
Abstract
Background
Patients surviving critical illness are at risk of developing psychological symptoms that affect quality of life and recovery. Patient diaries may improve psychological outcomes by reducing gaps in memory and contextualising what has happened during admission. Factors including lack of guidelines, lack of awareness and time constraints may lead to poor diary use.
Aims
This quality improvement project aimed to increase diary provision and overall multidisciplinary team engagement with diaries for all patients admitted for over 72 h to an intensive care unit.
Methods
Trialled changes implemented via the ‘Plan-Do-Study-Act’ method included adding alerts to the online patient note system, providing education sessions and introducing a guidance document to facilitate entry completion.
Results
A ‘diary provision’ target of 100% was achieved (from a baseline of 26.1%). Simple changes have proven effective in establishing routine engagement with diaries, and lessons may be used to improve diary systems elsewhere.
Keywords
Introduction
The problem
Patient diaries kept during critical illness can improve patient outcomes and quality of life. They are routinely used in several National Health Service trusts, but their use is not standardised due to lack of national guidelines. Having considered their overall positive impact on patient experience, we felt it would be worthwhile to try and improve the patient diary system at Medway Maritime Hospital (MMH). Informal feedback from patients at the critical care rehabilitation clinic following discharge was overwhelmingly supportive of diaries.
This project was undertaken in a nine-bed intensive care unit (ICU) with 88 members of multidisciplinary team (MDT) staff providing care for approximately 600 patients per year. A patient diary system was established by nursing staff in 2012, but despite there being local diary guidelines, there were inconsistencies in diary provision and use.
Studies have shown a positive correlation between psychological sequelae and length of stay,1,2 especially in those who have been ventilated1,3 or sedated.2,4,5 On one occasion where MMH ICU was sampled, only one out of six mechanically ventilated patients had a diary. Furthermore, entries were being completed predominantly by relatives. Although relatives’ entries are helpful for patients and family, 6 entries written by staff can be targeted towards specific details which may later be perceived as distressing. They may also highlight milestones such as sitting out into a chair for the first time. In MMH, staff entries were written exclusively by nurses, but it is important to consider that diaries with entries from several contributors and disciplines may hold more meaning for patients.
Consequently, the primary SMART aim of the project was to provide all patients admitted to ICU for over 72 h with a diary (outcome 1). Secondly, we aimed for 90% of diaries to have entries written by at least three different MDT professionals (outcome 2).
Background
Patients surviving critical illness are at risk of developing psychological sequelae forming part of what is known as ‘post-ICU syndrome’, which can have substantial effects on quality of life and recovery. 7 It is estimated that 29% of patients discharged from ICU go on to develop symptoms of post-traumatic stress disorder (PTSD). 1 Evidence suggests patients also experience symptoms of anxiety and depression.8–11
National reviews such as ‘Critical to Success’ 12 and the Department of Health’s mandate ‘Comprehensive Critical Care’ 13 were the first to highlight the need for rehabilitation services. Current National Institute for Health and Care Excellence (NICE) guidelines for rehabilitation after critical care recommend commencement as soon as possible in order to prevent both physical and non-physical morbidity. 14 One of the emerging strategies to tackle this has been the use of patient diaries, which consist of a detailed narrative accounting one’s admission. Patients are able to read entries during recovery to piece together their stay. 15
During an admission to ICU, there are various cognitive, physical and emotional barriers to the formation of coherent and contextualised autobiographical memories including periods of amnesia, hallucinations, delusions, the impact of critical illnesses and treatment, pain and other forms of acute distress. If delusional memories are persistent and pervasive, there is a higher risk of developing psychological consequences of critical care, 16 and these factors should be addressed in order to tackle psychological sequelae.
