
Abstract
Critically ill military trauma patients have been found to have a high incidence of psychological morbidity following their Intensive Care Unit (ICU) experience, including recall of significant auditory and visual hallucinations. It follows that this may be attributable to delirium, which has not been previously described in a young, previously fit population following trauma. The case-notes of 85 male patients (mean age 26 years), admitted to a single UK ICU following military trauma, were retrospectively assessed for delirium using DSM-IV criteria. Of the 993 ICU days assessed, 13.4% were delirium-positive, with just over half of patients (51.8%) experiencing at least one day of delirium. On delirium-positive days, 69.2% received a documented intervention, with the majority of interventions (66.4%) being pharmacological, commonly with a sedative or anti-psychotic. Presence of delirium was significantly associated with severity of injury, assessed by Injury Severity Score (OR 1.037, 95% CI 1.003–1.072, p = 0.031). Duration of ICU stay was significantly increased, from 4 to 8 days (p < 0.005), as was the duration of mechanical ventilation (for the 84.7% of patients who were ventilated) from 7 to 13 days (p < 0.005). Delirium is common in military trauma patients, despite their young age and premorbid fitness. A review of longer-term psychological outcomes should be considered.
Introduction
Following traumatic injury on overseas deployment, critically ill UK military patients are aeromedically evacuated to the Intensive Care Unit (ICU) of the Royal Centre for Defence Medicine (RCDM), Queen Elizabeth Hospital Birmingham. Following discharge, many attend the Defence Medical Rehabilitation Centre (DMRC) at Headley Court. 1
A review at the DMRC ICU follow-up clinic highlighted a high incidence of psychological morbidity. 2 Whilst formal psychiatric diagnoses were beyond the scope of the clinic, the review did assess patients’ recall of symptoms. One of the most notable findings was that 48% of patients recalled having significant and distressing hallucinations during their ICU admission. Patient descriptions included; ‘I lived a permanent nightmare’, ‘the worst days of my life’ and ‘worse than getting my legs blown off’. It follows that these symptoms may be attributable to delirium.
There has been rising interest in critical care delirium as its association with poorer outcomes is increasingly recognised. The risk factors for developing delirium on the ICU are described by the PRE-DELIRIC model: age, disease severity scoring (APACHE-II), admission group, coma, infection, metabolic acidosis, use of sedatives and morphine, urea concentration, and urgency of admission. 3 Many of these risk factors, with the exception of age, are relevant to a military ICU population. Prospective studies have found the incidence of delirium in the general ICU population to be 20–80%. 4 However, critically ill military patients represent a unique population that has not been previously described with respect to their experience of delirium.
To our knowledge, there are no reported data looking at ICU delirium in either military patients or young trauma patients. However, psychological disturbance amongst ill military patients is a long recognised phenomenon. Early nineteenth century military physicians described a change in mental state amongst injured servicemen and suggested that this could be linked to alcohol withdrawal. 5 Recently, there have been a number of small descriptive studies suggesting an increased incidence of delirium on emergence from general anaesthesia amongst serving and veteran military patients.6,7 This is an interesting observation for what it suggests about the inherent predisposition of the military patient’s susceptibility to delirium. In the authors’ clinical experience, medical staff have frequently observed episodes of agitation and confusion amongst military ICU patients.
The aim of this study was to identify the incidence of delirium in this unique patient population.
Methodology
With permission from DMRC, we accessed the data from 119 patients who had been involved in a trial ICU follow-up clinic. The clinic assessed the patients’ ICU experience and subsequent symptoms by interview and patient questionnaire. We identified 96 of the patients involved. The majority were distinguished by recorded unique identifiers: service numbers (72) and Joint Theatre Trauma Registry (JTTR) reference numbers (7). A minority were identified by cross-referencing age, date of injury and Injury Severity Score (ISS) with the JTTR (14). The remaining 23 could not be identified with confidence and were excluded. The complete intensive care case notes were available for 85 of the 96 patients identified. The intensive care episodes for these patients ranged from 3 December 2008 to 2 February 2013, during which 325 military patients were admitted to the ICU. Figure 1 is a consort flow diagram illustrating patient inclusion.
