
Abstract
Background
Medical–legal partnerships integrate lawyers into health care to identify and address legal problems that can create and perpetuate disparities in health for patients and their families. They have previously been utilised for patients who are at high-risk of being disadvantaged such as the elderly, the disabled and those affected by chronic diseases. We have used a partnership to address the legal needs of patients with acute, critical illness including major trauma.
Method
In 2007, a free, comprehensive legal advice service was established at University Hospital Southampton NHS Foundation Trust. The service is bound by strict guidelines which have been endorsed by NHS England. The legal service is specifically prevented from acting against the NHS. A retrospective analysis of the service over a period of 11 years was undertaken to look at the range of legal advice sought. Where a potential compensation claim against a third party was identified, the percentage of cases where the legal service was instructed was noted and the outcome for those cases was examined in further detail.
Results
Five hundred and fifty-one patients and or their families have been referred to the legal service. Of these, 343 had sustained major trauma. Over 2300 hours of free legal advice were provided on non-compensation issues, primarily related to welfare benefits, local authority assistance, obtaining power of attorney or seeking Deputyship from the Court of Protection and claims against existing insurance policies. Two hundred and seventy-five of the 551 patients (50%) were found to have a potential compensation claim against a third party. The legal service was instructed to pursue a claim in 82 cases. Interim payments of nearly £13 million were provided and £128 million of compensation has been awarded in 51 cases that have been settled.
Discussion
Medical–legal partnerships are well-established in the USA. We have demonstrated that in UK, there is a demand for early legal advice for patients who have sustained critical illness including major trauma. More data are required to identify the rehabilitation outcomes for patients who have received legal support. A similar medical–legal partnership should be considered at every acute NHS Trust.
Keywords
Introduction
In January 2018, NHS-England published the NHS Standard Contract 2017/18 and 2018/19. 1 In this, there was a specific endorsement of the valuable legal service provided to patients and their families in major trauma centres (MTCs). Currently, 11 of the 27 MTCs in England have a legal support service in place, and a further 10 centres have such services in various stages of development (Prof Chris Moran, National Director of Major Trauma, personal communication). Similar services are also in place at a number of specialist rehabilitation centres. Patients admitted acutely to hospital have often made little, if any, arrangements regarding their personal affairs. Their families may find difficulties in dealing with financial and legal matters while the patient is seriously ill, particularly those in ICU when the patient often lacks capacity. In 2012, the Government introduced the Legal Aid, Sentencing and Punishment of Offenders Act 2012 which restricts legal aid in particular for cases involving family law, clinical negligence, employment and immigration law, debt and housing and welfare benefits. 2 As a result of these cuts to legal aid, patients and their families can struggle to secure legal representation.3,4 Within hospitals, there is often limited facility to obtain legal advice; Patient Advisory Liaison Services or Citizen Advice Bureaus may be available but these may be unable to provide advice on specific legal issues or in a timely manner. Early identification and resolution of financial and legal issues may help to relieve the anxieties experienced by patients and their families. Many seriously ill patients also experience delays in access to rehabilitation or problems arranging suitable accommodation that can result in inappropriate acute bed occupancy.5–7 Access to legal advice may help with the early identification of funding sources which can enable patients to access earlier or increased amounts of rehabilitation. These funding sources, such as an interim payment from a compensation claim or a payment under a personal insurance policy, may facilitate appropriate discharge.
There are a number of models for a legal service established at NHS Trusts in England. An individual legal firm provides the service at some centres, including the service at University Hospital Southampton (UHS). A consortium of legal firms is contracted to a single centre at some Trusts, and a case management firm is contracted by others. UHS was the first acute NHS Trust to develop a free and comprehensive legal service for critically ill patients and their families. We have previously reported the preliminary results of this service over the first two years following commencement in the Neurosciences Intensive Care Unit. 8 This paper reviews the experience from 11 years of operation including further details regarding patients reported in the earlier paper.
