
Abstract
Introduction
Despite potential benefits, it is not known how widely physiotherapists use mechanical insufflation-exsufflation devices on UK adult intensive care units. This survey aimed to describe mechanical insufflation-exsufflation use in UK adult intensive care units.
Methods
Cross-sectional electronic survey of physiotherapists working in a permanent post on adult intensive care units.
Results
One hundred and sixty-six complete surveys were available for analysis, reflecting a diverse geographical spread. Nearly all (98%; 163/166) clinicians had access to mechanical insufflation-exsufflation. The estimated frequency of use varied, with the majority reporting weekly or monthly use (52/163, 32%; 50/163, 31%, respectively). Nearly all clinicians (99%) used mechanical insufflation-exsufflation with extubated patients. In contrast, around half of respondents (86/163, 53%) used mechanical insufflation-exsufflation with intubated patients, with a range of perceived barriers reported.
Conclusions
Mechanical insufflation-exsufflation devices are widely available on UK adult intensive care units, with use more common in extubated patients. Barriers to mechanical insufflation-exsufflation use in the intubated population warrant further investigation
Introduction
In the United Kingdom, approximately 230,000 adults are admitted to an intensive care unit (ICU) each year. 1 Around half require respiratory support (40–50%), commonly invasive ventilation (40.5%). 1 Although most adults successfully extubate in less than five days, some fail extubation. 2 Extubation failure is defined as reintubation within 48 h, with the incidence reported at between 10 and 40% of patients.2–5
Extubation failure is associated with increased ICU length of stay (LOS) and impaired quality of life. 6 Additionally, mortality is four times more likely in patients who require re-intubation. 7 Mechanical ventilation, although lifesaving, can cause significant problems for the patient; impaired psychological state (depression, anxiety), sleep deprivation, iatrogenic withdrawal and delirium, muscle weakness and infection. 8 Furthermore, the cost of an adult ICU NHS bed is around £2000/24 h; 9 therefore, increased LOS has significant cost implications. One cause of extubation failure is secretion retention, resulting from a patient's inability to cough effectively.5,8,10 An ‘Unmanageable secretion load’ was reported in 89% of patients requiring re-intubation, in comparison to only 39% of those who were successfully extubated. 11 Having an artificial airway in place impairs the patient's ability to cough and although secretions can be partially cleared by suctioning this will not clear the smaller airways.12,13
One device that can be used to aid secretion clearance is a mechanical insufflation-exsufflation (MI-E) device. MI-E is a non-invasive aid that delivers a deep inspiration (insufflation) followed immediately by a deep expiration (exsufflation) by applying positive and negative pressures. 14 The rapidly alternating positive and negative pressure aims to produce airflow in the airway approximating a normal cough. 14 There are a number of MI-E devices available for use within the UK. These MI-E devices can be applied via a facemask, a simple mouthpiece or via an endotracheal (ETT) or tracheostomy tube (TT). Despite emerging evidence relating to the positive use of MI-E in the ICU setting, we do not know the use of this device in the UK adult ICU. Thus, our aim was to describe the use of this device in practice across the UK.
Methods
A cross-sectional electronic survey (E-Survey) was undertaken in February 2018. The specific objectives were:
To quantify use of MI-E in adult ICU settings across the UK. To describe perceived enablers/barriers from physiotherapists to using the device. To explore ICU patient groups that physiotherapists feel are or are not appropriate for MI-E use.
Survey development
A 20-item survey was developed by ES in conjunction with researchers (FC and LT) and an independent physiotherapist (a UK based consultant Physiotherapist specializing in ventilation and airway clearance). The questions were closed-ended with space provided for free-text comments. The survey was piloted for face validity and clarity with two senior physiotherapists from UHBristol who had extensive working knowledge of MI-E in acute medicine. Minor amendments were made to the wording for clarity and the final survey input into Survey Monkey for distribution.
Sample
Inclusion criteria were qualified physiotherapists working in a permanent post on adult ICU in the UK. Exclusions were rotational physiotherapy staff, non-physiotherapists and non-adult ICU physiotherapists.