Patient numbers included and excluded from study population. Overall, 85 patients were included in the study. ISS, NISS and APACHE II scores not available for every patient which was taken into account in later analyses.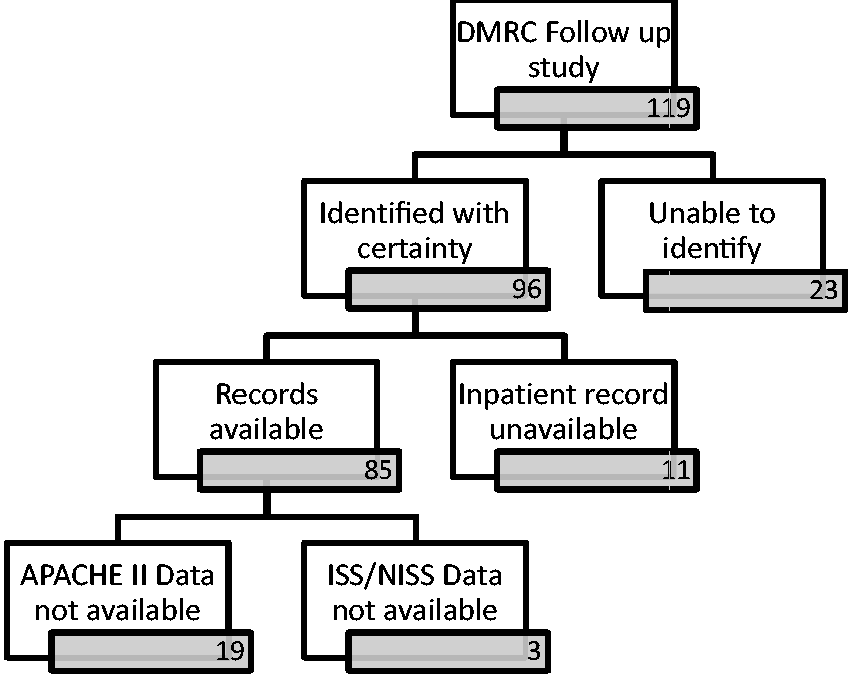
Expert advice was sought on the retrospective assessment of case notes and ICU charts for evidence of delirium. An assessment proforma was developed, utilising DSM-IV criteria
8
which defines delirium as follows:
Disturbance of consciousness (i.e. reduced clarity of awareness of the environment) with reduced ability to focus, sustain or shift attention. A change of cognition (such as memory deficit, disorientation, language disturbance) or the development of a perceptual disturbance that is not better accounted for by a preceding, established or evolving dementia. The disturbance develops over a short period of time (usually hours to days) and tends to fluctuate over the course of the day. There is evidence from the history, physical examination or laboratory findings that the disturbance is caused by the direct physiological consequences of a general medical condition.
An ICU day was defined as starting at 0800 and finishing at 0800 the following calendar day, to coincide with the 24-h time period covered on each ICU chart. Each ICU day for each patient was assessed. Note was made of mechanical ventilation status, the highest and lowest Sedation Scores of the day (which changed to Richmond Agitation Sedation Scores after change in local policy at the mid-point of our data collection period), whether there had been a planned sedation hold, whether any formal screening for delirium had been documented and whether the patient had attended for an operation. Documentation was then assessed for acute onset or fluctuating symptoms of delirium. These include confusion, mental status change, inattention, disorientation, hallucinations, agitation or inappropriate behaviour. Evidence was recorded verbatim. An episode had to demonstrate both disturbance in consciousness and change in cognition for the ICU day to be documented as delirium-positive. This method of retrospective case note review of delirium has since been validated. 9 If the day was delirium-positive, the subsequent management and interventions were noted.
