
Abstract
Introduction
Non-valvular cardiac aspergillosis is a rare infection of the pericardium, myocardium or endocardium and is associated with a high mortality. There is a paucity of reports of non-valvular cardiac aspergillosis in critically ill and solid organ transplant (SOT) patients. The majority of cases have been reported in haemato-oncology patients, some of whom have undergone a bone marrow transplant.
Objectives
We describe four cases affected by non-valvular cardiac aspergillosis in the intensive care setting including a systematic review of this extremely rare infection which is associated with high mortality.
Results
All four-patients died but presented with varying clinical, radiological and microbiological evidence of the disease. Three patients presented following complications after solid organ transplantation, two in the context of acute liver failure and emergency liver transplant and one several years after a double lung transplant. The last patient presented with necrotising gall stone pancreatitis, multi-organ failure and subsequently a prolonged intensive care unit (ICU) stay. On review of the literature, January 1955 to July 2019, 45 cases were identified, with different risk factors, clinical and radiological manifestations, treatment regimen and outcome.
Conclusion
Antemortem diagnosis of cardiac aspergillosis is difficult and rare, with no cases reporting positive blood culture results. Galactomannan serology has poor sensitivity in solid organ transplant patients, further reduced by prophylactic antimicrobial treatment, which is common in the ICU setting especially post-transplant patients. Due to the scarcity of cases, treatment is extrapolated from invasive aspergillosis management, with emphasis on early treatment with combination therapy.
Introduction
Non-valvular cardiac aspergillosis is a rare infection of the pericardium, myocardium or endocardium and is associated with a high mortality. It is characterised by formation of large mural vegetations and peripheral embolisation. The main cause of spread is from fungaemia and systemic embolisation resulting in dissemination to almost every major organ system including respiratory, the gastrointestinal tract, central nervous system and the heart. 1,2 Endomyocardium or pericardium can be directly invaded through a separate mechanism via dissemination of fungi to the left atrial wall and pulmonary veins or through direct pericardial invasion following invasive pulmonary aspergillosis.3,4
Although non-valvular cardiac aspergillosis has a predilection for the immunocompromised, cases have been reported in young immunocompetent patients, frequently with fatal consequences.5,6 There is a paucity of reports of non-valvular cardiac aspergillosis in solid organ transplant (SOT) and immunocompetent individuals. The majority of cases have been reported in haemato-oncology patients. Here we report a case series of four patients admitted to Intensive Care Units (ICUs) of a tertiary referral institution who presented in multiple organ failure (MOF) with diverse risk factors for non-valvular cardiac aspergillosis and a review of the literature.
Cases
Two patients, #1 and #2, underwent emergency extended right lobe auxiliary partial orthotopic liver transplant (APOLT) for intentional acetaminophen overdose and emergency liver transplantation (ELT) for polypharmacy overdose, respectively. In both cases, there were no co-morbidities, but patients required pre- and post-operative multiorgan support in the form of vasopressors, mechanical ventilation and continuous veno-venous haemodiafiltration (CVVHDF). Both patients were started on dual immunosuppressive therapy immediately post-operatively as per hospital protocol. Case #1 received Dacluzimab (CD25 monoclonal antibody) for presumptive acute cellular rejection (ACR) 13 days after her transplant. Case #3, admitted with Type 1 Respiratory Failure and seizures, was also immunosuppressed as their past medical history included double lung transplant as well as panhypogammaglobulinaemia. The only case without history of immunosuppressed state was patient #4, who was admitted to the ICU with MOF secondary to gallstone pancreatitis.
Apart from case #2, all patients were started on empirical antibiotics and antifungals for sepsis, whereas case #2 was on prophylactic fluconazole and intravenous antibiotics (tazobactam-piperacillin) as part of the post liver transplant protocol not for treatment of sepsis. All three patients with clinical signs of sepsis went on to have computer tomography (CT) of the chest, with only case #1 demonstrating the stereotypical halo sign indicative of pulmonary aspergillosis (Figure 1). Case #3 and #4 had non-specific pulmonary features of bilateral widespread ground glass changes and wide-spread bilateral consolidation, respectively. In case #4, CT chest showed multiple hypodense lesions throughout the left ventricular myocardium, the largest lesion measuring more than 2.2 cm in diameter.