Data collection
The survey was distributed via the UK physiotherapist professional networks: the Association of Chartered Physiotherapists in Respiratory Care (ACPRC), Regional Intensive Care Networks and the Respiratory Leaders Physiotherapy Group. These groups were asked to forward the survey to clinicians meeting the inclusion criteria. E-mail reminders were sent at weekly intervals during the four weeks that the survey remained open. Ethical approval was granted by the University of the West of England (UWE) Research Ethics Committee (REC) Reference Number HAS.17.12.063. Participation was voluntary, and consent was implied by questionnaire completion.
Data analysis
Returned surveys were reviewed by ES to ensure respondents met the inclusion criteria. Only completed surveys were included for analysis. Data were downloaded into Microsoft Excel for analysis. Quantitative analysis was entirely descriptive, reflecting the aim of the survey. Data are presented as simple percentages and mean (SD) as appropriate. Free text responses were analysed by simple thematic analysis, using Burnard's framework 15 and are presented as themes.
Results
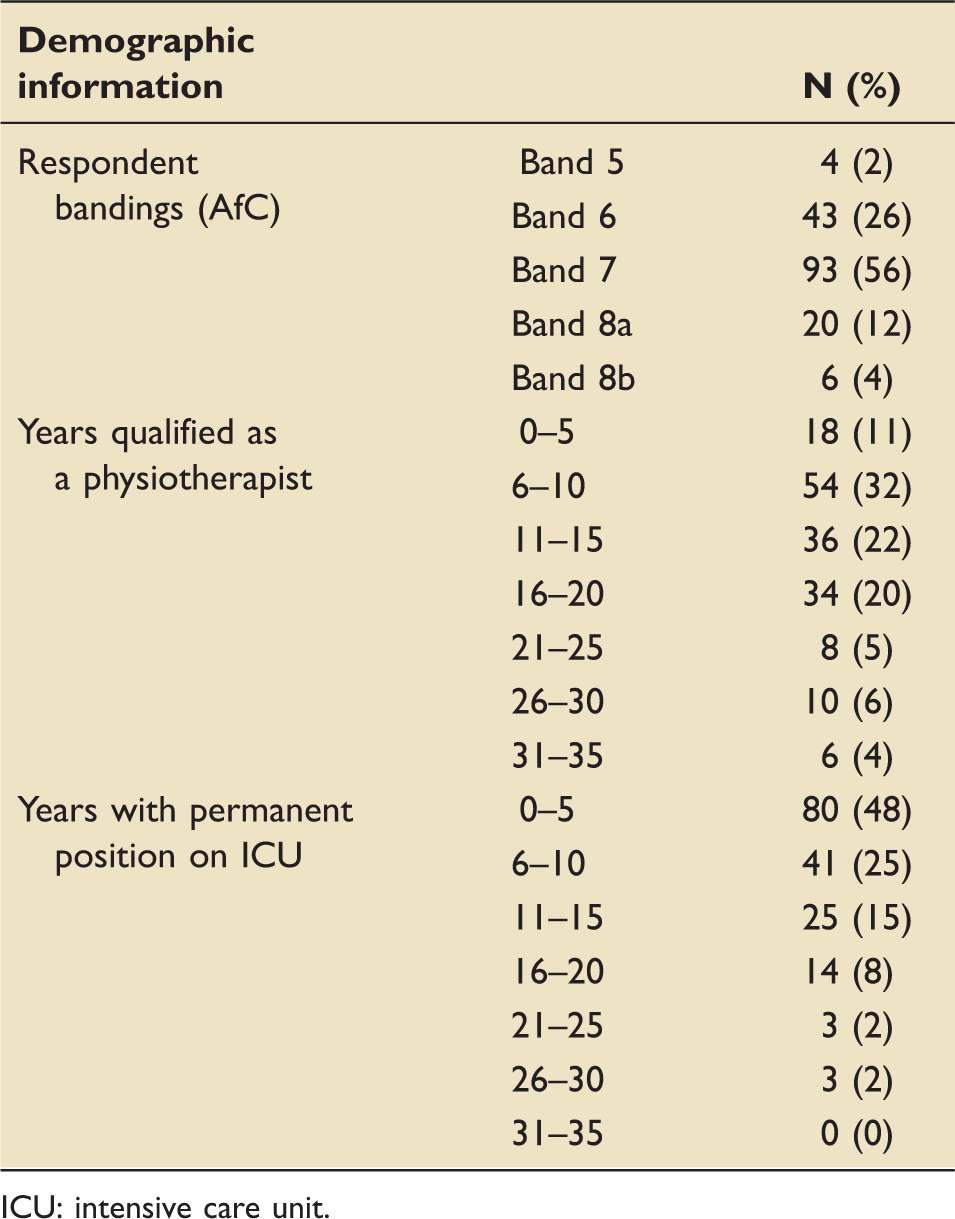
One hundred and sixty-six complete surveys were returned with diverse geographical representation (Figure 1) and including a mixture of Teaching Trusts and District General Hospitals. Due to the distribution method, and consequently unknown denominator, response rate could not be calculated. Over half (72%; 119/166) respondents were senior physiotherapists (Agenda for Change Band 7 and above) with a mean (±standard deviation) of 13 (±7) years since qualification and 8 (±6) years in a permanent role on an adult ICU (Table 1).