Methods
UHS NHS Foundation Trust is accredited as one of 12 major trauma centres for the care of both adults and children in England. UHS is also the regional centre for neurosciences and cardiovascular disease. The Wessex trauma network that it serves covers an adult population of around 3.5 million and receives paediatric cases from neighbouring networks to the east and west. Each year, UHS receives around 50,000 emergency admissions with around 800 patients having major trauma (injury severity score > 15). The legal service was introduced at UHS NHS Foundation Trust in January 2007. This followed the first such service which had been initiated at a national spinal rehabilitation centre. Permission was granted for a six-month pilot scheme following discussions between the Trust's legal advisors and the clinicians and managers of the neurosciences directorate. The scheme was approved by the Trust's ethics committee. The service commenced for patients in the Neurosciences Intensive Care Unit and subsequently expanded to cover patients on the General ICU, Paediatric ICU and for patients sustaining major trauma following the establishment of UHS as a major trauma centre in 2012. The key principles supporting the development are summarised in Appendix 1. Importantly, the legal service gives free advice on a full range of legal issues. If the legal service identifies a potential claim for compensation, they provide a list of approved firms that can undertake such work and will not accept instructions on the first meeting with the patient or their family. Funding from compensation claims, in which the legal service is subsequently instructed, supports the pro-bono component of the service. There are no financial inducements to either the host NHS Trust or to health care professionals to make referrals to the legal service. Independent legal advice was that a tendering process was not required as the Trust derived no financial benefits from the service. A formal, rolling contract between the host Trust and the legal service has subsequently been established.
Patients or their relatives are provided with an information leaflet regarding services available within the hospital that includes information on the free legal services available. A signed request to see the legal service is obtained from the patient or their family and recorded in a ward diary. The legal team are not provided with any of the patient's medical records but simply the name of the person requesting the meeting. The legal service provides a weekly clinic to meet with patients or their families although urgent legal advice is available by telephone at any time. Each meeting is conducted by a partner (senior solicitor) from the legal service. The NHS Trust legal service is the responsibility of a named partner in the legal firm who has overall responsibility for the non-compensation cases. The non-compensation work is done by paralegals under the supervision of the Head of Pro Bono work who is an Associate Solicitor. The legal service keeps a record of the issues addressed with each client, and a monthly record is provided to the NHS Trust.
Non-compensation advice
Powers of attorney and court of protection
The legal service can provide advice on the patient's property and affairs whilst they are in hospital. They can advise on mental capacity and, in the event that the patient lacks the mental capacity to manage their property and affairs, the process of applying to the Office of the Public Guardian to appoint a Deputy. If the patient has capacity, the legal service can advise on Ordinary and Lasting Powers of Attorney and can assist with executing a power of attorney.
Financial issues Outgoings
Patients may have direct debits and regular payments which need to be paid such as mortgage repayments. The legal service can write to the various organisations concerned to inform them of the patient's situation. This is sent with an accompanying ‘To whom it may concern’ letter from the clinical team outlining the patient's admission to hospital. The legal team can request a hold or cancellation of the direct debits and assist the patient with reinstating these at a later date. Patients may have incurred debts which they will be unable to repay following their injury. In these circumstances, the legal service contact the creditors and request a hold on the patient's account so that no further interest is accrued on the debt until the patient's prognosis is better known and the patient is able to arrange repayment. They can also assist where patients are no longer able to go on holidays which have been booked. They can write to holiday providers and/or travel insurance companies to outline the patient's circumstances.
Once the patient's long-term prognosis is established, they can assist the patient or their families to calculate their disposable income by using an income and expenditure calculation or in having debts written-off entirely.
Insurance policies
The legal service advises patients and their families to check all insurance policies to establish whether they have no-fault or critical illness cover which may provide for payment in the event of injury or illness. The legal service can assist with reviewing any policies and making claims under them if cover is available. A number of patients have insurance policies which provide cover for ‘Personal Accident’ or ‘Total Permanent Disablement’ and also ‘Hospitalisation Benefit’. The legal service assists patients in completing claim forms and will liaise with insurers on their behalf. In some circumstances, insurance providers can refuse to provide payment because the patient's injuries do not meet their policy criteria. In this situation, the legal service can write to the insurance company setting out the extent of the patient's injuries and resulting difficulties in order to demonstrate that they do in fact meet the criteria. In some instances, the insurance company may maintain that the patient does not fit their criteria, and the legal service can assist patients to make a complaint to the Financial Ombudsman Service.
Care
The legal service can advise on the duties of the NHS and the local authority to provide care post discharge from hospital for patients who have sustained serious injury.
Employment
Often an informal and personal approach is usually best initially as employers can be reluctant to engage with solicitors. The legal service can provide general advice from the Employment department to help to inform patients. The legal service can advise on employment schemes such as Access to Work and Specialist Employability Support. These schemes are run by Jobcentre Plus who will put applicants in touch with a Disability Employment Advisor. The legal service can also advise on the patient's sick pay entitlement and their rights under the Equality Act.