Computer Tomography of the chest demonstrating multiple focal areas of consolidation in both lungs, with halo sign suspicious of angioinvasive fungal infection.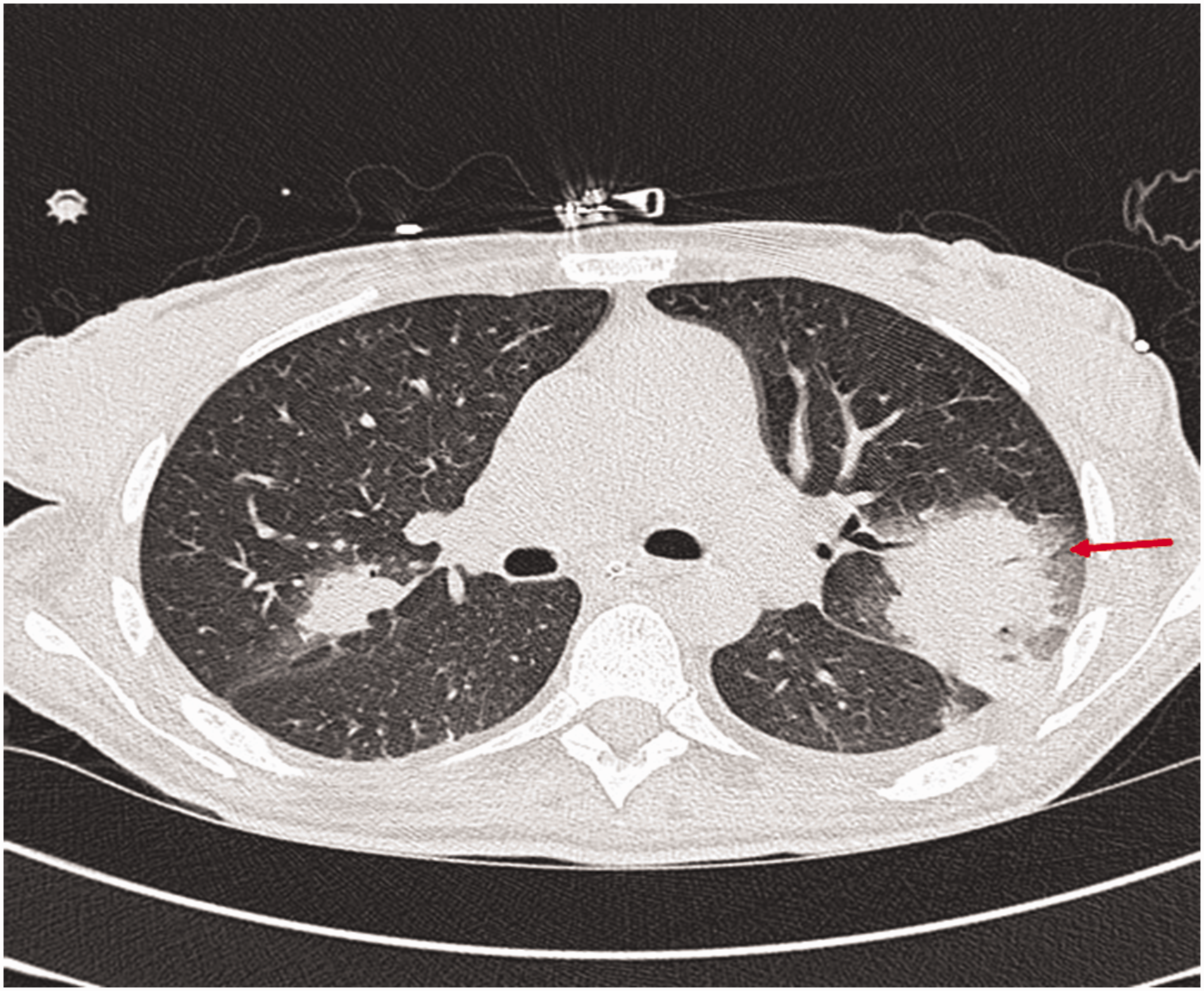
All patients showed evidence of embolic disease ante-mortem, some of which were prior to identification of cardiac infection. Evidence of embolic disease in case #2, multiple areas suspicious of infarcts/septic emboli on CT and confirmed on MRI brain (Figure 2), led to the suspicion of infective endocarditis. In addition to cerebrovascular disease, case #2 had CT features confirming infarction of kidneys and the spleen ante-mortem. Patient #3 was the only one that did not show evidence of cerebrovascular embolic disease ante-mortem but did have an occlusion of the descending aorta with thrombus causing bilateral ischaemic limbs. Embolic disease was not the only sequalae of cardiac aspergillosis, however; case #4 required insertion of a temporary pacing wire due to sustained multiple episodes of prolonged sinus arrest as did case #1 for narrow complex junctional escape bradycardia.
