
Abstract
This primer summarizes the diagnosis, treatment, complications, and prognosis of anti-N-methyl-
Introduction
Anti-N-methyl-
This immune-mediated encephalitis is often paraneoplastic and associated most commonly with ovarian teratoma. 6 Other neoplasms associated with NMDA-r include Hodgkin lymphoma 7 as well as testicular, lung, and breast cancers. 3 However, many patients lack a clear trigger, and one case series of 44 patients found that the majority of cases were not associated with a neoplasm. 8 Another identified risk factor is a history of herpes simplex virus-1 (HSV-1) encephalitis, where a study of 51 patients with HSV encephalitis found that 27% went on to develop autoimmune encephalitis, with 9 of the 14 patients developing autoimmune encephalitis having NMDA-r antibodies.9–11 Patients characteristically start with a constellation of cognitive and behavioural symptoms such as delusions, hallucinations, and/or catatonia, and therefore, may present to psychiatry.5,6 This usually follows a subacute course, evolving into movement disorders such as chorea, dystonia, and stereotypies, 12 in addition to altered mental status, and ultimately involving the neurology service. 5 Intensive care unit staff usually become involved with the subsequent development of seizures, status epilepticus, and profound dysautonomia, resulting in cardiac arrhythmias, hyperthermia, hypoventilation, and coma. However, patients may present early with seizures and in status epilepticus, warranting earlier ICU involvement.
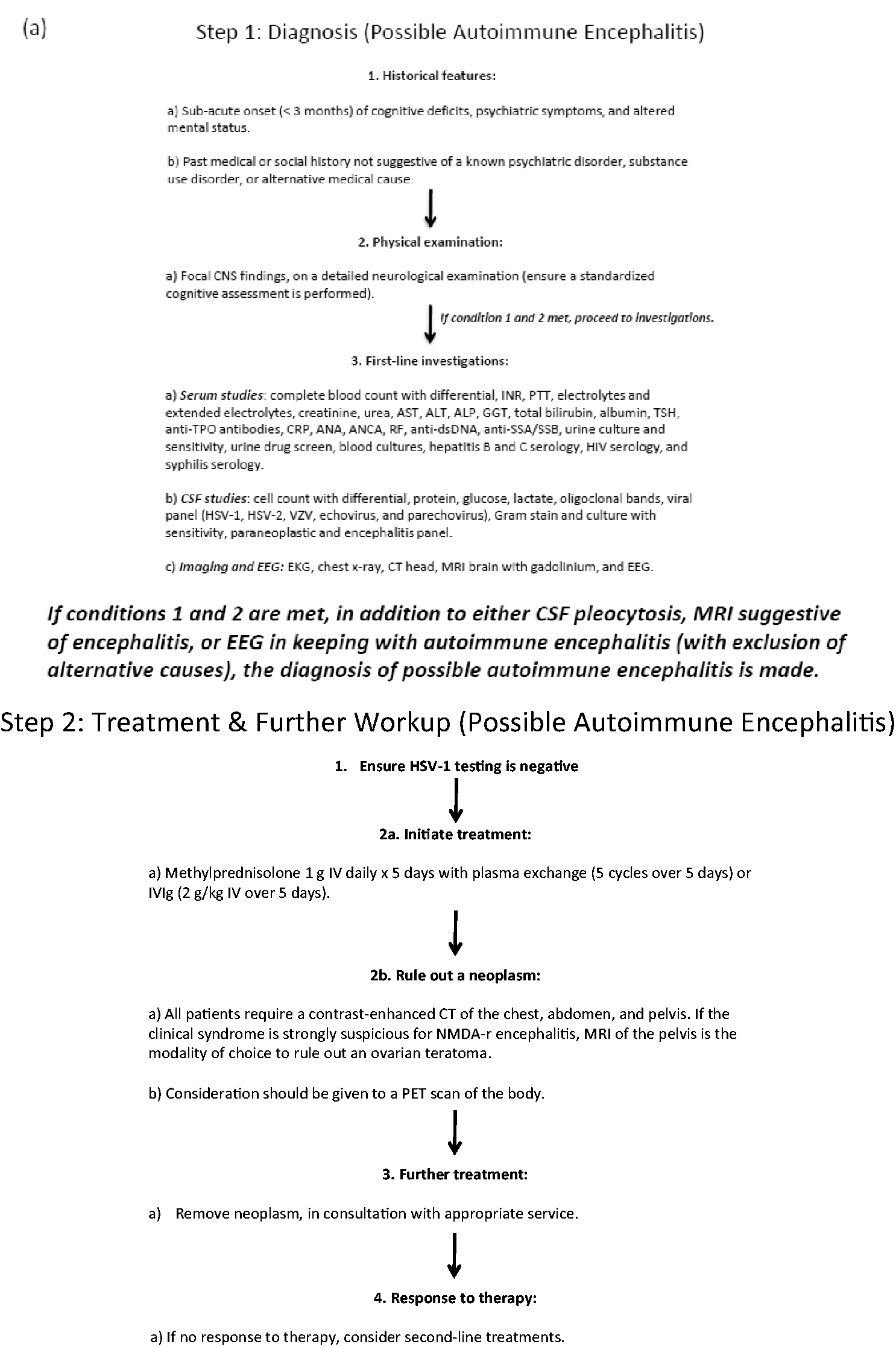
In addition to highlighting key points about NMDA-r encephalitis (Figure 1), this review summarizes the steps required to secure an early diagnosis and spur expeditious and aggressive management (Figure 2(a) and (b)). We also outline unique complications, and what to do when first-line treatments fail. Importantly, a diagnosis of NMDA-r encephalitis can cause considerable emotional toll on families and HCPs, given its protracted course and dramatic symptoms. It is important to emphasize that it has a generally favourable long-term outcome with high-quality survival (Figure 3). Accordingly, ongoing ICU effort and resources are justified, and patients, HCPs, and families may benefit from support and counselling (Figure 4).