Housing
Patients are sometimes unable to return to their property because it is inaccessible to them. The legal service provides advice on re-housing and the local authority's duty to provide minor adaptations. They also advise patients on the availability of Disabled Facilities Grant (DFGs). DFGs provide funding towards the cost of providing essential adaptations to give a disabled person better freedom of movement into and around their home and access to essential facilities within their home. DFGs are means-tested, and an application form must be completed. The legal service can assist with DFG applications and liaise with the local housing department on the patient's behalf.
Welfare benefits
The legal service can advise on patient's benefits entitlement following a serious injury. They can also advise on becoming an Appointee, which is a mechanism that enables family members to claim benefits on behalf of the patient if they are unable to do so themselves. The legal service can provide patients and their families with an overview of the benefits they may be entitled to and explain the necessary criteria for each such as means-testing. In circumstances where patients have had their benefits revoked or reduced, they can review the patient's documentation and can advise on the prospects of submitting an appeal. If required, they can assist with that appeal.
Transport
The legal service can advise on the motability scheme and the procedure to be followed to obtain a blue badge.
Compensation claims
If a potential compensation claim is identified, the legal service is contracted to provide the patient or their family with a list of legal firms and their contact details that could provide assistance. This list comprises firms of solicitors approved by Headway (the brain injury charity) and the Spinal Injuries Association. The in-house legal service will not accept instruction to act on behalf of a patient on the first meeting with a patient or their family. The host Trust is provided with a list of cases where a potential compensation claim is identified and whether the in-house legal service was instructed.
Cases involving serious injury may take several years to conclude. Compensation claims are often only settled when experts are able to give a final opinion and prognosis of the Claimant. Only then can the Claimant be certain to recover all of the costs to which they are entitled. Final settlements will often comprise an initial lump sum and annual periodical payments depending on the life-expectancy of the claimant. The law recognises that a claimant may need access to some of their compensation at an early stage, and if a potential compensation claim is identified, it may be possible to obtain an interim payment from the insurance company of the Defendant. Such payments are a payment on account of the subsequent final settlement. Receipt of an interim payment can potentially reduce or even stop a Claimant's entitlement to welfare benefits after one year of receiving the first interim payment. Advice is therefore offered regarding the establishment of a Personal Injury Trust into which any interim payments can be placed. Such Trusts prevent interim payments from affecting Claimant's benefits
Results
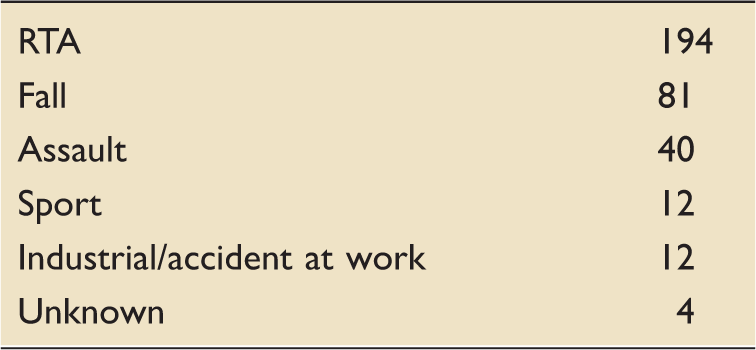
Aetiology of traumatic mechanism.
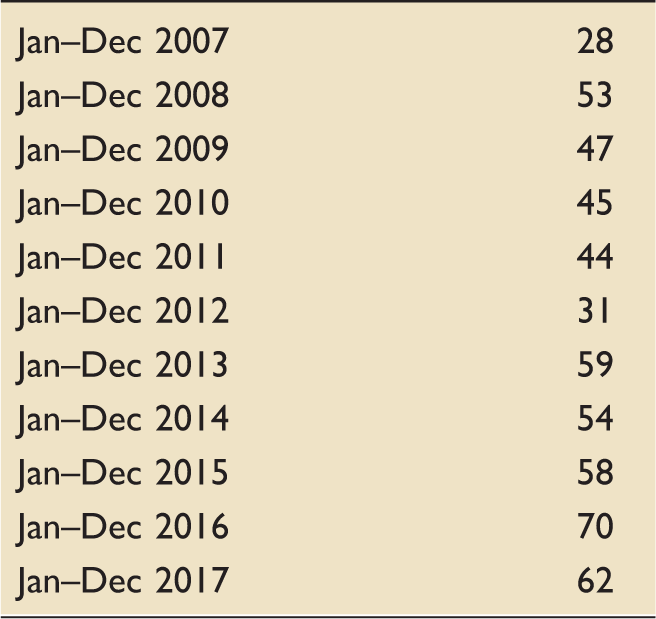
Number of appointments year on year.