Geographical representation of survey respondents. Respondent demographic information. ICU: intensive care unit.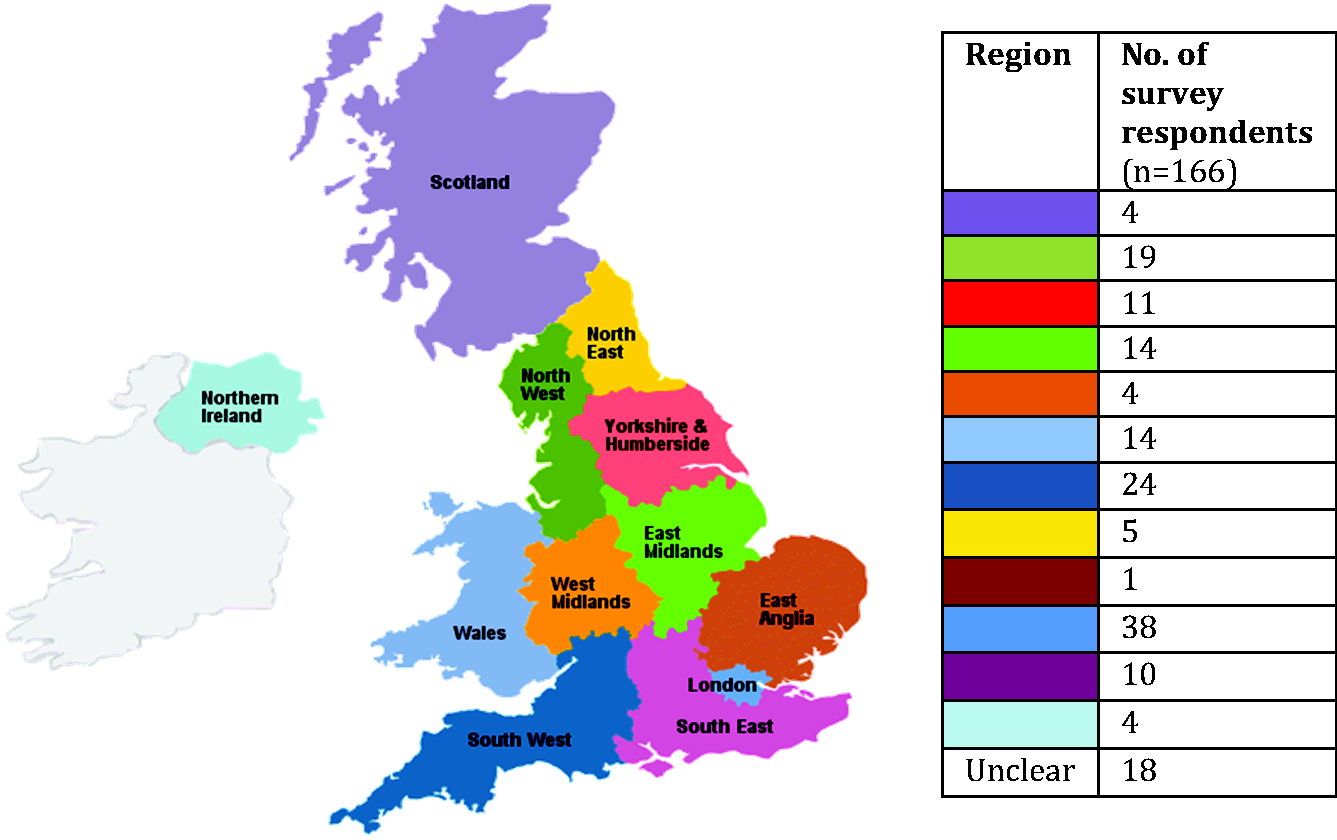
Nearly all (98% 163/166) clinicians had access to an MI-E device. Only three clinicians stated they did not have access to MI-E on ICU, reasons for this were identified as a ‘perceived lack of clinical need’ and ‘a lack of funding’. When asked if they would use MI-E if available, all stated ‘no’ to use in the intubated population, with mixed responses for use in an extubated population.
