, LR Nanda, S Natarajan, M Nordblad, AD Patil, D Perry, S Peacock, C Riley, K Roberson, N Roberts, J Sakathevan, A Sangam, S Scott, C Seeley, P Shekar, S Siew, M Sinnott, J Slattery, EJ Smith, M Smith, S Thoms, S Traynor, T Trouton, A Williams, C Wearmouth, C Yates.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by University Hospitals Bristol NHS Foundation Trust [RCF-SI-2019-01]. GDP is supported National Institute for Health Research (NIHR) Applied Research Collaboration (ARC) West Midlands and NIHR Senior Investigator. The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.