
Abstract
We evaluated whether non-invasive estimated inspiratory muscle pressure (Pmus) predicts extubation outcomes in ICU patients. Estimated Pmus, reflecting the pressure generated by respiratory muscles, was measured before and after the spontaneous breathing trial (SBT). Lower pre-SBT estimated Pmus (<4.1 cmH₂O) and post-SBT (<4.4 cmH₂O) were associated with extubation failure (AUC ≈ 0.73). P0.1 and dynamic transpulmonary pressure (PL,dyn) showed no significant association. Estimated Pmus offers a simple bedside method to assess inspiratory muscle strength and may help identify patients at risk of extubation failure. Further multicenter studies are needed to validate these findings.
Introduction
Extubation timing directly affects critically ill patients: premature extubation increases the risk of reintubation and related complications, whereas delayed extubation prolongs mechanical ventilation, increasing morbidity and ICU stay. 1 Respiratory muscle strength, reflected by the pressure generated during inspiration (Pmus), is a key determinant for weaning success. 2 Historically, measuring Pmus required invasive techniques, such as transdiaphragmatic pressure, which are complex and impractical for routine bedside use. 3 Bertoni et al. 4 proposed a non-invasive estimation method using airway occlusion maneuvers, providing a feasible tool to evaluate inspiratory muscle effort during ventilation.
We hypothesized that lower estimated Pmus values measured before and after the spontaneous breathing trial (SBT) could predict extubation failure, even in patients who initially tolerate the SBT.
Method
This prospective observational study was conducted from July 2022 to October 2023 in two mixed medical-surgical ICUs in Brazil. We included adult patients (>18 years) ventilated >24 h who passed a 30-min T-piece SBT and met clinical criteria for extubation. 5 Exclusion criteria included tracheostomy, accidental/self-extubation, and upper airway failure, as these do not reflect inspiratory muscle capacity. 6 Ventilatory data were collected immediately before and after SBT, including P0.1, estimated Pmus, and dynamic transpulmonary driving pressure (ΔPL,dyn). Estimated Pmus and ΔPL,dyn were calculated according to the method described by Bertoni et al., 4 which is based on the patient’s inspiratory effort against an occluded airway (ΔPocc). ΔPocc is the difference between PEEP and the minimum pressure reached during the inspiratory effort. Three expiratory airway occlusions were performed, each separated by at least three respiratory cycles, and maintained for the duration of a single breath. The mean value of the three ΔPocc measurements was used to estimate Pmus (Pmus = ¾ × ΔPocc) and to calculate ΔPL,dyn [ΔPL,dyn = (Peak airway pressure – PEEP) – (2/3 × ΔPocc)].