Magnetic resonance imaging (MRI) confirming left cerebral hemisphere infarct indicative of embolic infarction.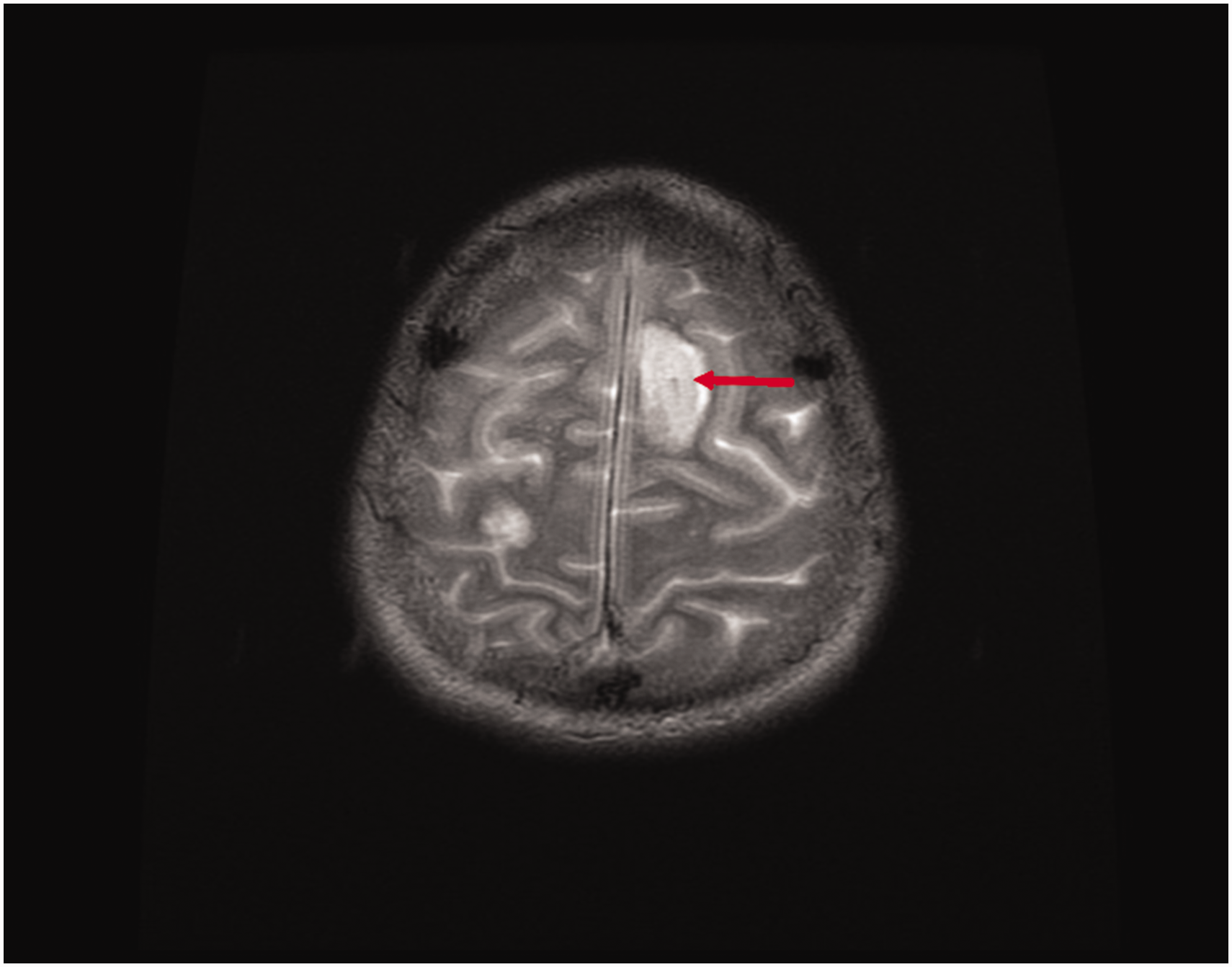
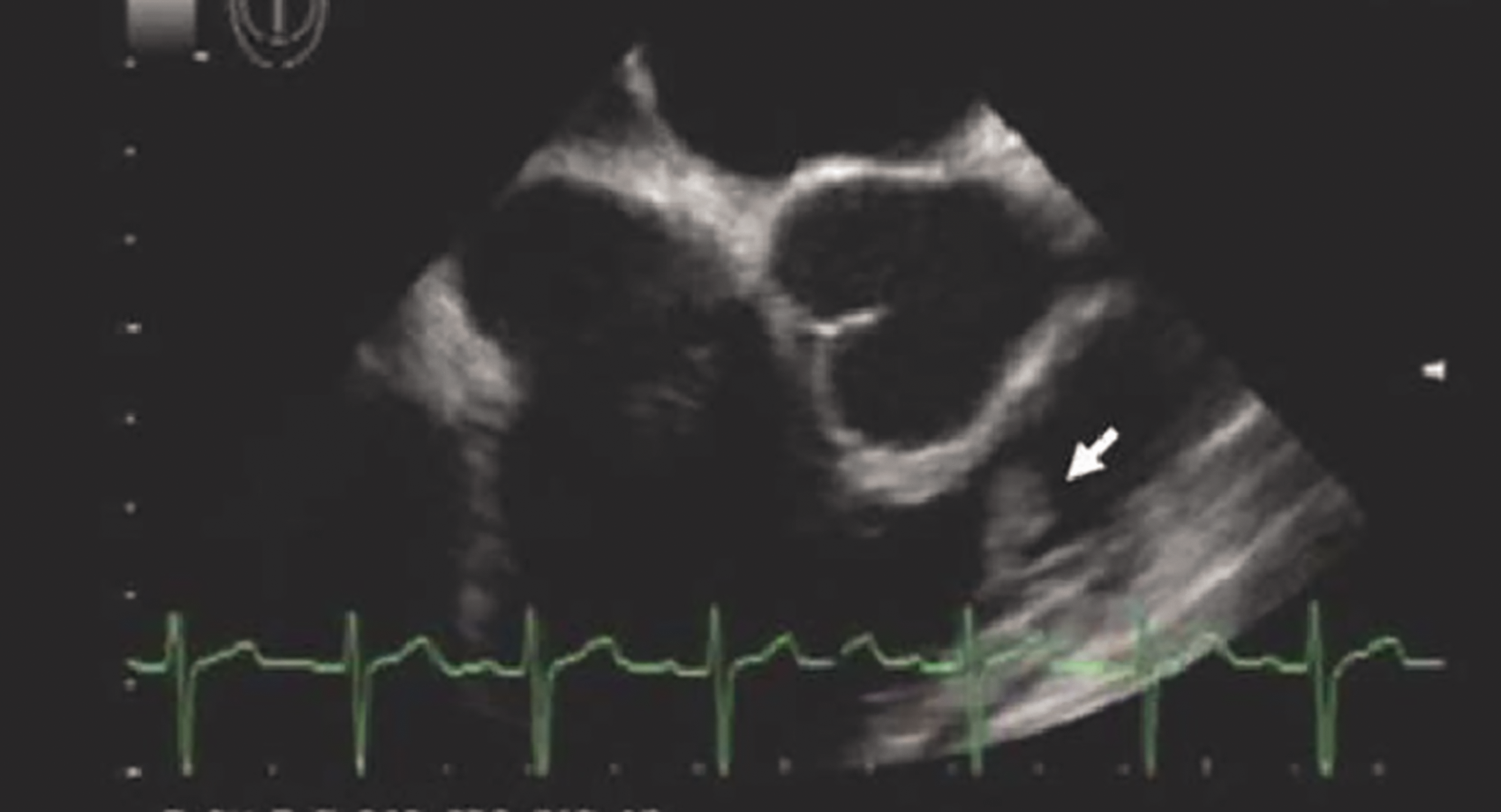
All cases had findings indicative of an infective carditis on Transoesophageal Echocardiogram (TOE), but echocardiographic image characteristics differed for each patient. Case #1's TOE showed a large, mobile lesion at the antero-septal aspect of the left ventricular outflow tract compatible with vegetation and mild-to-moderate mitral regurgitation, but no flail leaflet or valvular vegetation (Figure 3). Case #2 showed a mobile lesion in the right ventricular outflow tract, too distal in location for a moderator band, but no evidence of pulmonary or tricuspid valve incompetence (Figure 4). Although TOE in case #3 showed vegetation of mitral and aortic valves, post-mortem histology showed invasion of branching hyphae into the myocardium around the mitral ring, but no valve leaflet involvement. In case #4, the TOE confirmed the findings on CT chest of multiple round ovoid lesions throughout the left ventricular myocardium.
Transoesophageal Echocardiagram showing a large, mobile lesion at the antero-septal aspect of the left ventricular outflow tract, but no flail leaflet or valvular vegetation. Transoesophageal Echocardiogram showing a mobile lesion in the right ventricular outflow tract, but no evidence of valve incompetence.
Only case #4 did not have a post-mortem, but had convincing clinical, radiological and microbiological evidence of cardiac aspergillosis. A white mass was identified in the right upper lobe segments on bronchoscopy and cultures of the biopsy grew aspergillus fumigatus. Additionally, broncho-alveolar lavage (BAL) galactomannan tested strongly positive. Post-mortem examination of case #2 showed evidence of multiple abscesses involving both cerebral hemispheres, thalami, left upper lung lobe, pericardium, endocardium and myocardium, but no valvular abnormalities or vegetation. Microscopic examination of these abscesses revealed branching hyphae consistent with aspergillus infection (Figure 5). Post-mortem of case #1 also had branching fungal hyphae on microscopic examination of abscess involving the myocardium, as well as left lung, thyroid gland, brain and kidneys.
