
Abstract
Objective
The ETView VivaSight single lumen airway tube (ETView) is a tracheal tube incorporating a video camera. We carried out a meta-analysis of previous simulation studies by inexperienced personnel to determine if the ETView could improve the success rate of first-attempt intubation.
Methods
We collected data from randomized controlled trials comparing the use of the ETView VivaSight single lumen versus a conventional endotracheal tube in a simulated manikin or cadaver study.
Results
Eleven studies (558 participants, 3,254 intubations, and 19 scenarios) were included. The ETView had a significantly higher success rate and shorter insertion time than conventional intubation in both normal airways (with or without chest compression) and in difficult airways. In addition, the ETView demonstrated better results in terms of a higher rate of Cormack−Lehane grade 1 and a lower incidence of dental trauma.
Conclusions
Inexperienced personnel can insert the ETView more rapidly and with a higher intubation success rate compared with a conventional tube.
Introduction
Endotracheal intubation is the gold standard technique for providing and maintaining a secure airway. Immediate airway interventions for oxygenation are necessary in emergency situations such as severe trauma, cardiac arrest, apnea, and coma because they can guarantee minimal pause in chest compressions. 1 However, endotracheal intubation requires considerable skill and experience and may be more difficult in certain situations, including in patients with an immobilized cervical spine as a result of severe trauma, or in chest compressions for cardiopulmonary resuscitation.2,3 Delayed or failed intubation has been identified as an important indicator of major airway complications, 4 and failure to perform successful endotracheal intubation may have devastating outcomes. In this regard, education and training for endotracheal intubation in a variety of situations can be helpful, and manikins have been widely used for simulations related to airway management.5,6
A new single-use, endotracheal tube (ETView VivaSight, ETView Ltd., Misgav, Israel) has recently become available. The device has an integrated, high-resolution camera with a display monitor and a light source embedded at the distal tip of the tracheal lumen, enabling continuous visualization of the camera view.7,8 The improved visualization features may facilitate effective airway management by inexperienced medical personnel in various situations. However, the ability of the ETView VivaSight single lumen (ETView) to improve intubation conditions overall, thereby increasing the first-attempt success rate and decreasing intubation time compared with conventional laryngoscopy, remains unclear.
We aimed to analyze pooled data from randomized controlled trials (RCTs) comparing the ETView, with conventional endotracheal tubes (cETTs) and a Macintosh laryngoscope in simulation studies by inexperienced personnel. The primary objective was to compare the success rates of first-attempt intubation using the ETView or cETTs in different simulation scenarios. We also assessed the intubation time, overall success rate, Cormack–Lehane grade, incidence of dental trauma, ease of use, and device preference.
Materials and methods
This systematic review and meta-analysis were performed according to the Cochrane Review Methods 9 and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) recommendations 10 (Supplemental material 1) and the study protocol was registered with PROSPERO (registration number: CRD42019132051). The study was designed to use existing literature and did not involve new human data, and was therefore exempt from institutional review board assessment.
Inclusion and exclusion criteria
We defined the inclusion and exclusion criteria a priori. The inclusion criteria (specified according to the PICO acronym) were as follows: Population: adult participants (aged >16 years) with no previous experience in clinical intubation with ETView in a simulated adult manikin or cadaver (aged ≥18 years), in studies including a crossover design; Intervention: intubation with video-mounted endotracheal tube (ETView); Comparator: intubation with a cETT with a Macintosh laryngoscope; Outcomes: first-attempt success rate, intubation time, tooth damage, Cormack–Lehane grade, overall success rate, ease of intubation score, and device preference. The exclusion criteria were participants aged ≤16 years, pediatric manikin or cadaver aged <18 years, and studies in a real clinical setting.