The primary outcome was extubation failure, defined as reintubation or use of non-invasive ventilation within 48 h post-extubation. 7 Statistical analysis included t-tests for continuous variables, Fisher’s exact test for categorical data, univariate logistic regression for significant predictors, and ROC curves to assess the predictive ability of estimated Pmus and identify optimal cutoffs.
Results
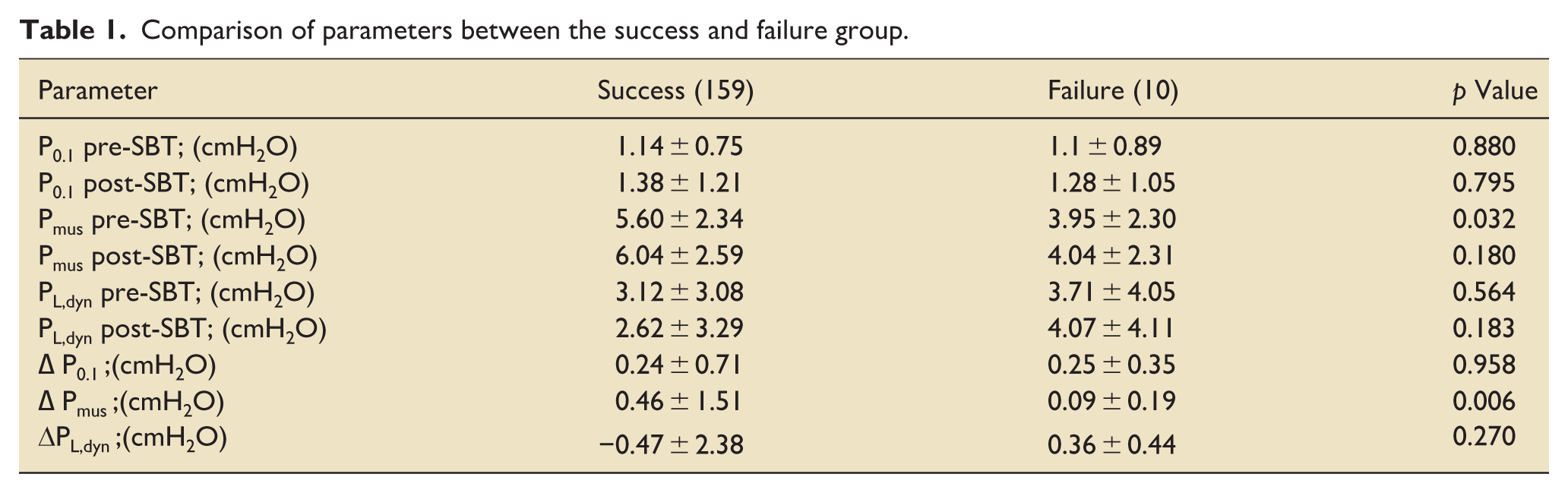
Out of 413 patients screened, 169 were included; 159 (94.1%) had successful extubation, while 10 (5.9%) failed (Supplemental Figure 1). Baseline demographics were similar between groups, with no significant differences in age, sex, APACHE II scores, or ICU length of stay (Supplemental Table 1). The success group had higher estimated Pmus before SBT (5.6 ± 2.3 cmH₂O) compared to the failure group (4.0 ± 2.3 cmH₂O; p = 0.032) and a greater increase after SBT (ΔPmus: 0.46 ± 1.51 vs 0.09 ± 0.19; p = 0.006; Table 1).
Comparison of parameters between the success and failure group.
ROC analysis showed an AUC of 0.727 for pre-SBT estimated Pmus and 0.737 for post-SBT values (Figure 1). Cutoffs identified were <4.1 cmH₂O pre-SBT and <4.4 cmH₂O post-SBT, predicting failure with reasonable sensitivity and specificity. P0.1 and ΔPL,dyn were not associated with extubation outcomes.
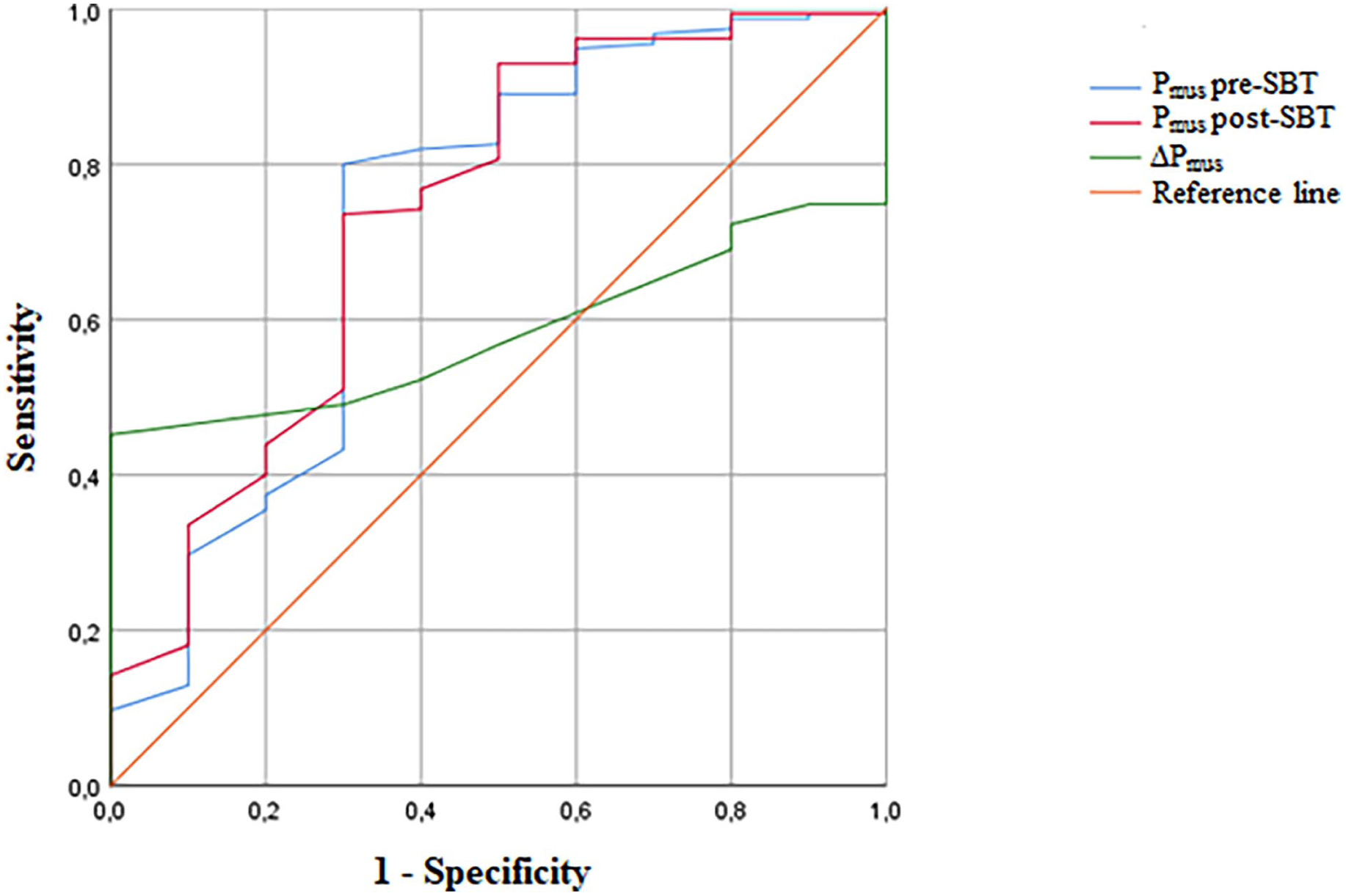
ROC curves of estimated Pmus pre-SBT (blue line), AUC = 0.727 (95% CI, 0.534–0.919); estimated Pmus post-SBT (red line), AUC = 0.737 (95% CI, 0.557–0.917); estimated Δpmus (green line), AUC = 0.584 (95% CI, 0.490–0.677).
Discussion
This study demonstrates that lower estimated Pmus values, even among patients who tolerate SBT, are associated with higher risk of extubation failure, likely due to underlying diaphragmatic weakness. 3 Estimated Pmus offers a direct, non-invasive measure of inspiratory muscle effort, contrasting with P0.1, which reflects respiratory drive and may not correlate with muscle strength. 8 While AUC values indicate moderate predictive power, our findings suggest estimated Pmus could complement existing weaning indices, like RSBI, to enhance clinical decision-making. 9