Ten summary points for ICU staff related to NMDA-r encephalitis. Algorithmic approach to NMDA-R encephalitis. ALP: alkaline phosphatase; ALT: alanine transaminase; ANA: antinuclear antibody; ANCA: anti-neutrophil cytoplasmic antibodies; AST: aspartate aminotransferase; CNS: central nervous system; CRP: c-reative protein; CSF: cerebrospinal fluid; CT: computed tomography; EEG: electroencephalogram; EKG: electrocardiogram; GGT: gamma-glutamyl transferase; HSV-1: herpes simplex virus-1; INR: international normalized ratio; IVIg: intravenous immunoglobulin; MRI: magnetic resonance imaging; NMDA-r: anti-N-methyl- The mRS. Resources for families following the diagnosis of NMDA-r encephalitis.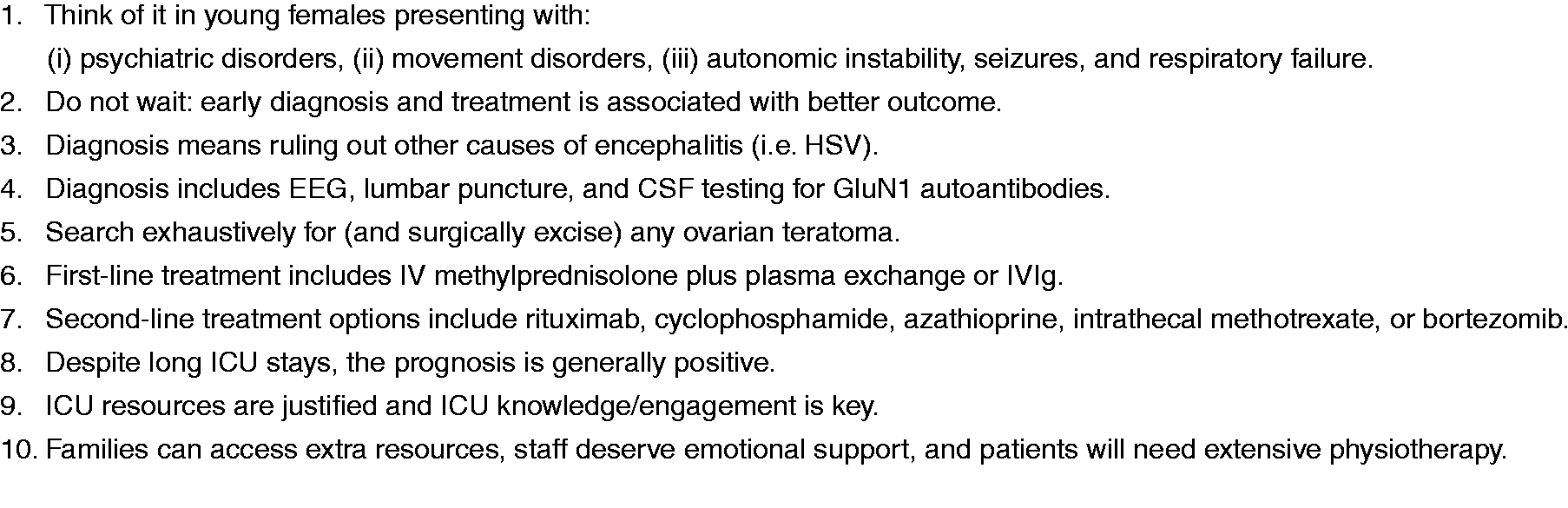
Diagnosing NMDA-r encephalitis: Chance favours a prepared mind
Diagnosis starts with a thorough history and physical exam, followed by laboratory confirmation. ‘Probable NMDA-r encephalitis’ incorporates three criteria: (1) a rapid onset (over less than three months) of at least four of the following symptoms: abnormal behaviour or cognitive dysfunction, speech dysfunction, seizures, movement disorder, decreased level of consciousness, autonomic dysfunction or central hypoventilation; (2) abnormal electroencephalogram (EEG) (i.e. extreme delta brush) or abnormal cerebrospinal fluid (CSF) with pleocytosis or oligoclonal bands; and (3) reasonable exclusion of other disorders, most notably primary psychiatric disorders, exposure to drugs or toxins, CNS infections, alternate immune mediated conditions, or metabolic disorders. 13 ‘Definite NMDA-r encephalitis’ is made following the detection of CSF antibodies to the GluN1 subunit of the NMDA receptor. 13
In five years, our institution has had 27 patients with definite NMDA-r encephalitis. Just over half (14/27) required ICU involvement before definitive diagnosis. Thus, acute care HCPs play an important collaborative role in caring for these patients and their families. This is emphasized by the association between worse outcome and delays in diagnosis and treatment.1,4–6,14 Intensive care unit HCPs should also understand that there are many forms of encephalitis (i.e. autoimmune, paraneoplastic, and infectious), and the approach to diagnosis, treatment, and outcomes differs.