The ISS, New Injury Severity Scores (NISS) and APACHE II scores were recorded for each patient, where available. ISS is calculated by summing the squares of the Abbreviated Injury Scores of the three most injured body areas, whilst NISS is a modification accounting for multiple injuries in the same body area. A higher score indicates a higher severity of trauma and is predicative of survival. 10 APACHE II is a measure of acute physiological instability and predicts outcome. 11 Due to data unavailability, ISS and NISS were not available for three patients and APACHE II scores were not available for 19 patients. The duration of mechanical ventilation was calculated from admission to the UK ICU. The majority of patients were aeromedically evacuated to the UK by day 1 following injury; however, there was some variability, so duration of mechanical ventilation prior to arrival in the UK was also considered.
Case notes were reviewed over the period July to October 2014. Each assessing clinician received training on using the proforma and recognising delirium. The first 14 patients, totalling 76 ICU days, were assessed independently by multiple clinicians, blinded to the others’ assessments. Inter-rater reliability was reviewed using the Krippendorf alpha statistic using a freely available online utility. 12 Subsequently, a single clinician assessed independently, with group discussion and consensus to resolve equivocal assessments.
Statistical analysis was carried out using IBM SPSS Statistics for Windows, version 20.0. Independent Mann–Whitney U test was used to determine significance, as data did not follow a normal distribution after assessment with Kolmogorov–Smirnov and Shapiro–Wilks tests. We considered p ≤ 0.05 as the level of significance.
Local clinical governance approval and military approval was granted. As a retrospective analysis of routine clinical data, ethical approval was not sought.
Results
Inter-rater reliability
The Krippendorf α statistic in the pilot population of 14 patients was 0.8821, with percentage agreement of 97.4%, demonstrating good inter-rater reliability.
Study sample
Comparison of factors amongst patients who did and who did not experience delirium.
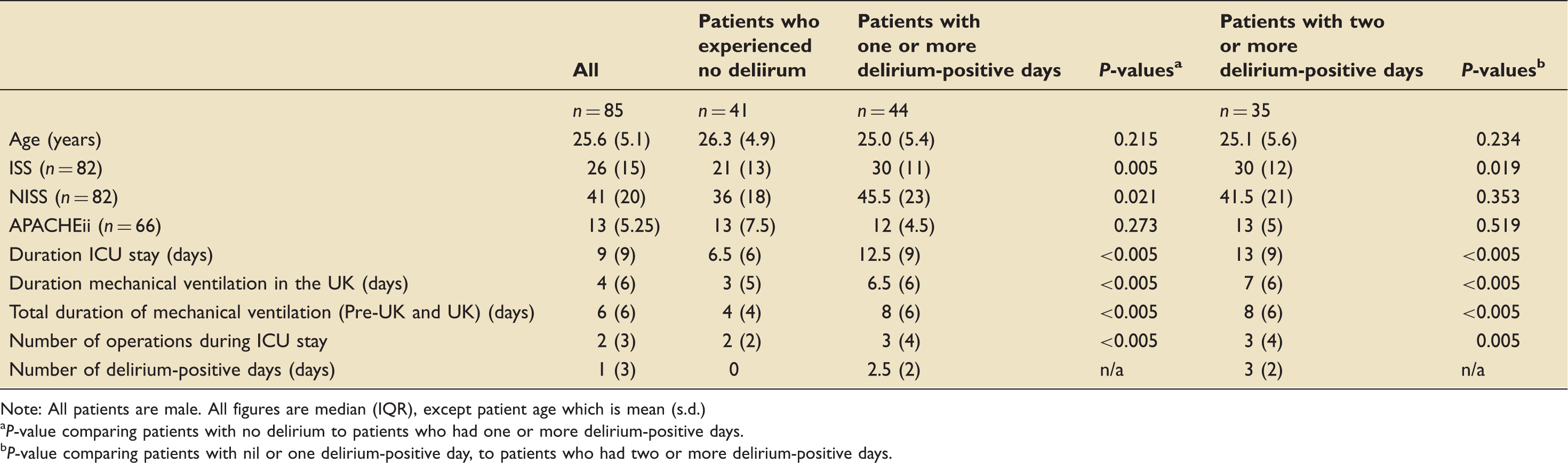
Note: All patients are male. All figures are median (IQR), except patient age which is mean (s.d.)