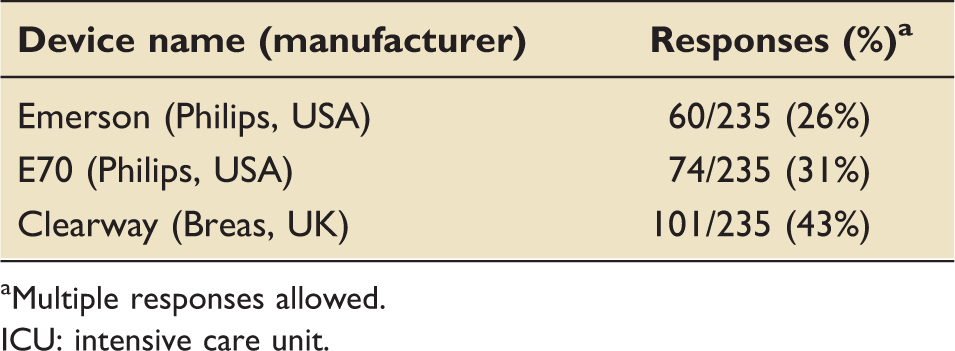
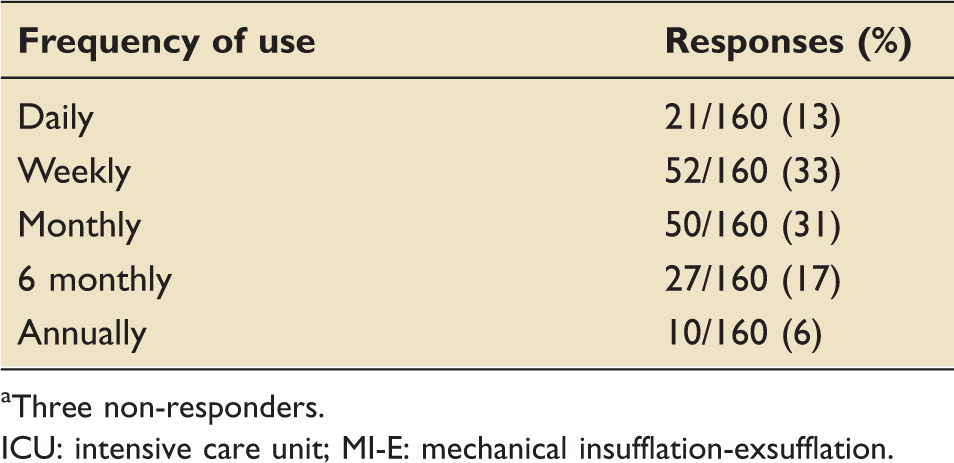
For those clinicians that had access to MI-E (n = 163), a range of devices were reported with the NIPPY Clearway (Breas, Stratford Upon Avon) being the most commonly available (Table 2). The frequency of use varied, with the majority of clinicians reporting weekly or monthly use (52/163, 32% and 50/163, 31% respectively) (Table 3). Just over half of respondents (n = 86/163, 53%) used the MI-E with intubated patients. In contrast, 99% of clinicians used the MI-E with extubated patients. Of those clinicians who did not use the MI-E in intubated patients (77/163, 47%), a range of perceived barriers was reported (Figure 2).