Following multidisciplinary input (neurology, psychiatry, infectious diseases, and intensive care), along with established criteria, 13 we developed an algorithmic protocol (Figure 2). This is intended to summarize and expedite diagnosis and treatment. It is informed by local experience and worldwide literature. Diagnostic tests include (i) serum studies, (ii) CSF analysis, (iii) EEG, and (iv) imaging studies. Serum studies serve to rule out systemic inflammatory or infectious conditions. CSF analysis is employed to rule out infectious causes of encephalitis (especially HSV-1), to identify a lymphocytic pleocytosis or CSF-specific oligoclonal bands, and to identify GluN1 autoantibodies. Notably, CSF is more sensitive than serum for the NMDA-r antibody, 15 and therefore, should be tested even in the absence of serum antibodies. Either flow cytometry or cell-based assays can be used to detect NMDA-r antibodies with cell-based assays appearing to have higher sensitivity without compromising specificity. 16
Magnetic resonance imaging (MRI) of the brain with and without gadolinium is often unremarkable in NMDA-r encephalitis patients.17,18 However, MRI is still recommended to rule out other mimics including inflammatory, infectious, or neoplastic lesions of the CNS. EEG can be useful, as it is rarely normal in patients with NMDA-r encephalitis; the pattern of extreme delta brush is highly specific. 19 Moreover, EEG abnormalities correlate with the need for ICU admission and prolonged recovery time. 20
Treatment: Multipronged, aggressive, and expeditious
Treatment should start without delay once HSV-1 testing (either by polymerase chain reaction or serological analysis) is confirmed negative in CSF. If there is low suspicion of HSV encephalitis and features suggestive of NMDA-r encephalitis (see above), treatment should be initiated promptly. First-line treatment includes intravenous methylprednisolone (1 g daily for five days), alongside either plasma exchange (five cycles over five days) or intravenous immunoglobulin (IVIg) (2 g/kg IV over five days) (Figure 2). Our local preference is to use plasma exchange rather than IVIg providing the patient is cooperative. For psychotic or agitated patients, plasma exchange includes the risk of patients pulling out their central lines. In these cases, we either judiciously sedate or use IVIg instead.