The content of diaries can help the development of a coherent narrative where there are underlying fragmented trauma memories. 17 There is small-scale evidence from randomised controlled trials indicating reduced rates of psychological symptomatology in patient diary groups.9,18 However, patient diaries are not yet recommended by NICE, with a Cochrane report in 2014 stating there is insufficient evidence to support their use. 19 But as more large-scale studies are being conducted, more evidence is emerging. A recent meta-analysis has shown that diaries may reduce anxiety and depression while improving health-related quality of life. 20
Additionally, many studies describe encouraging effects on patient experience, with patients specifically stating they were helpful for recovery.15,21,22 They may also be beneficial for family members, by lessening learned helplessness and providing individuals with a role, 6 and there is evidence suggesting they reduce PTSD among relatives. 20
Furthermore, the ‘lack of evidence’ for diaries has not halted their use. Local guidelines have been developed as more evidence has emerged, and one is available for the Critical Care Network which includes MMH.23,24 Furthermore, formal intensive care follow-up is recommended by NICE, 14 and patient diaries are often an integral part of MDT follow-up clinics like the one run at MMH.
There is limited literature focusing on the improvement of patient diary systems. Pilot studies trialling and improving diary systems have focused on the effects on patient experience, but diary use has not been measured directly.15,25
Methods
Measurement
To establish baseline, we assessed the proportion of patients in ICU admitted for over 72 h who had been provided with a patient diary by directly surveying diaries on the unit on three distinct days at weekly intervals for 3 weeks. This resulted in a mean of 26.1%. All diaries sampled contained entries written by nurses only.
During cycle 1, we implemented a change to the online patient notes system (Metavision) that provided us with a continuous means of collecting data. Firstly, we generated an alert that triggered after 72 h of admission. Staff would be required to state if they had provided the patient with a diary before proceeding (yes or no). This provided a binary measure of diary provision. Members of the MDT would also see an alert when completing daily documentation asking if they had completed a diary entry; this would record a yes or no response. These binary data were extracted from the system at monthly intervals and cross-referenced with admission and length of stay data to calculate outcome 1, and with a staff list to calculate outcome 2.
To assess the validity of these measures, we directly sampled three diaries and cross-referenced them with outcome data. Statistical analysis was conducted using GraphPad Prism. Data were assumed to follow a normal distribution.
Primary outcome data were collected at 10-day intervals, and an average for each 10-day period was obtained. Given the slow ICU patient turnover and subsequent low number of individual entries per diary, secondary outcome data were presented as an average per cycle.
A staff survey was created, and 31 members of the MDT were asked to give opinions on diaries using a combination of Likert scales and free-text responses. Responses were used to determine process measures: the percentage of healthcare professionals aware of patient diaries and the stock availability of blank diaries. Balancing measures considered were staff perception of increased workload from completing diary entries and the added cost to the ward for providing greater numbers of diaries. Eleven members of nursing staff were re-surveyed after project completion to assess changes in these measures.
Design
We used the Plan-Do-Study-Act (PDSA) format adapted from the Institute of Healthcare Improvement.
26
We planned to make sustainable interventions by tailoring our efforts around survey answers and introducing changes that integrated easily into the normal working day. We also developed a cause and effect fishbone diagram in order to identify factors contributing to the problem
27
(Figure 1). This was considered in conjunction with staff survey results to determine which areas to target.