Barriers to MI-E use in the intubated population. MI-E: mechanical insufflation-exsufflation. Devices available on UK ICUs. Multiple responses allowed. ICU: intensive care unit. Estimated frequency of MI-E use in ICU by physiotherapists (in both intubated and extubated patients).
a
Three non-responders. ICU: intensive care unit; MI-E: mechanical insufflation-exsufflation.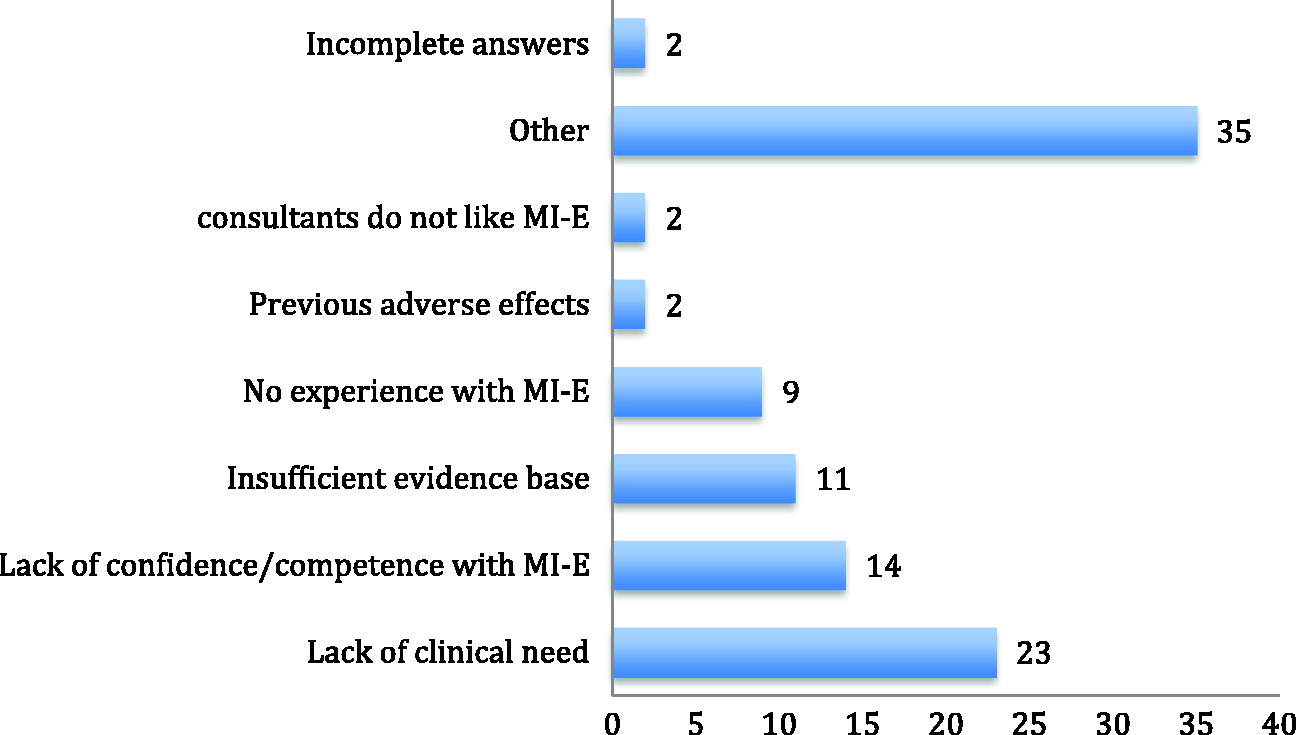
Perceived contraindications or precautions to use of the device were cited as: any contraindications to positive pressure use including high levels of positive end expiratory pressure (PEEP); undrained pneumothorax; cardiovascular instability and acute brain injury. Respondents stated they sought further opinion regarding MI-E use on thoracic and upper gastro-intestinal surgery patients and patients with lung cancer.
The majority of respondents (126/166) provided free text comments throughout the survey. Comments most frequently related to barriers to using MI-E in the intubated population. These were categorised into three main themes: (1) the need for training and experience using the device, (2) resource availability and (3) the culture of the ICU.
The need for training and experience using the device
Physiotherapists commonly referred to needing more training and experience, which was perceived as a barrier to MI-E use. In some cases it was clear that using MI-E in an intubated population was not a practice they had been exposed to before, “I have no experience in using a cough assist with intubated patients” (Band 7 physiotherapist). This was a common comment across bandings/seniority of clinicians. There was, however, a clear appetite to learn about MI-E in the intubated population. Comments included, “I would like to use it more-I have no experience using this in intubated patients” (Band 7 physiotherapist).