Alongside expeditious treatment, it is important to thoroughly investigate for a neoplasm with computed tomography (CT) of the chest and abdomen. We order pelvic MRI for an ovarian teratoma because pelvic ultrasound can miss a small teratoma. Moreover, there should be a low suspicion for diagnostic laparoscopy, if all imaging modalities are normal. If a neoplasm is found it should be surgically removed. If no neoplasm is found, we perform whole body positron emission tomography (PET). Still if a neoplasm is not detected, PET body or CT of the chest, abdomen, and pelvis and MRI of the pelvis should be repeated at regular intervals. This is because of case reports of ovarian teratomas detected years after initial presentation of NMDA-r encephalitis. Dalmau and colleagues recommend screening for ovarian teratomas for at least two years after initial presentation regardless of recovery. Although not currently standard practice, there are case reports of exploratory laparotomies where occult ovarian teratomas were discovered and removed, with subsequent improvement in the patient’s clinical status.21,22
When primary treatments fail (do not give up)
Treatment failure is defined as little to no clinical response after four weeks of treatment. Currently, there is no standardized approach to second-line treatment, if the first-line combination of pulsed steroids, plasma exchange, and/or IVIg fails. Justifiable second-line options include rituximab,5,22 cyclophosphamide, 5 azathioprine, 24 and intrathecal methotrexate. 25 High-quality evidence for these therapeutic agents is lacking in the setting of NMDA-r encephalitis, and their rationale comes from their effectiveness in other autoimmune conditions.
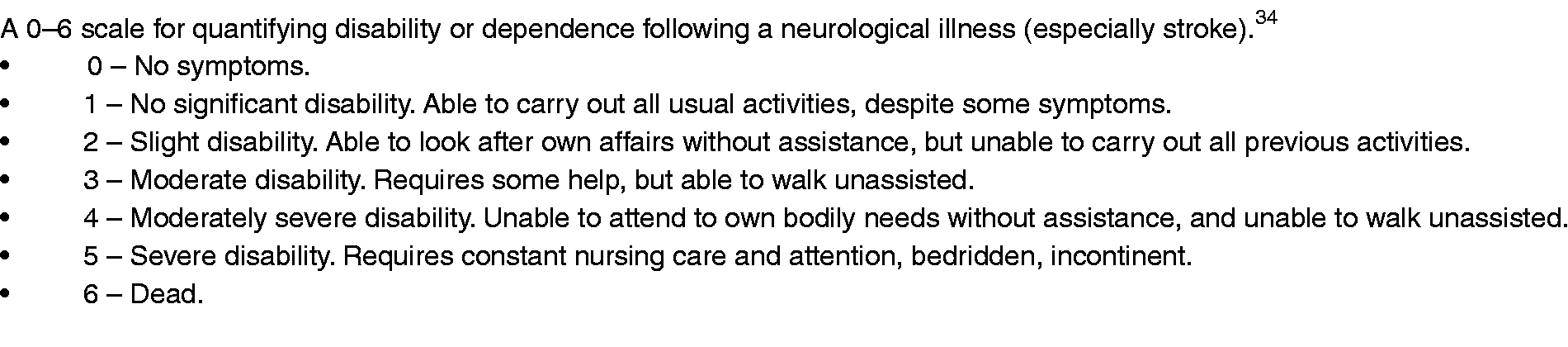
Aside from the aforementioned second-line agents, bortezomib has shown benefit in small case series of refractory NMDA-r encephalitis. This proteasome inhibitor is approved for use in multiple myeloma and functions by depleting plasma cells. 26 In one case series of five patients, bortezomib was associated with clinical improvement and a concomitant decrease in NMDA receptor antibody titres in all but one patient. 27 Separately, in a report of two cases, both patients benefited from bortezomib, one of whom received the therapy following relapse. 28 In a third case series of five patients with refractory disease, some of the patients showed some clinical improvement and a reduction in antibody titres, but did not improve their modified Rankin score (mRS score; see Figure 3 for a description of this useful functional scoring system). 29 Locally, we have used bortezomib in five refractory NMDA-r encephalitis cases and witnessed subjective improvement in all five. Furthermore, the safety profile of bortezomib appears to be favourable.27,28 Accordingly, and while more study data are required, this agent has been added to the arsenal of immune treatments for refractory NMDA-r encephalitis.