A fishbone diagram summarising the main reasons for poor staff engagement with patient diaries.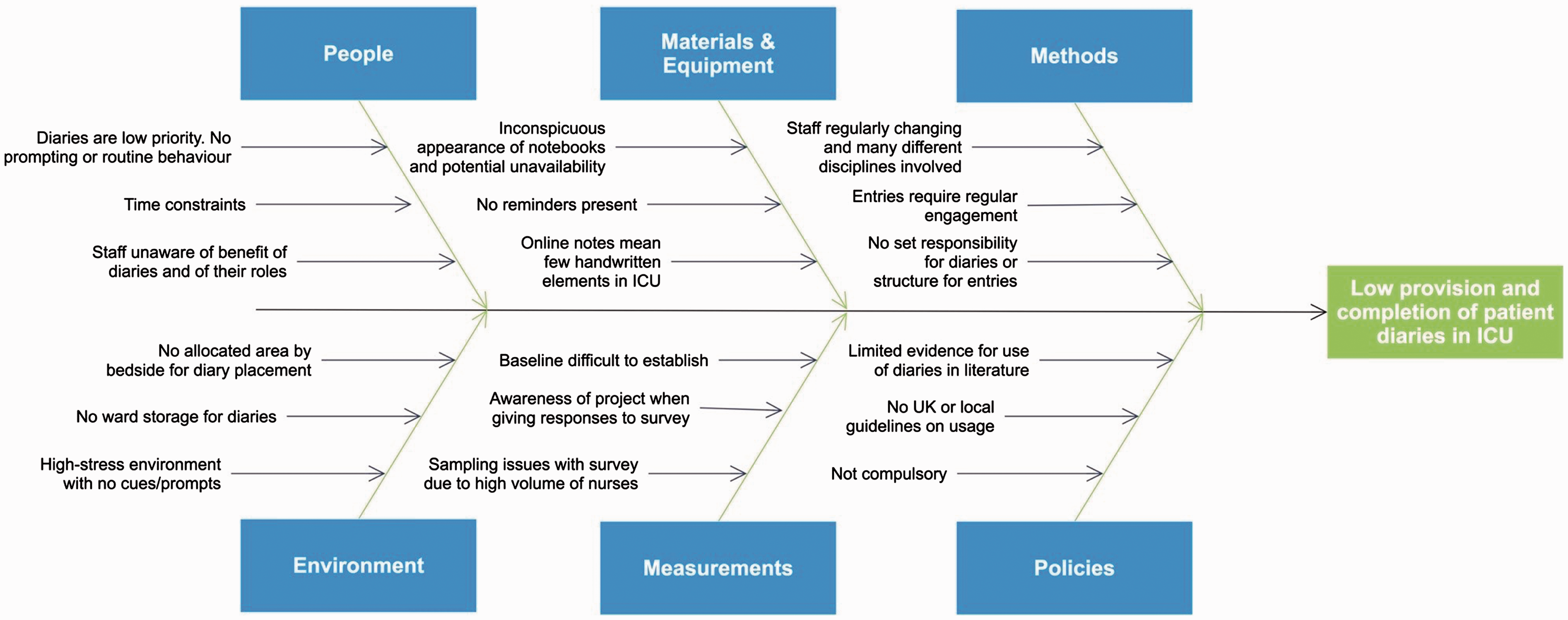
The project team consisted of two medical students in final stages of training, supervised by a senior physiotherapist and an ICU consultant who met monthly. We recruited the support of key stakeholders such as senior nurses already involved with diaries and education leads. The project ran over the course of 6 months, with a total of 53 MDT members participating.
The rationale behind focusing on patients admitted for over 72 h is that prolonged length of stay is recognised as being a risk factor for developing psychological sequelae.28,29 This identifies a patient group most likely to benefit from the diaries and avoids the application of a blanket intervention. 5
We aimed for the majority (90%) of diaries to have entries reflecting three different MDT professions once completed. We thought patients would benefit from having entries written by a range of healthcare professionals, as explaining their specialist work may provide broader insight and make diaries more beneficial to read during recovery.
Strategy
Results from the initial staff survey indicated that the non-compulsory nature, low priority and lack of routine use of the diaries were the main barriers to consistent provision and completion. Thus, PDSA cycle 1 introduced a visual alert for staff to start diaries and complete entries. We hoped that doing this on Metavision, which was used by staff daily, would be the most successful strategy.
We generated the Metavision changes described previously; the alert triggered after 72 h of admission which required a yes or no response regarding diary provision, and the compulsory checklist option asking if clinicians had completed a diary entry (recording a yes or no response). The latter was added to the nursing daily documentation checklist, and the physiotherapy, occupational therapy and doctor assessment pages.