A lack of clarity regarding suitable patient application was also apparent, with frequent reference to patients with a tracheostomy. One senior physiotherapist stated “personally I haven't had the need or the patients suitable for it-I wait till they are trached.” Similarly other senior physiotherapists (Bands 8a and 7, respectively) reported “I have used it on patients via a trachy, but not intubated with an ET [endotracheal] tube” and “with regards to intubated patients I have used it mainly with trachy patients.”
ICU culture
A common theme related to how the culture of ICU could be a barrier to the use of the MI-E device. A number of physiotherapists described senior staff having a negative perception to MI-E use in the intubated population, limiting the use of MI-E by other more junior physiotherapists, with respondents stating; “seniors are very reluctant to use” (Band 6 Physiotherapist) and “Senior Physiotherapists are very reluctant to allow Band 7, 6 and 5 set up the device” (Band 6 Physiotherapist).
A number of respondents also referred to there not being a common culture for use of the device. In relation to MI-E use in the intubated population a physiotherapist (Band 6) stated “there's not really a culture of using it within critical care.” Another physiotherapist (Band 7) explained “I feel treatment is based on what has routinely been done and this is then passed onto all members of staff, making integration of new techniques difficult.”
There was often reference made to the differing opinions of using this device in the intubated population, “others in my team are bigger fans of these devices” (Band 7 physiotherapist).
Resource availability
The final theme related to how a lack of devices and finances to purchase more devices and associated consumables impacted on the ability to use MI-E. There was a common pattern that despite a unit having access to MI-E, the device was often borrowed from another clinical area “we would use MI-E more frequently but we don't have our own machines (bid currently in)” (Band 8a Physiotherapist CICU). For those units that did have their own device, it was then the quantity of devices that became the barrier to a wider implementation of the device. “We have one device only, so if use becomes widespread we would not have sufficient machines to make this functional” (Band 7 Physiotherapist).
There was also a situation where respondents wanted to use the device but were limited by finance “we are currently looking to secure funding for some devices to enable us to use them for intubated patients” (Band 7 Physiotherapist).
Discussion
MI-E has been examined as a treatment to facilitate extubation and prevent post extubation respiratory failure. Despite emerging evidence about the potential benefits and safety12,16,17 of this device in the intubated population, it is not known whether such findings are being translated into the clinical settings. This is the first survey of MI-E use across adult ICUs in the UK.
This survey has shown that the majority of physiotherapists have access to an MI-E device. Most physiotherapists used MI-E in the extubated population, whereas only around half used the device with intubated patients. A previous survey in Canada 18 did not specifically describe use in the intubated or extubated population. The use of MI-E as a secretion clearance technique to prevent intubation and re-intubation was found to be an indication for MI-E use, but routine use was infrequent (19% and 27% respectively). This use in the extubated population is lower than the current findings, where almost all of respondents used MI-E in the extubated population. Furthermore, Rose et al. 18 reported MI-E use during weaning from invasive ventilation in only 21% of respondents, and concluded this to be an infrequent indication for MI-E use. This is consistent with results from the current survey.
Analysis from the free-text responses further illustrated differences to use of MI-E via a TT or an endotracheal tube (ETT). Results from this survey highlighted that 53% of respondents (86/163) reported use of MI-E in the intubated population. What is not known from these results is whether respondents were referring to use with an ETT, a TT, or both. Free-text responses highlight the presence of an ETT (rather than a TT) to be a barrier to MI-E use in the intubated population. The evidence to date across both ICU and neuromuscular patients includes patients with both ETTs and TTs. Results from the current survey however suggest that only the findings related to the presence of a TT are being translated into the clinical setting. This is an interesting finding that requires further exploration.
A number of barriers to the use of MI-E in intubated patients were reported, often with conflicting views even within the same ICU. Commonly, the ‘culture’ of the ICU was cited as a barrier, and a negative perception by a senior physiotherapist would inhibit the use of the device. Similar findings have been reported previously with senior staff across multiple disciplines setting ICU culture and affecting implementation of all aspects of care. Previous studies examining the implementation of early rehabilitation or mobilisation on ICU concluded that ‘strong leadership’ was essential for success and sustainability of a new initiative or change of practice.19–21 Furthermore, Worral et al. 22 discussed how to improve uniformity in the delivery of lung protective ventilation across ICU. They highlighted challenges including ‘unit culture’, ‘authority hierarchy’ and ‘variation between multiple autonomous practitioners’ – all of which were concluded to impact the implementation of change. The diversity of opinion within clinical teams was evident in the current survey. Rose et al. 18 also found barriers to use where a lack of clinician knowledge and a lack of robust evidence to support wider implementation of MI-E, alongside other cough augmentation strategies. These barriers are consistent with our findings for MI-E use in intubated patients.