P-value comparing patients with no delirium to patients who had one or more delirium-positive days.
P-value comparing patients with nil or one delirium-positive day, to patients who had two or more delirium-positive days.
Incidence of delirium
In total, 993 ICU days were assessed, in which 133 (13.4%) were delirium-positive. Of the 85 patients, 44 (51.8%) experienced at least one day of ICU delirium on retrospective assessment. Of these, 35 patients (79.5%) experienced more than one day of delirium. The median number of delirium-positive days per patient was one day (IQR 3, range 0–8).
Presence of delirium was significantly associated with severity of injury. ISS of greater than 20 was associated with an incidence of delirium of 61.8%, compared to an incidence of 29.6% when the ISS was 20 or less. An NISS threshold of 30 gave similar results. Univariate analysis shows that both ISS (OR 1.077, 95% CI 1.022–1.135, p = 0.005) and NISS (OR 1.037, 95% CI 1.003–1.072, p = 0.021) are significantly associated with development of delirium. All patients with an ISS greater than 40 developed delirium. Figure 2 illustrates the incidence of delirium with increasing ISS. Where the data were available for the APACHE II scores, there was no link with the incidence of delirium.
Histogram showing the incidence of delirium with increasing ISS.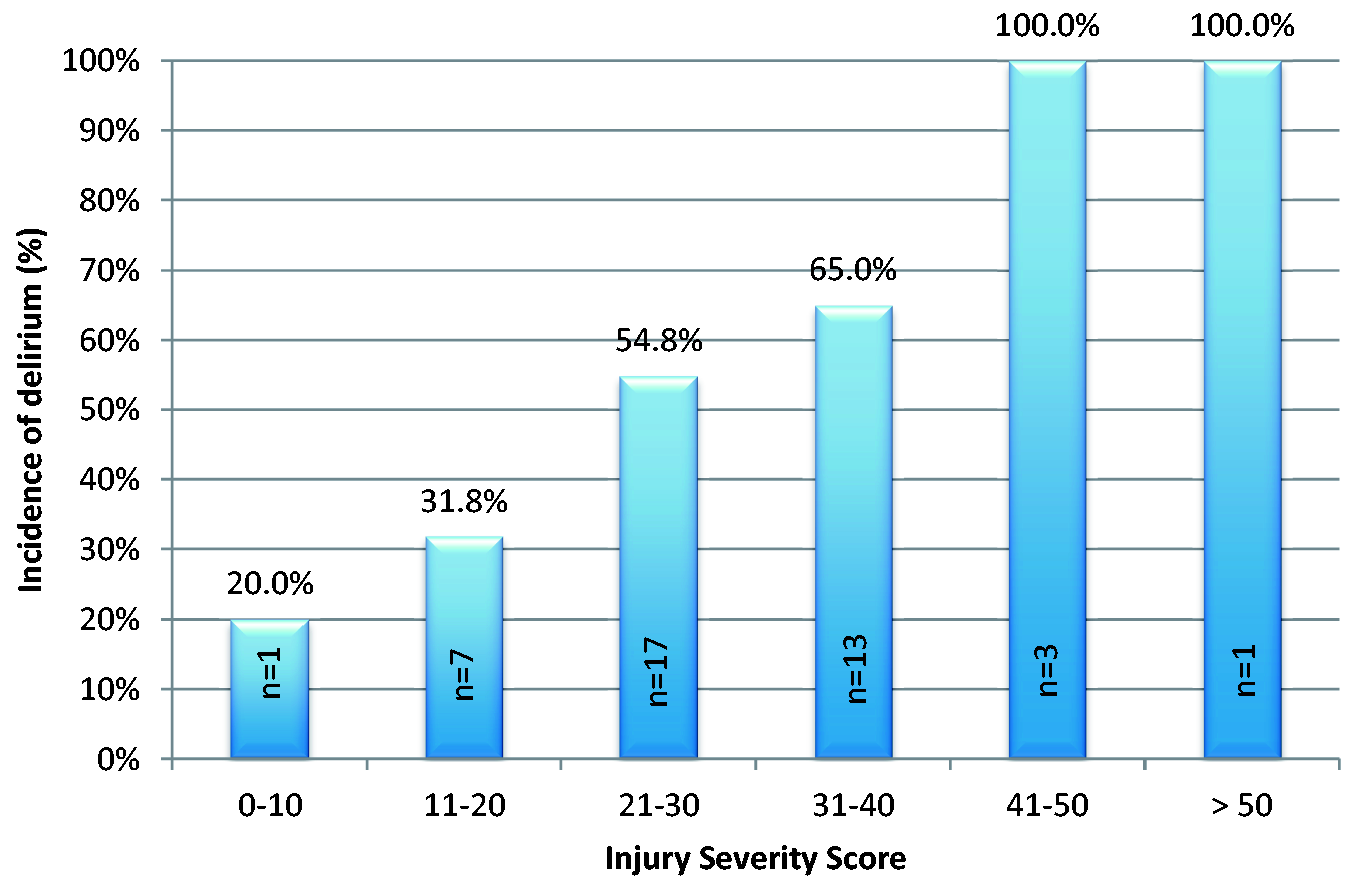