PDSA cycle 2 concentrated on education within the MDT. Information briefings with a focus on the rationale behind diaries were delivered. Posters were put up around the ward, and senior staff, including the educational leads, disseminated information to colleagues.
PDSA cycle 3 involved the introduction of a second visual cue, given the success of this strategy during cycle 1. A laminated guidance document outlining the importance of diaries and instructions with an exemplar entry was produced. The information on this document was based on local guidelines. 23 These were placed on the nursing trolleys by each bedside, and an online version was uploaded to Metavision and emailed to staff.
Results
One hundred and twenty-nine patients were admitted to ICU during the course of the project (Figure 2). Seventy-one patients were admitted for over 72 h and 55 received diaries (77%). When calculating our secondary outcome, a further 10 diaries were excluded due to insufficient data. All qualifying patients admitted during the course of the project were accounted for. Mean length of stay was 7 days.
Flowchart accounting for all patients admitted to ICU during the course of the project.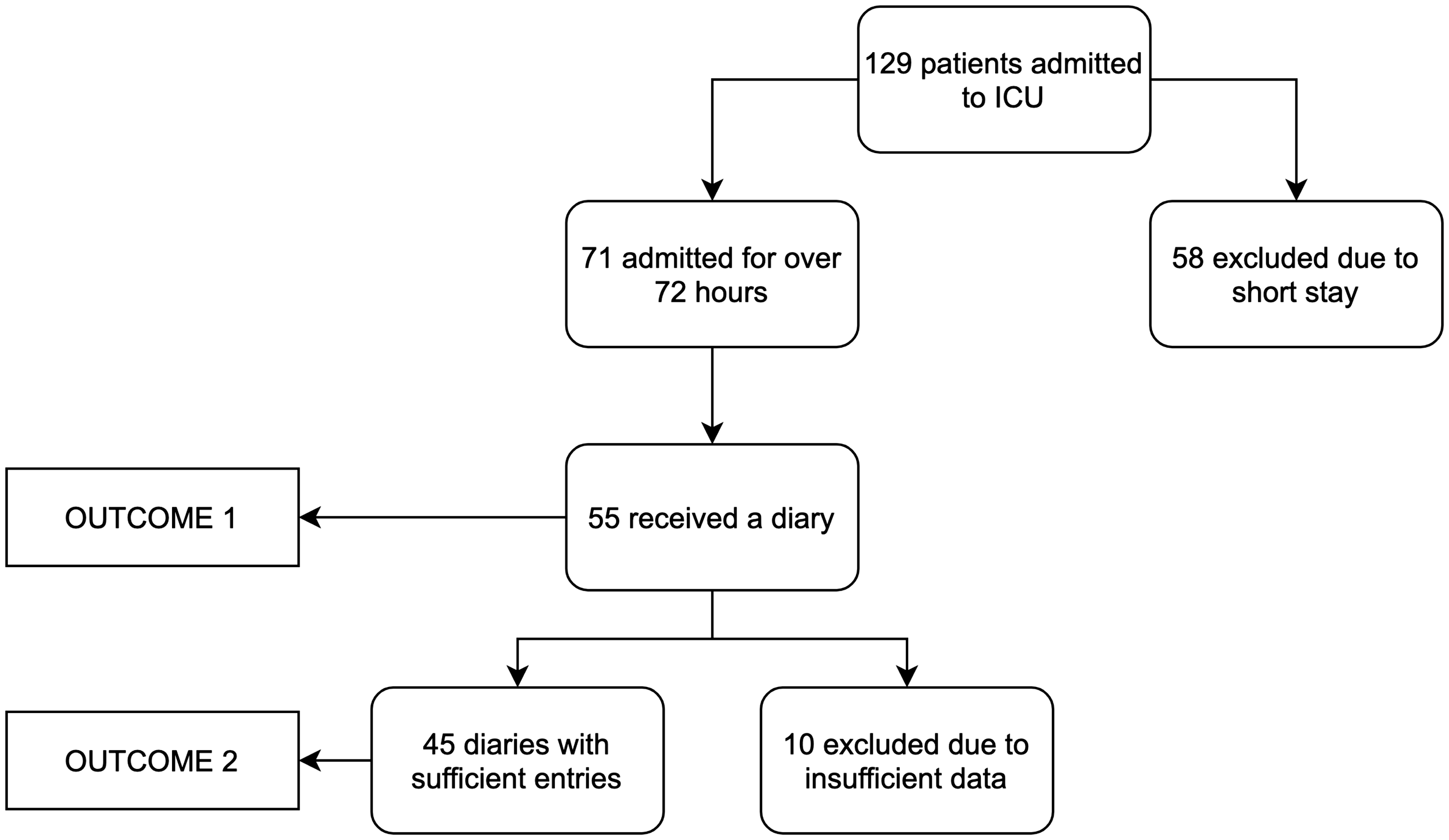
The results for our primary outcome, as displayed on the run chart, show a substantial improvement from baseline (Figure 3). Overall, the run chart illustrates a ‘shift’ above the baseline and ‘too few runs’ or crossings of the median line. These changes are consistent with non-random variation.