From both the current survey and previous work, 18 there is frequent reference to a ‘reduced evidence base’ by respondents as a barrier to the use of MI-E in the intubated population. However, there is increasing evidence of early benefits of MI-E in the intubated population to reduce reintubation. 12 An RCT of MI-E in mechanically ventilated was compared to standard care in 180-ventilated adults. 16 The MI-E group was superior for the primary outcomes of aspirated sputum weight (2.42 ± 2.32 g vs. 1.35 ± 1.56 g, P < 0.001), static lung compliance, airway resistance, work of breathing. However, no haemodynamic or ventilator complications were reported throughout the study.
Sanchez-Garcia et al. 17 also demonstrated preliminary data regarding the safety of using MI-E in intubated patients through a summary of case reports. Prior to this study, safety data were primarily based upon neuromuscular populations. Clinical parameters were measured before MI-E application, and at 5 and 60 min post intervention. They found no adverse effects including barotrauma, desaturations, atelectasis and hemoptysis. It should, however, be acknowledged that this study involved a small sample size of relatively stable patients, and no control group.
Results of our survey highlight that, despite the growing evidence for the device, barriers remain regarding the implementation and knowledge translation of these results into clinical practice. It is not clear whether clinicians are aware of this evidence or whether they believe that gaps remain in the evidence. Further in-depth exploration of the barriers to implementation of findings into the clinical setting is required including the apparent resistance to change. This reluctance to change is a common finding within healthcare professionals in general, and not specific to ICU or to physiotherapists 23 and the delay between research evidence incorporation into clinical practice is well known. 22 Exploring this is of paramount importance to understand the staff needs and when planning future educational activities in relation to the use of MI-E in the intubated population.
The most common reported frequency of use was weekly (33%), with monthly use the next most common (31%). Only 13% of respondents reported daily use of MI-E on ICU. Whether monthly, six monthly or annual use equates to a device being fully implemented into clinical practice, and whether such frequency enables clinicians to gain sufficient exposure and experience to maintain competence requires further consideration. Depending upon frequency of use other methods of device exposure such as simulated practice updates may be required to develop and maintain skills. Others have described more frequent device use, in intubated patients of at least once per day, 16 and in one study three times per day. 12 This finding highlights a gap between the evidence and its translation into the clinical setting. Despite the positive results from these studies,12,16,17 it should be questioned why clinicians are not following similar treatment protocols for the use of MI-E in an intubated population.
With regard to contraindications for the use of the device, participant responses were consistent with both manufacturer recommendations and the current evidence.12,16 Recent studies using MI-E in critically ill adults have excluded patients defined as having hemodynamic instability; neurologic instability; and the presence of an undrained pneumothorax. Findings from our study are consistent with those by Rose et al. 18
There are limitations to this survey that need to be acknowledged. Due to the distribution method, it was not possible to calculate a response rate for the survey. Some conflicting responses were reported from the same unit; however, this shows the variability of views between physiotherapists about this device. As with any survey self-report, responses may not reflect real practice. Despite these limitations, this survey has described current practice with the MI-E device within a wide geographical representation of UK adult ICUs.
Conclusions
MI-E is widely available on adult ICUs across the UK. Clinicians reported greater use with extubated patients in comparison to intubated patients. Barriers to the implementation of MI-E use in the intubated population are apparent. Understanding these potential barriers is important and warrants further exploration. Future research is required to understand the barriers could inform education and implementation techniques to enable effective and optimal use of this device in the wider ICU population.
Footnotes
Acknowledgements
Authors would like to thank the Association of Chartered Physiotherapists in Respiratory Care, The Respiratory Leaders Network, The Chartered Society of Physiotherapy and clinical colleagues for their assistance in sharing this survey during the recruitment period.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.