Histopathology slide revealing branching hyphae in myocardium consistent with aspergillus infection.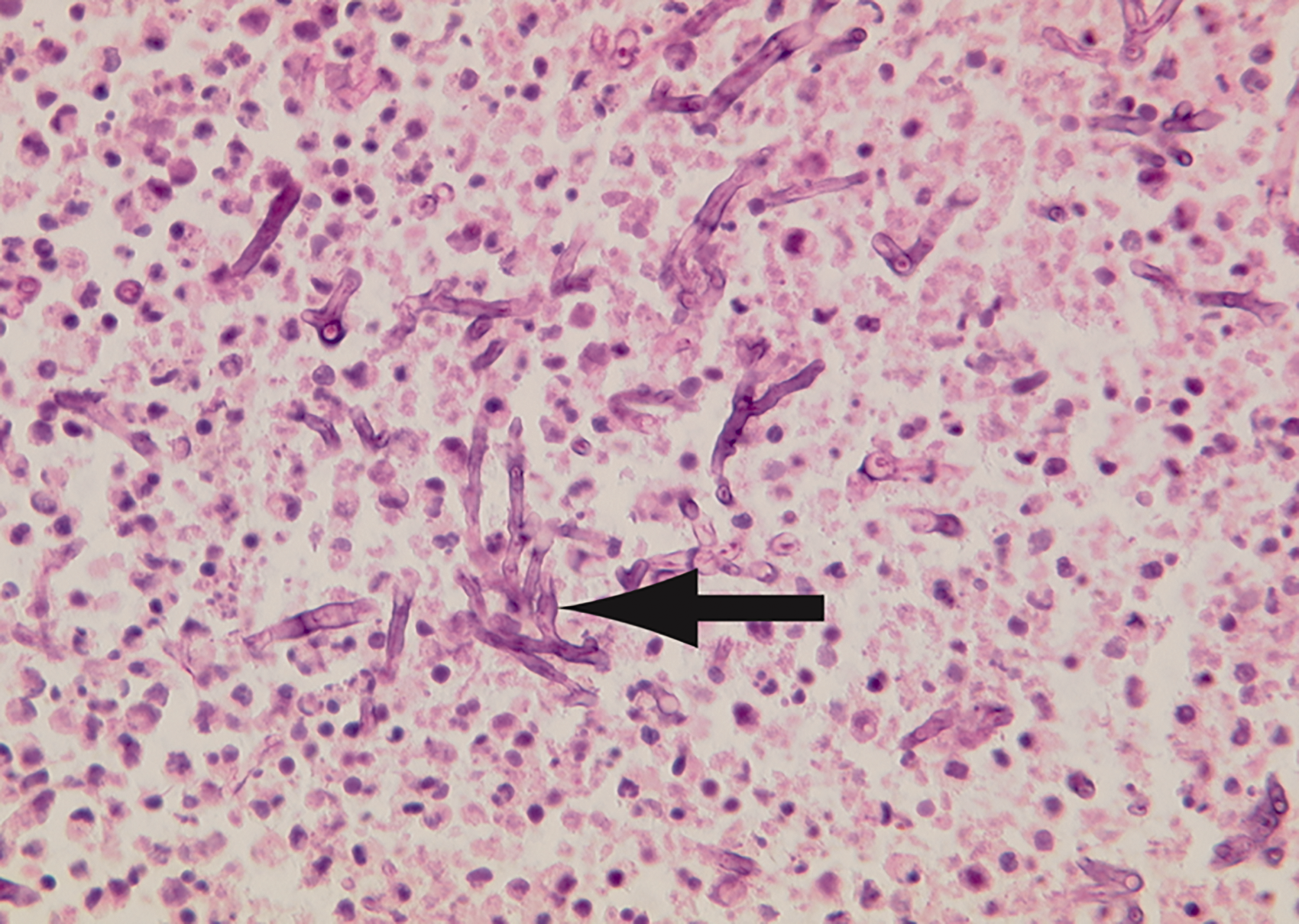
Demographics, past medical history, echo findings and antifungal therapy of case series described.