Complications for patients with NMDA-r encephalitis
In the acute phase of the illness, complications include seizures, dysautonomia, central hypoventilation, movement disorders, agitation, and catatonia. Dysautonomia most often presents with bradycardia and tachycardia, hypotension and hypertension, hyperthermia, and hypersalivation. 6 Bradycardia can be significant enough to necessitate cardiac pacing. 6 Central hypoventilation can disrupt the patient’s synchronization of breathing. This can prolong the need for mechanical ventilation (necessitating tracheostomy and a percutaneous feeding tube) and cause ventilator dyssynchrony (delaying ventilatory weaning and ward transfer).
Movement disorders associated with NMDA-r encephalitis are a highly disabling patient complication. Movement disorders are also extremely emotionally distressing for families and HCPs. They often present later and include choreoathetosis, dystonia, stereotypies, ballism, catatonia, myoclonus, and opisthotonos.5,12 Oro-lingual-facial dyskinesias are common and can cause mouth trauma such as tongue laceration and broken teeth. 6 Bite blocks may mitigate such injuries. Currently there is no accepted approach to managing NMDA-r encephalitis associated movement disorders. Dopamine depleting agents such as tetrabenazine, deutetrabenazine, and valbenazine have been described in the literature as potential options for treating hyperkinetic movement disorders. 30 We have employed botulinum toxin, injected into the masseter muscles, to mitigate the complications of the oro-lingual-facial dyskinesias. Agitation and catatonia are also common. Involvement of the psychiatry service may help. High doses of benzodiazepines can control agitation, insomnia, and catatonia. 31 Electroconvulsive therapy may alleviate catatonia. 31
Outcomes
Friends and family may assume that any patient with severe and long-lasting neurologic symptoms will almost certainly suffer significant permanent brain damage. Therefore, it is important to emphasize that the majority of NMDA-r encephalitis patients eventually do well. In a large case series (n = 100) at a median follow-up of 17 months, 75% either fully recovered or had only mild residual deficits with a mRS of 0 and/or returned to work. 6 However, recovery can take many months and usually requires prolonged physical and cognitive rehabilitation. Importantly, it should be noted 25% do not recover as well, and between 5 and 10% are dead within a year of diagnosis. 6 Recovery in that study was defined as having an mRS of 0, mild deficits, and/or if patients were able to return to their activities of daily living. 6 Cognitive dysfunction is also a common consequence of NMDA-r encephalitis, with one paper reporting eight of nine patients having persistent cognitive impairment up to 2–3 years after the illness. 14