The method’s practicality makes it attractive: Pmus estimation requires only standard ventilator functions and simple maneuvers, potentially allowing widespread implementation. Six patients in our cohort had high estimated Pmus (>10 cmH₂O), indicative of excessive effort, yet were successfully extubated, underscoring the complexity of balancing adequate effort without overexertion. Conversely, patients with lower Pmus may fail due to insufficient strength to sustain spontaneous breathing.
Limitations include the observational design, single-center setting, and small number of failure events, which limit statistical power. Moreover, while upper airway failure cases were excluded, other non-muscular causes of failure could confound results. Larger multicenter studies are needed to validate cutoff thresholds and explore integration with multimodal weaning assessments.
Estimated Pmus measured non-invasively before and after SBT shows promise as a predictor of extubation failure in ICU patients, with cutoffs <4.1–4.4 cmH₂O indicating higher risk. Integrating this simple bedside parameter into routine practice could aid in identifying patients at risk, but further multicenter validation is essential.
Supplemental Material
sj-docx-2-inc-10.1177_17511437251377989 – Supplemental material for Lower non-invasive estimated Pmus predicts extubation failure in mechanically ventilated ICU patients
Supplemental material, sj-docx-2-inc-10.1177_17511437251377989 for Lower non-invasive estimated Pmus predicts extubation failure in mechanically ventilated ICU patients by Graziela Müller, Manoela Bonato Zocoli, Jéssica Magnante, Geovana Teo Zamprogna, Silvano Altair do Nascimento, Gustavo Bruno Rático, Ewan C. Goligher and Antuani Rafael Baptistella in Journal of the Intensive Care Society
Supplemental Material
sj-tif-1-inc-10.1177_17511437251377989 – Supplemental material for Lower non-invasive estimated Pmus predicts extubation failure in mechanically ventilated ICU patients
Supplemental material, sj-tif-1-inc-10.1177_17511437251377989 for Lower non-invasive estimated Pmus predicts extubation failure in mechanically ventilated ICU patients by Graziela Müller, Manoela Bonato Zocoli, Jéssica Magnante, Geovana Teo Zamprogna, Silvano Altair do Nascimento, Gustavo Bruno Rático, Ewan C. Goligher and Antuani Rafael Baptistella in Journal of the Intensive Care Society
Footnotes
Acknowledgements
Thanks to the patients and professionals of the ICU of the Hospital Universitário Santa Terezinha.
Ethical Considerations
The study was approved by the ethics committee of our institution on July 26, 2022 (UNOESC/HUST Ethic Committee, protocol number: 5.545.989).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.