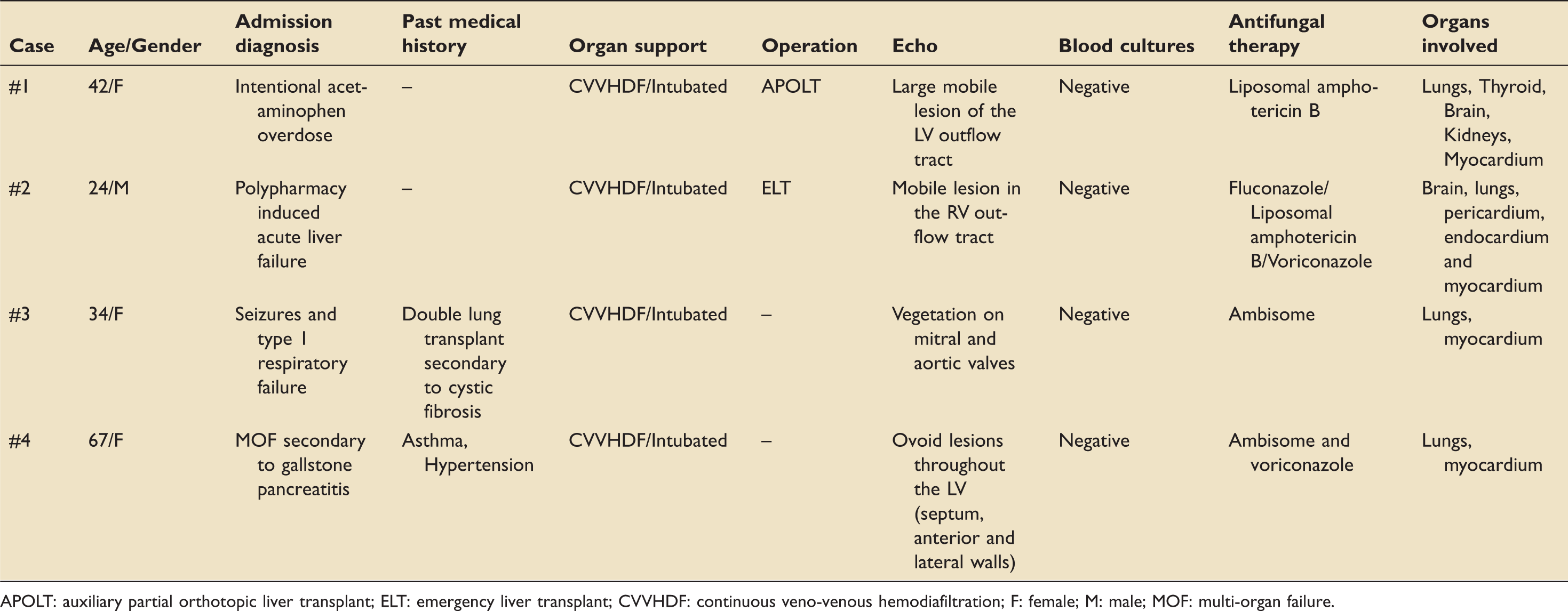
APOLT: auxiliary partial orthotopic liver transplant; ELT: emergency liver transplant; CVVHDF: continuous veno-venous hemodiafiltration; F: female; M: male; MOF: multi-organ failure.
Systematic review of non-valvular aspergillus carditis
We conducted a Medline database search from January 1955 to July 2019. The terms used for the search were ‘aspergillosis’, ‘aspergillus’ or ‘aspergilloma’ combined with the terms ‘non-valvular’, ‘myocarditis’, ‘pancarditis’, ‘pericarditis’ or ‘endocarditis’. This provided 599 abstracts of manuscripts and conference presentations. Reviewing the title and abstracts, all items that had a reference to non-valvular endo-/myo-/peri-/pancarditis due to aspergillus infection were included. Of these, any manuscripts that reported on cases under 18 years of age, were not written in English or were conference abstracts were excluded. On reviewing full manuscripts, any cases that had aspergillosis secondary to pacemaker wires were also excluded. Of the 47 papers included, full access to manuscripts was not possible in seven. Please see Supplemental information 1 for table of cases with associated summaries.
Results
Our literature search produced 599 papers, 507 of which were excluded based on their title and abstract. Of the remaining 92, 52 were excluded after reviewing the contents of the full article (seven of which had inaccessible manuscripts and 10 were not written in English). There were 40 papers that reported a total number of 45 cases of aspergillus carditis with no involvement of the valve leaflets (Figure 6).
Diagram of systematic review process.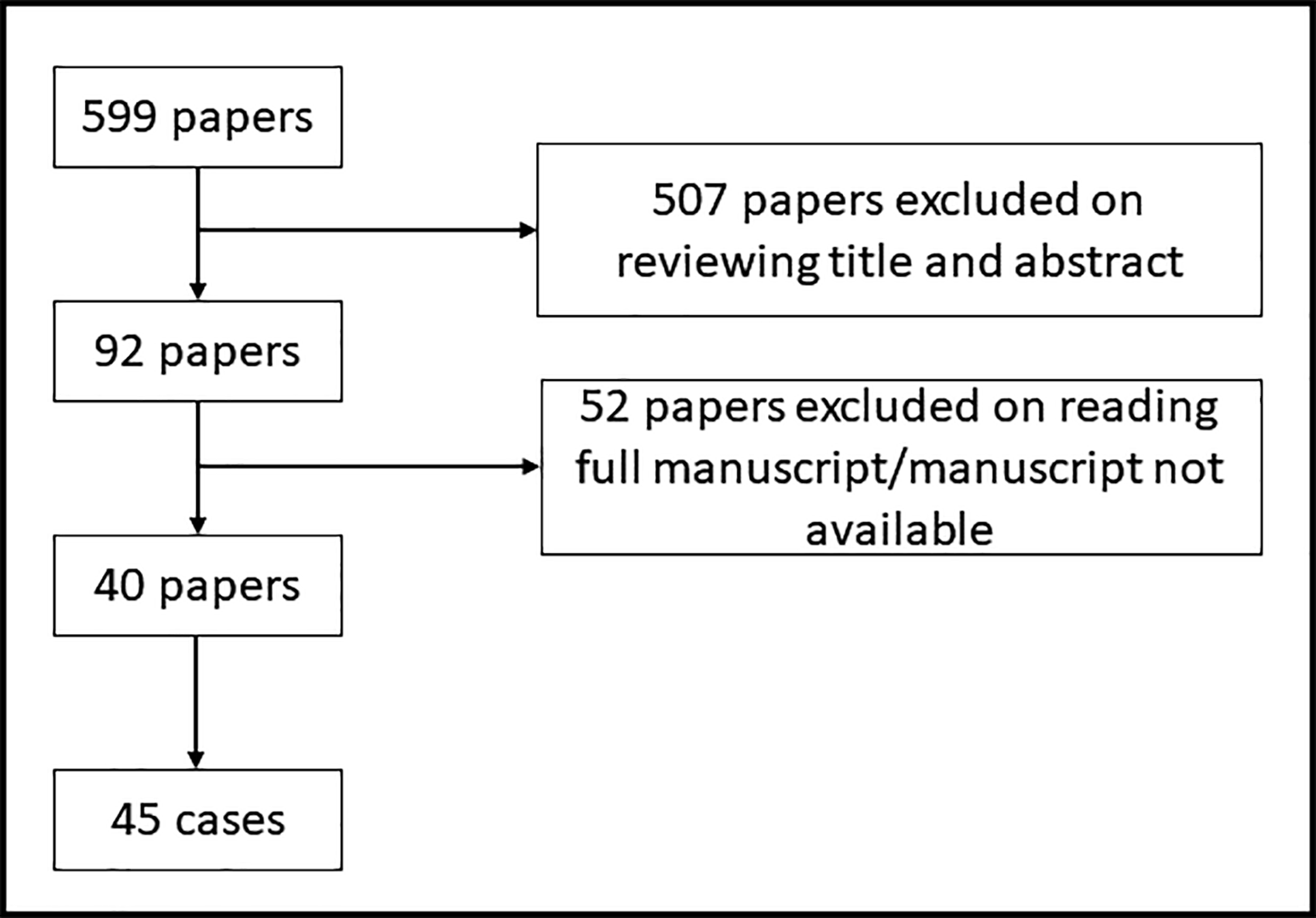
Patient demographics
The mean age was 43 years (range 18–75), with male preponderance (66.7% vs. 33.3%). The majority of individuals were immunocompromised/immunosuppressed (73.3%, n = 33), with 12 being transplant patients (solid organ or bone marrow). Others were receiving chemotherapy, long-term steroids, had acquired immunodeficiency syndrome (AIDS) or inherited immunodeficiency disorder.
Pathology