Database and literature sources
We searched MEDLINE (28 January 2020), Embase (28 January 2020), the Cochrane Controlled Trials Register and Cochrane Database on Systematic Reviews (28 January 2020), Web of Science (28 January 2020), Scopus (28 January 2020), and databases of RCTs that compared ETView VivaSight single lumen versus conventional intubation with a Macintosh laryngoscope in a simulated manikin or cadaver study including a crossover design. The following search terms were used: “intubation”, “ETView”, “VivaSight”, “manikin”, “manikins”, “mannequin”, “cadaver”, and “simulation”. There were no language restrictions imposed on the searches (Appendix 1).
After the initial electronic search, we evaluated the bibliographies of all the identified studies and performed a manual search using Google Scholar. We also searched the World Health Organization International Clinical Trials Registry Platform and the ClinicalTrials.gov database to identify unpublished or ongoing studies. The identified articles were individually assessed for inclusion in the analysis.
Data selection
Two independent investigators (SKO and YJW) performed the study selection by searching the titles and abstracts of the potentially eligible articles. Finally, the full text of the identified articles was retrieved and assessed for eligibility. Disagreements between the two investigators were resolved by discussion and consultation with a third author (BGL).
Data extraction
Among the searched trials, two authors (SKO and YJW) independently extracted the data for inclusion into a Microsoft Excel spreadsheet (Office 2016 professional edition, Microsoft Corp., Redmond, WA, USA). Any ongoing disagreement was reviewed and resolved by the third author (BGL). The following data were extracted: name of the first author, year of publication, journal name, study design, participant characteristics and number, presence of concurrent chest compression or difficult situations, and outcomes including time to intubation and insertion success rate.
The primary outcomes of this review were the first-attempt success rates in the ETView and cETT groups. Secondary outcomes were intubation time, tooth damage, Cormack–Lehane grade, overall success rate, ease of intubation score, and device preference. The success rate was determined according to the definitions of insertion failure (e.g., time limitation >60 s or incorrectly placed tube, such as esophageal intubation) described in each study. The overall success rate was defined as the final result after three attempts. The definition of intubation time (time to successful ventilation) varied among the studies: some studies used the initial grasp of the airway device (first contact) as the start point and first successful ventilation as the end point,11–13 while others used the insertion of the laryngoscope blade between the teeth as the start point,14,15 and others did not include any definition of the intubation time.
Crossover studies were treated as parallel studies, with each interventional phase treated as an independent arm of a parallel study. 16
Assessment of methodological quality
Two reviewers (SKO and YJW) independently assessed the risks of bias in the included articles according to the Cochrane Collaboration’s tool, consisting of selection, performance, detection, attrition, reporting, and other sources of bias. 17 Bias was graded as “low-risk,” “high-risk,” or “unclear.” Any ongoing disagreements between the two reviewers were resolved through discussion, or by review by the third author (BGL). Publication bias was assessed by funnel plot tests for asymmetry and Egger’s linear regression test.
Statistical analysis
This meta-analysis was carried out using RevMan version 5.3 software (The Cochrane Collaboration, Oxford, UK). Continuous variables, including intubation time, were analyzed using the inverse-variance method with the mean difference (MD) with 95% confidence intervals (CIs). An MD < 0 indicated that the intubation time was lower in the ETView group than in the cETT group. Dichotomous variables, including first-attempt success rate, overall insertion success rate, tooth damage, Cormack–Lehane grade, ease of intubation score, and device preference, were analyzed by pooled odds ratios (ORs), and 95% CI using the Mantel–Haenszel method. Random-effects models were conducted primarily to incorporate within and between study components of variance, and fixed-effect models were used secondarily to confirm and compare the results.
Each analysis was assessed for statistical heterogeneity using Cochran’s Q test and I2 statistics. The proportion of between-study inconsistency due to true differences between the studies (rather than differences due to random error or chance) was determined for the I2 statistics. Values >50% were considered to indicate significant heterogeneity. A P-value < 0.1 for Cochran’s Q test was considered statistically significant. 9
Subgroup analyses were pre-planned to compare the following: 1) different scenarios (e.g. with or without chest compression, with or without cervical immobilization, in a car, or at rest); 2) different types of participants (e.g. novice, medical student, physician, or paramedic); and 3) different subject types (e.g. manikin or cadaver).