Presence of delirium was also associated with increased duration of both mechanical ventilation and total ICU stay. In patients who experienced at least one delirium-positive day, the median duration of UK mechanical ventilation increased from 4 days to 6.5 days, and median duration of ICU stay increased from 9 days to 12.5 days. Both results were statistically significant with p < 0.005. There was also a significant increase when comparing patients who had more than one delirium-positive day to those who had nil or only one day of delirium (p < 0.005 for both). There was no significant association with age, presence of head injury, mechanism of injury or repatriation time. Association with pain, infection and level of sedation could not be robustly assessed retrospectively. A summary of results is presented in Table 1.
Screening for delirium
There was no documented formal delirium screening on any delirium-positive day.
Management of delirium
Of the 133 delirium-positive days, 92 days (69.2%) received either pharmacological, non-pharmacological or both types of intervention for delirium. Consequently, there was no documented management or intervention on 30.8% of delirium-positive days.
In total, there were 128 documented interventions, of which 85 interventions (66.4%) were pharmacological. The most common choices were haloperidol (19.5%) or an increase in or bolus of sedation (18.0%), for example with propofol or midazolam. By far, the most common non-pharmacological intervention was reassurance or reorientation (23.4%), with exposure to daylight and use of family visits being infrequently implemented. Figure 3 demonstrates the distribution of interventions for delirium.