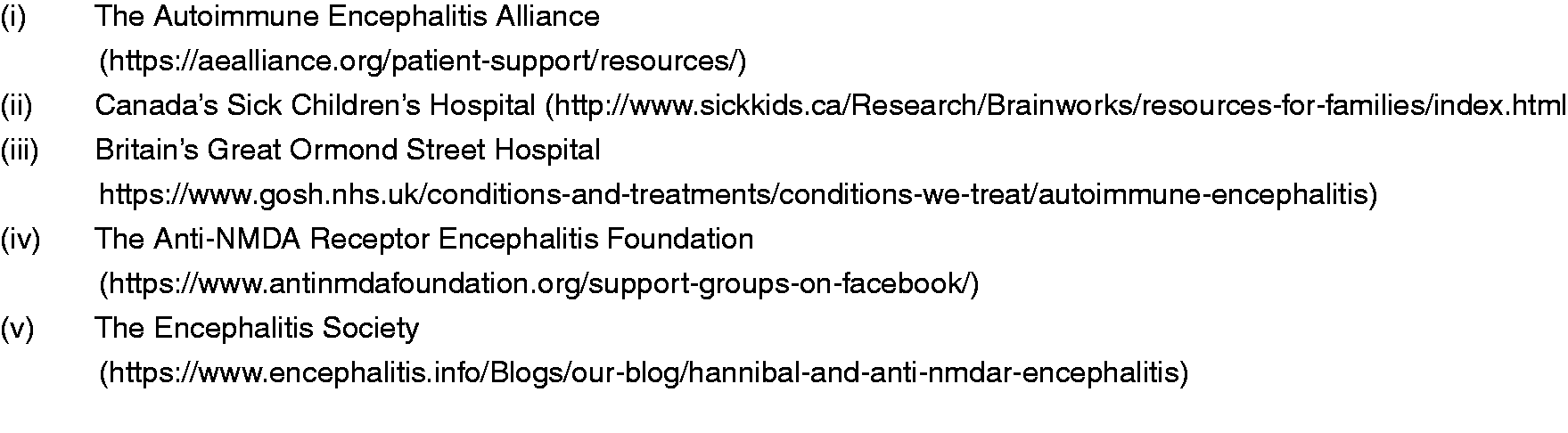
Given the patient’s typical young age and long inpatient battle, this disease can be especially distressing for both staff and families. Moreover, HCPs may not be accustomed to persisting with treatment in patients with severe neurological disease for as long as may be required in this disease. As such, we strongly encourage staff education about the prognosis coupled with an opportunity to debrief about their own feelings. We also recommend maximizing physiotherapy for patients and in-hospital family support. Families may also benefit from contact with support groups. Figure 4 summarizes five resources which may be of benefit to both families and HCPs seeking basic knowledge and support.
To date, there is insufficient data to conclude which factors are associated with neurological and overall functional outcomes after NMDA-r encephalitis. Generally, prognosis is worse if patients present with a low Glasgow Coma Scale score, if the diagnosis is delayed, if treatment is ineffective, if ICU care is prolonged, or if NMDA-r encephalitis is associated with other diseases.1,4,32,33 Balu and colleagues examined the probability of a poor functional outcome using a cutoff mRS score of 3 or more at one-year. Specifically, they identified the following independent predictors of poor outcome: the need for ICU admission, treatment delay greater than four weeks, lack of clinical improvement within four weeks, elevated CSF white blood cell count (>20 cells/µl), and an abnormal MRI. They assigned each of these variables one point to create the anti-NMDAR encephalitis One-Year Functional Status (NEOS) score, where a higher NEOS score was associated with greater probability of poor one-year functional outcome. 4
Another multicentre study of patients with autoimmune encephalitis necessitating ICU admission found that the need for mechanical ventilation, tracheostomy, the presence of a tumour, sepsis, or autonomic dysfunction were associated with poor neurological outcome. 33 Another study found that receiving immunotherapy early and a low CSF white blood cell count were associated with a good neurological outcome, defined as an mRS score of 0–2 at six months after ICU admission. 1
Importantly, even after recovery, patients need long term follow-up. This is because 20–25% of patients relapse from this condition. 6 After such an investment of time, resources, and empathy, it would be especially tragic to lose patients to follow-up. In summary, with a combination of knowledge, coordination, persistence, and attention, HCPs can significantly help patients and families suffering with NMDA-r encephalitis, and the likelihood of meaningful recovery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.