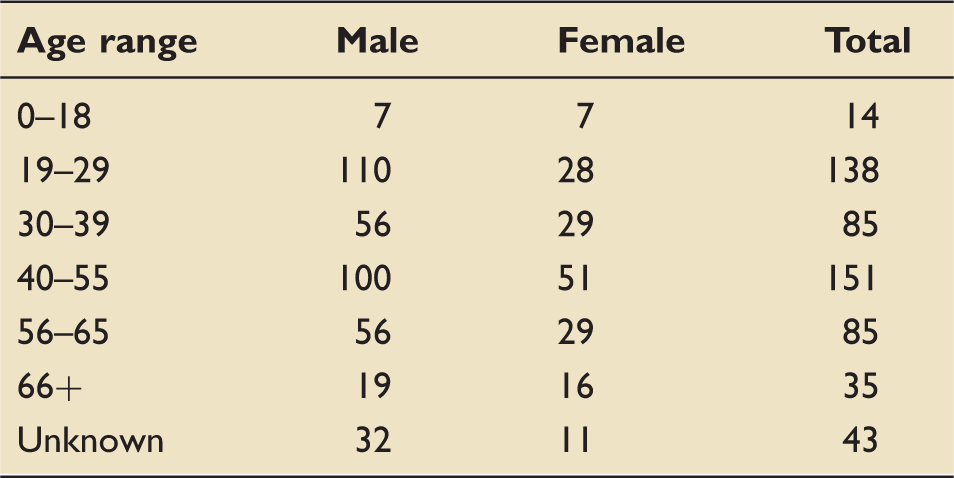
Age range of patients referred to the legal service.
Non-compensation advice
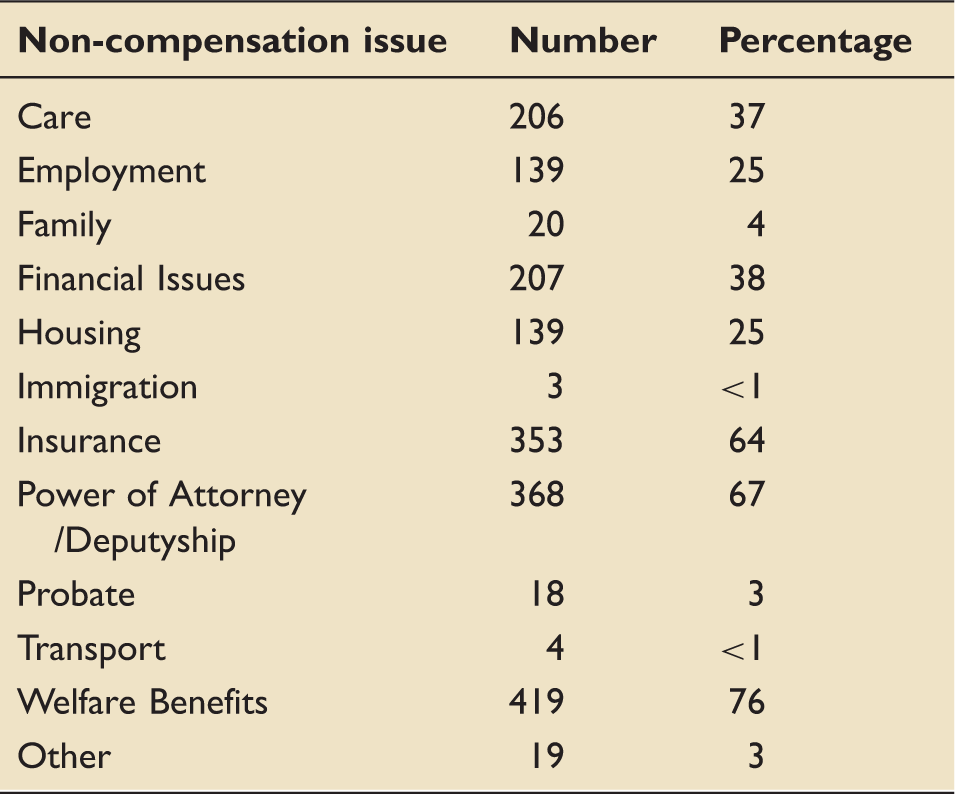
Number and nature of non-compensation work.