30
Run chart including baseline and all PDSA cycle data for outcome 1 (diary provision). The bottom line represents the mean for baseline data (26.1%); the top line represents our goal for this outcome (100%); the dashed line represents an interval when data were not collected. PDSA cycle data points represent 10-day intervals of data collection with the end date of each interval given as the ‘date of data collection'. Textboxes highlight implemented changes for each PDSA cycle. This run chart has two runs; the baseline is crossed only once, leaving a sequence of points below and one above.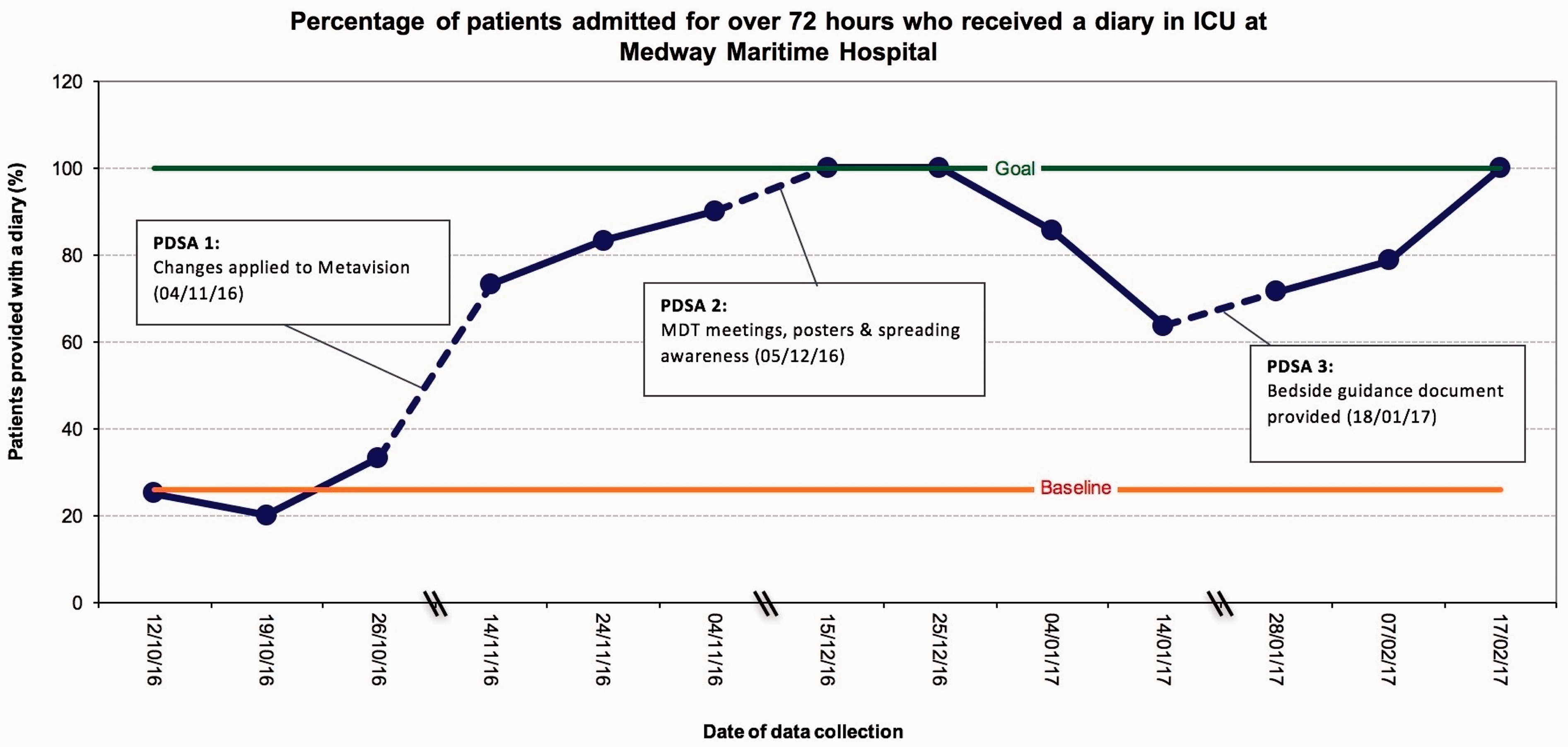
Diary provision increased steadily from baseline average (26.1%) to 90.0% after cycle 1, signifying that a simple reminder had a large impact. An unpaired-samples t-test was conducted to compare diary provision between baseline and PDSA cycle 1. There was a significant increase in provision during PDSA cycle 1 (M = 82.0, SD = 8.54) compared with baseline (M = 26.1, SD = 5.50) (t = 8.90, p = 0.0009).
Cycle 2 prompted a further increase to the 100% target, suggesting that education had reinforced initial changes. This was followed by a decrease to 63.6%. Given that this drop correlated with the holiday period, reasons such as reduced staffing levels and increased workload may account for this. It is also important to consider that education sessions may be effective in the short term but need to continue to sustain project successes. After the introduction of the bedside guidance document in cycle 3, diary provision steadily rose to 100% once more. However, it is difficult to interpret whether this increase is directly due to implementation of the document or whether provision was returning to previous standards once the holiday period had passed.