Classifying cases into pericardial, myocardial or endocardial (not including valve leaflets) related pathologies, 30.6% (n = 19), 45.2% (n = 28) and 24.2% (n = 15), respectively, reported above infection locations. Of these, 13 cases had a mixed picture including pancarditis being described in four patients. Only one case had positive blood cultures and only four reported positive galactomman results. A total of 10 cases did not have confirmation by pericardial/cardiac tissue histopathology but were diagnosed by clinical, radiological and microbiological evidence.
Outcome
Thirty-seven of 45 patients died. Aspergillus infection was suspected in 20 cases as they were started on some form of antifungal treatment, 13 of which diagnosed aspergillus carditis only ante-mortem. A total of 17 cases were not started on any antifungal intervention and not diagnosed with aspergillus carditis ante-mortem.
Discussion
We report four adult ICU cases of non-valvular aspergillus carditis; the first in a double lung transplant recipient. All cases were critically ill, requiring CVVHDF, mechanical ventilation and vasopressor support. Despite differences in immune status, co-morbidities and reason for being admitted to the ICU, the only risk factor shared by all cases was MOF. Risk factors associated with aspergillus pancarditis include heart valve replacement, acquired immunosuppressive or lymphoproliferative disorders and prolonged granulocytopenia.7,8 Given the paucity of information on this disease, other risk factors for invasive aspergillus (IA) must also be considered such as old age, bone-marrow transplant, need for mechanical ventilation or renal replacement therapy (RRT), all of which are associated with poor outcomes. 9
Among non-valvular aspergillus carditis cases, both our case series and the systematic review did not appear to show a particular age preponderance. Furthermore, 27.7% (n = 12) were not immunocompromised prior to admission but were critically unwell. Information regarding corticosteroid therapy whilst on ICU, however, was not reported; this could predispose patients to opportunistic infections through quantitative and qualitative functional impairment of macrophages and neutrophil function. 10 Although not commonly reported in the context of stress doses of hydrocortisone, prolonged steroid therapy in other indications such as alcoholic hepatitis and treatment for COPD has previously been associated with invasive mould infections.