Results
Identification of studies
The initial literature search revealed 2,042 articles. After duplicate removal, 1,276 publications were excluded because it was clear from the title and abstract that they did not fulfill the selection criteria. We scrutinized the complete texts of the remaining 24 articles and identified 11 potentially relevant articles. The remaining 13 articles were excluded for the following reasons: two were not RCT designs, two were a different study design, eight used different devices, and one was a human study. Eleven studies were therefore finally included in the systematic review11–15,18–23 (Figure 1).

PRISMA flow-chart for retrieval of the 11 randomized controlled trials included in the systematic review. RCT, randomized controlled trial.
Study characteristics
The characteristics of the included articles are summarized in Table 1. All studies were randomized crossover trials using manikins,12–15,18–23 except for one cadaver study. 11 Four studies were original research articles,11,12,14,15 five were correspondence to the editor,13,18–21 and two were poster presentations.22,23 The 11 studies included 558 participants and 3,254 total intubations in 19 situation scenarios. Two trials18,20 in car scenarios were continuation studies undertaken by the same participants, and 513 participants were therefore included in the analyses. However, considering each scenario in a crossover study as an individual parallel study increased the number of participants to 1116. The participants in four studies were physicians,14,15,22,23 six were paramedics,11–13,18–20 and one study involved medical students. 21 No participants had any previous experience with the ETView, and limited experience with cETT intubation in clinical settings (<5 to 19), except in two studies with the same participant in a car scenario18,20 where the participant had a mean of 9.4 career years as a healthcare provider, including experience with approximately 50 tracheal intubations in patients.
Characteristics of the included trials.

Four studies established a scenario with a normal airway at rest (in a neutral position) with no chest compression,11,12,14,15 and four others used a normal airway at rest including chest compression.11,14,21,23 Difficult airway situations requiring manual in-line stabilization were used in three studies,11,12,15,22 cervical immobilization using a cervical extraction collar was used in three studies,12,15,18 and cervical immobilization using a vacuum mattress was used in one study. 15 Another four difficult intubation situation settings were used,13,18–20 including one scenario of face-to-face intubation with a tongue-swelling situation, 18 and two studies with a normal airway car scenario without chest compression.11,12,14,15 In one case, access was through the open driver’s door (reclining seat was not allowed), 20 and the other was a car back-seat scenario with the manikin trapped in the left front seat with the only access to the patient from the back seat. 13
The scenarios were categorized into four types of scenarios: A, normal airway at rest without chest compression; B, normal airway at rest with chest compression; C, cervical stabilization at rest without chest compression; and D, difficult situation without chest compression. Considering that each study had two or three scenarios and was also performed as a crossover design, each participant experienced multiple intubation events, and the intubation event was therefore considered as the unit of analysis.
The devices used in the included studies were the ETView and a cETT with Macintosh laryngoscope. All intubations were performed with a size 7.0-mm tracheal tube.
Quality of included studies
The methodology for the quality assessment of each trial is described in Figure 2.