Compensation advice
Two hundred and seventy-five of the 551 patients (50%) were considered to have a potential compensation claim against a third party. In 82/275 (30%) of cases, the law firm providing the legal service was subsequently instructed to pursue a claim and further data is available.
Interim payments
Patients and their families have received in total over £12.9 million in interim payments pending final settlements. The period between instruction of the legal service and the provision of an interim payment ranged from 3 to 55 weeks. Interim payments varied in value between £5000 and £1.125 million.
Full settlement
Of the 82 potential claims, 51 have been settled, 22 are ongoing, 8 were discontinued and 1 claim was lost at trial. Of the settled claims, a total of over £128 million has been awarded in compensation. This comprises £65 million in lump sum awards and £63 million in annual payments. The lowest settlement was £7500 and the highest in excess of £15 million (comprising of a lump sum and periodical payments).
Importantly, none of these settlements have been as the result of a claim against the NHS. In one case, a potential clinical negligence claim against the host Trust was identified. The legal service declared a conflict of interest and advised the patient to discuss concerns regarding their treatment with their medical team. The patient and their family were provided with free advice on the non-compensation issues including employment, existing insurance policies, welfare benefits and family issues. The patient subsequently instructed another firm of solicitors and settlement was reached.
Discussion
Medical–legal partnerships are well established in other countries. In 1993, a medical–legal partnership model was developed between the Department of Paediatrics at Boston Medical Center and the Boston University School of Medicine. 9 It was intended to help parents negotiate the complex systems that contribute to improving children's health such as adequate housing, nutrition, education and safety. Studies in the USA have shown that households with low incomes have between one and three unmet civil legal needs related to their income, housing, employment or family issues such as guardianship of domestic violence. 10 In UK, the Low Commission surveyed over 1000 GPs in October 2014. The survey findings included that 88% of those questioned believed that patients being unable to access legal or specialist advice about their problems would have a negative impact on their health. 11 In 2006, a National Centre for Medical–Legal Partnership was established in the Department of Health Policy and Management at the Milken Institute School of Public Health at the George Washington University. There are now over 290 health clinics and hospitals in the USA that partner with legal-aid agencies, pro-bono legal firms and law schools in 41 states (http://medical-legalpartnership.org/). The first hospital–legal partnership in Canada was established at The Hospital for Sick Children in Toronto in 2009. 12
Although the model originated in paediatrics in the USA, it has expanded to include other populations who are at high-risk of being disadvantaged such as the elderly, the disabled and those affected by chronic diseases.13–15 For many vulnerable patients, accessing legal services can be challenging, and many do not recognise that their problems have legal solutions. 9 Within the geriatric population, clinicians considered that at least half their patients had issues of capacity and competency to make medical decisions. Patients were also considered to be affected by issues related to benefits, health insurance, housing, utilities, estate planning, employment or immigration. 13 By addressing complex social issues such as housing, employment, income and benefits, legal advocacy can directly benefit patients. These benefits include reduced costs of medical care, less general stress, increased access to preventative healthcare and improved well-being. 16 Partnerships have also been able to improve the wider health care system as healthcare professionals have a unique access to vulnerable individuals and by early identification of legal issues can direct them to appropriate support thus helping to avoid crises. Medical–legal partnerships have also been able to support the introduction or amendment of laws to help vulnerable populations.
We independently established a free legal service for patients in Southampton in 2006. This was recognised in the National review of the MTC in Southampton conducted in 2014. Southampton University Hospitals has implemented free legal services for patients including major trauma patients which the panel commend as
The most commonly sought advice in our patient group was regarding entitlement to welfare benefits, applications for deputyship in the case of loss of competence to manage affairs, personal insurance claims, financial issues and care funding. All of the advice has been pro-bono and occurred whilst the patients have been admitted for their episode of acute care. Legal aid has been significantly cut over recent years. Having to seek and pay for such advice would we feel provide an additional burden for patients and their families at a time of acute distress. A report by the Citizen's Advice Bureau estimates that for every £1 of Legal Aid cost, there are potential savings of £2.34 for housing advice, £2.98 on debt advice, £8.80 on benefits advice and £7.13 on employment advice. 21 Provision of free legal advice on NHS premises is also likely to have a similarly large impact on government funding.