IA is inherently difficult to diagnose, with it being the most frequently missed infection on autopsy among patients requiring ICU admission. 11 Isolation of the organism from blood cultures is extremely uncommon, which is further demonstrated by only one case in the systematic review having positive blood cultures. 12 Aspergillus galactomannan serology has only 55% sensitivity in solid organ transplant recipients. The sensitivity of the test further decreases to 20% if patients are exposed to antifungal medication, which is common practice post-transplant where most patients receive universal or targeted antifungal prophylaxis. 13 Sensitivity is also limited in non-neutropenic patients undergoing RRT and in patients receiving penicillin-containing antibiotics, such as piperacillin – tazobactam, which was used in all our cases. The latter is due to cross reactivity because of the close structural resemblance of aspergillus and penicillium cell wall. 14
Diagnosis is further complicated by incapacity to differentiate colonisation from infection, as impact of Aspergillus spp isolates from respiratory cultures on the occurrence of IA is poorly understood in non-immunocompromised patients, including ICU patients.15–17 CT imaging of the lungs typically shows halo sign and crescent sign in the presence of pulmonary aspergillus, but these lack specificity in critically ill patients. 18 Echocardiography maybe the most relevant investigation, but in non-valvular cardiac aspergillosis only 18 out of 45 cases reported abnormal echocardiography results (please see Supplemental information).
Non-valvular aspergillus carditis is universally fatal, with only eight cases reported in the literature where treatment has been successful (please see Supplemental information). The heterogeneity of the cases reported makes treatment recommendations difficult. Voriconazole was used in four out of the eight cases, in conjunction with other anti-fungal agents as well as surgical interventions.19–22 Use of voriconazole has been associated with better survival in organ transplant recipients as well as with other forms of IA compared to amphotericin B.23,24 There are concerns, however, with regards to its interaction with immunosuppressive agents (i.e. tacrolimus, cyclosporine, sirolimus) via inhibition of the cytochrome P450 isoenzyme, therefore limiting its use in the post-transplant setting. 25 Intravenous voriconazole is probably safe to use in patients undergoing RRT as CVVHDF has been found to effectively remove sulfobutylether-β-cyclodextrin, a potentially toxic renally excreted conjugate.26,27 In cases where voriconazole cannot be used, liposomal amphotericin has a higher efficacy than amphotericin B for systemic aspergillosis, and high dose (10 mg/kg/day) therapy may be preferable where there are concerns around poor tissue penetration such as during endocarditis or pancarditis.8,28,29
Consideration of the pharmacological complexity of ICU patients is essential when deciding which combination of antifungals is being used. Especially in use of the triazoles, as risk of encephalopathy, hepatoxicity and visual disturbance associated with voriconazole are concentration dependent, which is one of the reasons why the British Society of Medical Mycology encourages therapeutic drug monitoring (TDM). 30 Further evidence encouraging TDM includes randomised control trial that showed higher rate of either complete or partial response in patients who had TDM than those that didn't. 31 Specifically with voriconazole, genetic polymorphism CYP2C19 means TDM is needed for both oral and IV treatment. 30 With amphotericin B, however, there is not enough concentration variability in dose-exposure relationship to warrant TDM. 30 Given the unpredictable pharmacokinetics in critically ill patients, or those with severe renal or hepatic dysfunction, TDM is encouraged if triazoles are included in multi-antifungal treatment strategies.
Conclusion
We report four cases of non-valvular cardiac aspergillosis; the first case in a patient with a past medical history of double lung transplant patient. The case series and systematic review demonstrate a significant heterogeneity in demographics, risk factors and echocardiographic findings. Mural cardiac aspergillosis is extremely rare and associated with high mortality regardless of age and immunocompetence. In vivo diagnosis of the disease is rarely made and requires a high index of suspicion. Early treatment is crucial; extrapolating from data reported for IA infections, combination therapy is currently the most effective medical treatment to successfully manage this condition in intensive care patients.
Supplemental Material
sj-pdf-1-inc-10.1177_1751143720936821 - Supplemental material for A case series of non-valvular cardiac aspergillosis in critically ill solid organ transplant and non-transplant patients and systematic review
Supplemental material, sj-pdf-1-inc-10.1177_1751143720936821 for A case series of non-valvular cardiac aspergillosis in critically ill solid organ transplant and non-transplant patients and systematic review by Annalan MD Navaratnam, Mohammad Al-Freah, Anna Cavazza and Georg Auzinger in Journal of the Intensive Care Society
Footnotes
Acknowledgements
The authors would like to acknowledge the hardworking staff at the King's College Hospital, delivering high-quality patient care and putting patient safety as a priority.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics and consent
Informed written consent was obtained from the next of kins for all patients presented in this case series. Ethics approval was not required for the systematic review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.