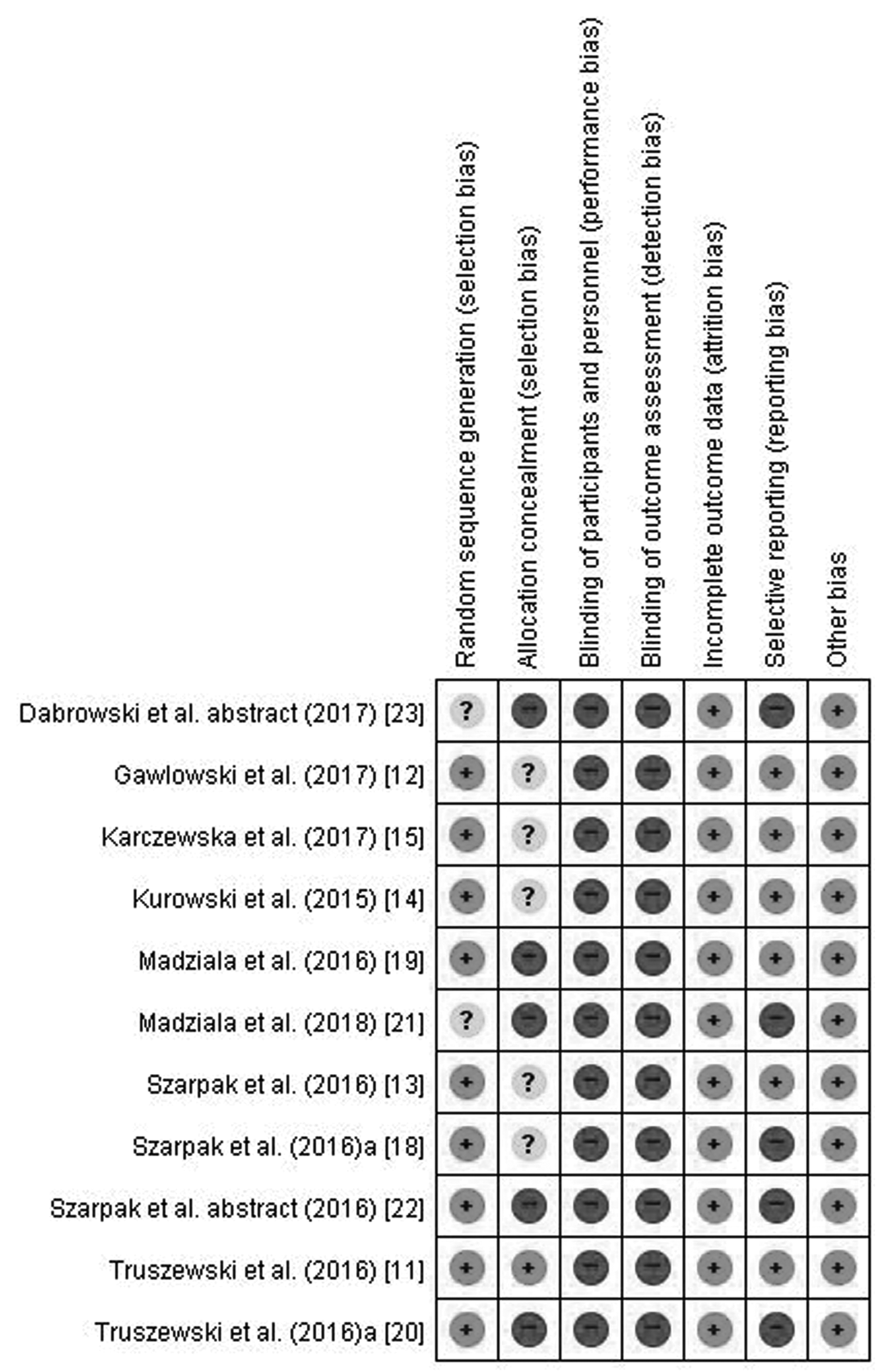
Risks of bias in seven methodological domains. Risk of bias was categorized as low (green), unclear (yellow), or high (red).
Allocation
Eleven of the included studies reported randomization,11–15,18–23 but only nine studies11–15,18–20,22 included information on the random sequence generation method applied. Allocation concealment was adequately reported in only one study. 12
Blinding
Performance and detection bias regarding the blinding of participants and assessors was assessed as having a high risk of bias in all studies.11–15,18–23 It was not possible to blind the participant performing the intubation nor to blind the investigators to the process measures because the device type could not be concealed during the performance.