Nearly half of all patients referred to the legal service were considered to have a potential claim against a third party. This figure is likely to reflect the demographic of patients admitted to the particular areas covered by the service at UHS. Of these, a third of patients instructed the legal firm providing the service. This figure has been roughly consistent throughout the period that the legal service has been in place. The remaining 70% of patients either did not pursue a claim or instructed an alternative provider of legal services. Patients who are involved in a compensation claim have been reported to have a worse recovery than those who are not involved in a claim. 22 This may be due to an unconscious, financial incentive for patients not to get better as long as the settlement process is ongoing, or an indication that the compensation process itself is a cause of stress. Financial and recovery concerns have been shown to be associated with worse pain and poorer physical and psychological outcomes following major trauma. 23 Early financial support may help alleviate the psychological distress following road traffic accidents and in doing so reduce the ultimate costs of a claim. 24 The provision of almost £13 million pounds of interim payments is clearly important in providing financial reassurance to seriously injured patients and their families, allowing them to make decisions regarding a range of care and housing matters.
This review of the legal service has a number of limitations. Clearly, UHS receives a large number of patients each year who were not referred or who declined access to the legal service. This is likely in part to the lack of knowledge of health care professionals regarding the legal service. It is recognised that knowledge among healthcare providers as to when and how to contact legal resources can be lacking. 25 In addition, the range of issues and constantly changing legislation make it difficult for doctors and other NHS staff to provide suitable advice and support. Use of an I-HELP screening assessment when obtaining the social history is recommended in many programmes in the USA. 13 Even in those aware of the legal service, there have been concerns expressed regarding the appropriateness of referring patients and their families to an outside service. We believe that this service fulfils one of the core principles of the NHS identified by Professor the Lord Darzi of Denham, namely working across organisational boundaries and in partnership with other organisations in the interest of patients, local communities and the wider population. 26 It is hoped that with the recent endorsement of NHS England, we can continue to educate healthcare professionals regarding the benefits of such a service.
The review provides very limited outcome data for patients who did access the legal service beyond details regarding compensation issues. We are currently seeking to follow up all patients referred to the legal service to establish their outcomes using standard quality of life questionnaires. It may then be possible to compare these with a cohort who were not referred or declined the legal service. Ideally, we would wish to see a legal service in all acute NHS Trusts in England. There remains a need for clarity regarding the best model for the legal service and which groups of patients might similarly benefit. Ultimately we would seek the formation of a UK Centre for Medical–Legal partnerships similar to that in the USA. Such a centre could independently advise Trusts and legal firms regarding the introduction of legal services, establish practices for identifying and addressing the full range of legal needs for patients and could work to improve the social and environmental factors that affect health.
Supplemental Material
Supplemental Material1 - Supplemental material for Medical–legal partnerships: 11 years' experience of providing acute legal advice for critically ill patients and their families
Supplemental material, Supplemental Material1 for Medical–legal partnerships: 11 years' experience of providing acute legal advice for critically ill patients and their families by C. Andrew Eynon, Lucy J. Robinson and Kara M. Smith in Journal of the Intensive Care Society
Supplemental Material
Supplemental Material2 - Supplemental material for Medical–legal partnerships: 11 years' experience of providing acute legal advice for critically ill patients and their families
Supplemental material, Supplemental Material2 for Medical–legal partnerships: 11 years' experience of providing acute legal advice for critically ill patients and their families by C. Andrew Eynon, Lucy J. Robinson and Kara M. Smith in Journal of the Intensive Care Society
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Eynon has advised NHS England and other NHS Trusts regarding the development of medical–legal partnerships. He has received funding from Stewarts Law LLP for providing advice regarding the development of legal aid services within the NHS. He has been instructed by Stewarts Law LLP and other legal firms to provide medicolegal advice and has received honoraria from Stewarts Law LLP and other legal firms for educational seminars. He was also on the editorial board for JICS until 2018. Ms Robinson is a partner at Stewarts Law LLP. Ms Smith is a senior associate at Stewarts Law LLP.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.