The secondary outcome was not met. In cycle 1, although no diaries met the criteria of having entries reflecting at least three different professions, 23.1% had entries written by two, which was still an improvement from baseline. During cycle 2, a single diary (4.8%) met criteria of three different professions and 47.6% met two, which was a further improvement. In cycle 3, however, no diaries met the criteria of three different professions, and this was a step back. Despite only one diary achieving the criteria of having entries written by at least three different professionals during the whole project, we saw an overall increase in physiotherapist and occupational therapist engagement. No doctors wrote entries.
Pre- and post-project surveys were used to evaluate process measures. The proportion of the MDT that were aware of the diaries increased from 93% to 100%, and nearly 50% of those completing the post-project survey experienced a situation where no blank diaries were available. This likely occurred secondary to the sudden increase in patients receiving diaries. This may have negatively impacted our results and needs to be addressed in future to ensure it does not continue to affect diary provision.
When considering balancing measures, we found that staff had a perception of increased workload. This was expected, given that they were being asked to complete diary entries on a more regular basis. The added cost to the ward for providing increased numbers of diaries was not quantified.
Discussion
When focusing on improvement within a clinical team, gaining the respect and enthusiasm of different members is crucial to promoting acceptance of change. However, with the introduction of any new initiative, there is frequently resistance, particularly if this involved increased workload. 31 Heavy workload has been shown to lead to poor communication and affect the time clinicians can allot to certain tasks. 32 For this reason, it is imperative that changes are simple, sustainable and they integrate well into routine. The changes introduced were successful in doing this, as illustrated by primary outcome data. By making the diary option on Metavision compulsory, we made sure staff addressed diary provision in their daily routine. Additionally, tailoring changes to staff opinions may improve sustainability.