Incomplete outcome data
All studies reporting the completeness of outcome data for each main outcome were assessed as having a low risk of bias.11–15,18–23
Selective reporting
Six studies were assessed as having a low risk of bias.11,12,14,15,18,19 Five studies13,20–23 where one or more reported primary outcomes were not pre-specified, or not all of the study’s pre-specified primary outcomes had been reported, were assessed as having a high risk of bias.
Other potential sources of bias
All studies had a low risk of other potential sources of bias.11–15,18–23
Meta-analysis of primary outcome measures
Information on the first-attempt success rate was available in all the included studies.11–15,18–23 The analysis demonstrated fewer failed intubations using the ETView in all scenarios (OR: 0.06, 95% CI: 0.04 to 0.10; P < 0.001, I2 = 18%). The pooled OR for the first-attempt success rate (decreased failure rate) in a normal airway at rest without chest compression was 0.05 (95% CI: 0.01 to 0.22, P < 0.001). This result showed no heterogeneity (I2 = 0%), (Figure 3).

Forest plots for first-attempt success rate (displayed as odds ratio for decreased failure rate; events were failure of intubation). M-H, Mantel–Haenszel; df, degrees of freedom.
Meta-analysis of secondary outcome measures
Intubation time was assessed in all the included studies.11–15,18–23 Assessment using a normal airway with or without chest compression and also with an airway situated in a difficult position revealed a significantly shorter insertion time in the ETView compared with the cETT group. The pooled MD for all 17 scenarios was −11.44 s (95% CI: −13.38 to −9.50, P < 0.001), although the heterogeneity was high (I2 = 96%). The pooled MD in four studies using a normal airway at rest without chest compression was −6.05 s (95% CI: −9.62 to −2.48, P < 0.001, I2 = 98%),12–15 and the MD in four studies with difficult situations was −16.82 s (95% CI: −22.67 to −9.50, P < 0.0001, I2 = 98%)11,18–20 (Figure 4).

Forest plots for intubation time (displayed as mean difference in seconds). SD, standard deviation; IV, inverse variation; CI, confidence interval; df, degrees of freedom.
The Cormack–Lehane grade was assessed in five studies,11,12,14,15,21 but detailed data were not reported in one of these. 21 The incidence of Cormack–Lehane grade 1 was significantly higher in the ETView compared with the cETT group in a normal airway at rest without chest compression (OR: 65.20, 95% CI: 12.58 to 338.03, P < 0.001, I2 = 0%), in cervical stabilization (OR: 687.11, 95% CI: 103.85 to 4546.16, P < 0.001, I2 = 38%), and in all nine included scenarios from four studies (OR: 207.99, 95% CI: 68.91 to 627.76, P < 0.001, I2 = 24%)11,12,14,15 (Table 2).
Secondary outcomes in four categorized scenarios.

aEase of use analyzed as standardized mean difference; other outcomes analyzed by odds ratio. ETView, ETView VivaSight single lumen; cETT, conventional endotracheal tube; Scenario A, normal airway at rest without chest compression; Scenario B, normal airway at rest with chest compression; Scenario C, cervical stabilization at rest without chest compression; Scenario D, difficult situation without chest compression; MD, mean difference; CI, confidence interval; N/A, not applicable; M-H: Mantel–Haenszel; IV, inverse variation.
Data on the overall success rate were available in six studies,11–15,22 and showed significantly fewer overall failed intubations in the ETView group in a normal airway situation with or without chest compression, and also with an airway situated in a difficult position (OR: 0.04, 95% CI: 0.01 to 0.15, P < 0.001, I2 = 0%) (Table 2).
The incidence of dental trauma was evaluated in four trials,12–14,20 and was significantly lower in the ETView compared with the cETT group (OR: 0.02, 95% CI: 0.01 to 0.08, P < 0.001, I2 = 0%) (Table 2).
Ease/difficulty of device use was assessed in three studies.12,15,18 The ETView was significantly easier to use than conventional intubation in cervical stabilization and difficult situations (standardized MD, inverse-variance, random-effects: −2.15, 95% CI: −2.47 to −1.83, P < 0.001, I2 = 0% and −3.03, 95% CI: −3.64 to −2.42; P < 0.001, I2 not applicable, respectively), but not in normal airway at rest without chest compression scenarios (−0.02, 95% CI: −0.74 to 0.70, I2 = 87% (Table 2).
Participants were asked about their device preference in four studies.11,12,14,15 The ETView was the preferred device in normal airway at rest without chest compression scenarios (OR: 163.40, 95% CI: 6.82 to 3913.17, P = 0.002, I2 = 95%) and in normal airway at rest with chest compression, with 100% selection (Table 2).
Subgroup analysis
Subgroup analysis was conducted in different types of participants (physicians versus non-physicians, such as medical students and paramedics). The results are summarized in Appendix 2. The ETView group consistently showed a significantly higher first-attempt success rate for intubation and shorter intubation time than the cETT group, regardless of the type of participant (physician or not).
Sensitivity analysis and publication bias
We conducted a sensitivity analysis by systematically removing unpublished articles (abstracts) and high-risk of randomization studies and recalculating the significance of the results to determine if each study influenced the overall results. No study significantly affected the heterogeneity and ORs. Additionally, a cadaver study 12 sensitivity analysis showed that heterogeneity and ORs were not significantly impacted.
Funnel plots were used to evaluate publication bias for the primary outcome. All the funnel plots appeared symmetrical, suggesting a low risk of publication bias. We used the trim and fill method to address publication bias, with a 12% reduction in effect size (2.413, 95% CI, 1.879 to 2.947, to 2.152, 95% CI, 1.658 to 2.646). Egger’s test gave a P-value of 0.06, confirming no significant evidence of a small-study effect (Appendix 3).
Discussion
The results of this meta-analysis showed that implementation of the ETView increased the success rate and shortened the intubation time in simulated studies, compared with conventional intubation using a Macintosh laryngoscope.
The success rate of the first intubation attempt is important because the risks of hypoxemia, aspiration, and even cardiac arrest have been shown to increase significantly after more than two intubation attempts. 24 Furthermore, improving the first-attempt success rate is considered the main goal of emergency intubation. 25 A shorter intubation time is also important in terms of securing airway patency during cardiopulmonary resuscitation, given that recent resuscitation guidelines emphasize that chest compressions should be interrupted only briefly when placing airway devices.26,27 The mean intubation time was 13.47 s faster with the ETView compared with the cETT. This difference may reduce the duration of interruptions to chest compression, thereby contributing to better perfusion of the major organs during resuscitation. Minimizing the hands-off time and maximizing organ perfusion are major factors affecting resuscitation outcome.28,29 In this regard, the ETView may be a critical device for improving patient outcomes during resuscitation. The difference in intubation time between the ETView and conventional intubation was further increased in difficult situations, with a pooled MD for normal at rest airways without chest compression of −6.05 s and a pooled MD in difficult situations of −16.82 s. The benefit of the ETView may thus be highlighted in difficult situations.
The superior success rate and faster insertion time of the ETView versus cETT, which was consistent across all types of scenarios in the current meta-analysis, suggest that the results may be clinically applicable in various conditions, such as during cardiopulmonary resuscitation, neck stabilization, and other difficult situations.
The participants included in this review had no previous experience with the ETView and limited experience with a conventional laryngoscope. However, despite this difference in device familiarity, the results demonstrated a clear advantage of the ETView vs. cETT in inexperienced operators.
In addition, the ETView had better intubation results in terms of a higher rate of Cormack–Lehane grade 1 and a lower incidence of dental trauma compared with the Macintosh laryngoscope.
Cervical immobilization limits the optimal head and neck position, termed the sniffing position. However, the ETView improves intubation conditions in this situation by visualizing the glottis without alignment of the oral-pharyngeal-tracheal axes. The difference in the incidence of Cormack–Lehane grade 1 was substantially increased in stabilization status scenario C, indicating that the ETView may enable faster and easier intubation than the cETT during cervical immobilization.