It may be difficult for staff to engage when they are not directly seeing the benefits of interventions. We tackled this issue by educating staff on the evidence base behind diaries. We believe this led to the significant increase in diary provision as it was not a time-consuming task. In future, it may be useful to feedback accounts from follow-up clinic to staff. Positive feedback from patients and family members in follow-up services have been shown to enhance work satisfaction among nurses. 33 This is relevant as organisations with engaged staff result in better patient experience and care. 34
We were unable to engage any doctors. This may be a result of not directly targeting them as a group or due to pre-existing beliefs about patient diaries being a task for nurses, as they spend the most time with patients. It has become clearer why patient diaries are very much nurse-led, but we should continue to strive for a multidisciplinary approach.
A main limitation was the difficulty in establishing baseline data. As Metavision changes were not yet in place, diaries had to be directly sampled by a team member. In an attempt to account for this, baseline sampling was conducted on three separate occasions. However, data may not accurately reflect the true baseline and may lead to underestimation of provision. Collecting data over a longer period would provide a more reliable measurement.
The project had a relatively small sample size, both in the patient group studied and in the staff surveyed. We attribute this to slow patient turnover and shift patterns. These limitations could be overcome by running cycles for longer.
There is also the possibility of imprecision if staff incorrectly recorded a ‘yes’ response on Metavision without providing a diary or completing an entry. To analyse this, we sampled three diaries. Diary provision matched Metavision data, but there were some discrepancies in entries. We tried to minimise this by asking senior staff to provide support. Furthermore, staff may be biased to complete entries while the project is being undertaken.
We have recognised that trying to standardise such a personal intervention is difficult, and consideration must be given towards what is appropriate for each individual. On reflection, length of sedation and ventilation is more pertinent than overall length of stay. Furthermore, stricter inclusion criteria need to be in place, in order to highlight those who would benefit most from a diary, while reducing workload for staff. In future, tools such as CAM-ICU 35 to identify delirium may be useful to highlight high-risk patients. Appointing a clinical psychologist into the ICU MDT would allow for this to be assessed on a regular basis and may improve outcomes. 36
We appreciate that problems addressed in this project may not exist in other trusts. However, we believe our findings may be relevant for small ICUs setting up patient diary systems, or to those with established systems who may wish to improve them.
Conclusion
The literature suggests patient diaries can improve patient experience and outcomes, and their content can help make sense of underlying fragmented memories. This project has highlighted simple ways for diary systems to be improved and integrated into the ICU daily routine.
Overall, the primary aim was achieved during two cycles, and improvement was seen after each implementation of change. Data suggest minor changes such as computer system reminders combined with education are effective in establishing routine staff engagement with something that is poorly understood or used.
However, changes were difficult to maintain, and decreases in provision occurred after periods without education sessions, highlighting the need for continuous training and encouragement. Failure to achieve our secondary aim may be attributed to overly optimistic targets. Furthermore, improving a behaviour that is already practiced (nurses providing diaries to patients) is often easier than establishing new behaviours (MDT members writing in diaries when they were not previously doing so). Despite this, the project resulted in engagement of a wider variety and greater number of MDT members.
Since completion of the project, Metavision changes and diary guides have stayed in place. A ‘diary champion’ has been nominated to maintain improvements, and this has resulted in procurement of higher quality diaries. The next steps would be to re-evaluate whether improvements continue to be sustained, and to establish regular education sessions for the MDT. Using formal feedback from patients attending follow-up clinic in order to tailor diaries would also be useful. We hope to have implemented effective changes, working towards long-term sustainability, and that these changes are a small step towards improving patient experience and recovery in ICU.
Footnotes
Acknowledgements
We would like to thank the staff of Medway Maritime Hospital ICU for their support, time and commitment to this project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.