The ease of use of the two methods was similar in scenario A (normal airway without chest compression), unlike the other scenarios, suggesting that ETView had no advantages in controlled situations, such as typical elective surgery in the operating room. However, intubation outside the operation room is generally much more difficult, and the perceived ease of use of the ETView may thus make it convenient in these situations.
Numerous studies and several meta-analyses have compared video and direct laryngoscopy for endotracheal intubation.30–35 Although the results of these meta-analyses regarding first-attempt success were inconsistent, use of a video laryngoscope decreased failed intubation of difficult airways in some studies.30–32 However, a video laryngoscope did not increase the first-attempt success rates of inexperienced or experienced operators in emergency situations, such as during cardiopulmonary resuscitation or trauma.33–35 The current review, which provides the first meta-analysis comparing a video-mounted endotracheal tube (ETView VivaSight single lumen) with a cETT, clearly showed superior intubation success rates with the video-mounted endotracheal tube in emergency situations. The video-mounted ETView endotracheal tube, instead of a video laryngoscope, may thus offer a better alternative than cETTs in emergency intubation situations.
There was substantial heterogeneity in the pooled data for intubation time in the present meta-analysis because the definition of intubation time differed between the studies: each study specified a different starting time point (e.g. touching the device, or inserting the device into the manikin), resulting in an extremely high level of heterogeneity. This heterogeneity prevented a higher quality meta-analysis of intubation time, and the first-attempt success rate was therefore defined as the primary outcome in our review.
The current review included correspondence and short reports, in addition to original research. The funnel plot displayed a visually symmetrical distribution, qualitatively indicating a low risk of publication bias, and all types of publications were therefore included in our review. The ETView produced consistently superior results, regardless of publication type, in all the included studies.
This study had several limitations. An important intrinsic deficiency in the studies was the difficulty in blinding, which was impossible because of the nature of the airway devices. Second, only simulated studies using manikins or cadavers were included instead of those conducted in clinical settings, and the implications of the results may thus be limited because the outcomes may differ in actual clinical patients. Further investigations in certified clinical settings are therefore necessary to verify the current findings. However, it would be difficult to perform RCTs in simulated emergency situations, such as during chest compression, neck stabilization, and difficult situations, especially with inexperienced personnel because of ethical issues. Simulated studies are therefore important to try and overcome these situational limitations and ethical challenges. Further systematic evaluation of the ETView in patients is also needed to assess its performance in emergency intubation situations, with a potentially high degree of airway soiling and consequent camera blurring.
Conclusions
Our evidence suggests that the ETView can minimize intubation failure and allow faster and easier intubation in simulated studies, compared with cETTs. This advantage is particularly evident in difficult situations, such as during chest compression, cervical stabilization, and outside-hospital settings. The use of the ETView is also likely to improve glottis visualization and reduce the possibility of dental trauma during intubation. These advantages may influence the ease of use and operator preference for the ETView compared with cETT in difficult situations. The ETView, as a video-mounted endotracheal tube, may be useful for emergency intubation performed by inexperienced personnel. However, the current results were based on simulated situations, and the demonstrated advantages of the ETView should be confirmed in further studies in clinical settings.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research was supported by a Korea University Grant awarded to Dr. Young Ju Won from Korea University (Seoul, South Korea).
Supplemental material 1. PRISMA checklist
Appendix 1. Search terms used for database searches.
Appendix 2. Subgroup analysis of first-attempt success rate in physicians and non-physicians.
Appedix 3. Funnel plots of first-attempt success rate,with precision rate (vertical axis) plotted against effect size (horizontal axis). OR,odds ratio;SE(log[OR]),standard error of the log odds ratio.
(A) Funnel plot of observed data from studies.
(B) Funnel plot after application of trim and fill method; observed data from studies with imputed study data