Histogram showing the distribution of the 128 pharmacological and non-pharmacological interventions over 92 of the 133 delirium-positive days.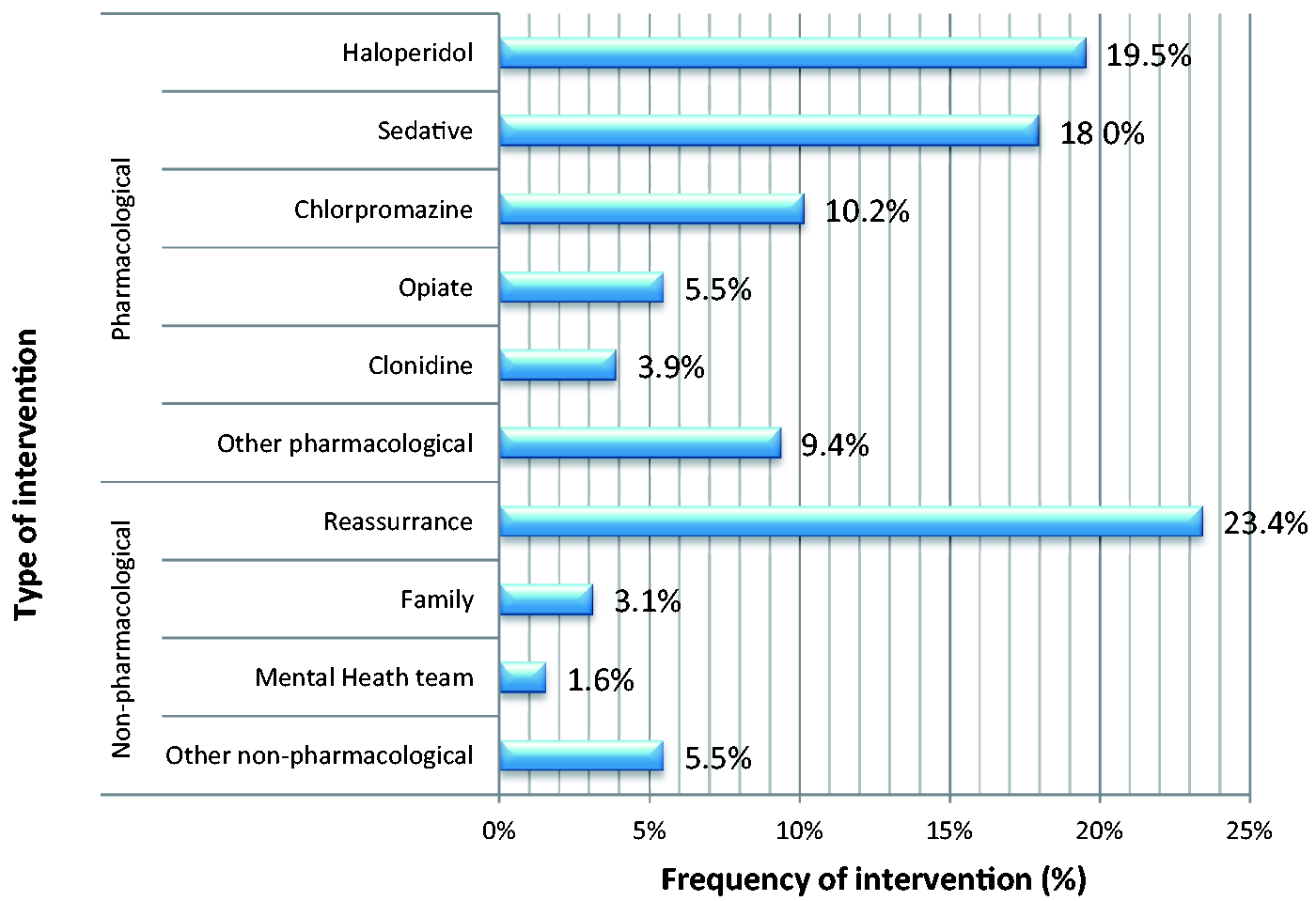
Discussion
Our results report an incidence of delirium of 51.8% among a critical care population of military patients. There is an association between delirium and the severity of injury. We have shown a relationship between delirium and increased length of mechanical ventilation and ICU length of stay; however, we cannot infer whether the causality is due to delirium or severity of critical illness.
The observed incidence of delirium lies within the wide range (20–80%) of reported incidences of delirium in the general population. 4 The PRE-DELERIC scoring system recognises 10 predictive factors: age, APACHE-II score, admission group, coma, infection, metabolic acidosis, use of sedatives and morphine, urea concentration, and urgent admission. 3 Military patients represent a young, previously fit and well, population. On arrival to the UK ICU, their physiological parameters have been largely normalised, with resolution of acid–base and electrolyte imbalances during initial resuscitation and repatriation. However, they have a high incidence of infection owing to significant wound contamination due to mechanism of injury. 13 They were observed to typically receive high doses of opiate analgesia at time of injury and throughout ICU admission, certainly in excess of the PRE-DELERIC threshold of 18.6 mg morphine per 24 h. Additionally, the requirement for evacuation may result in extended sedation for some patients. There are also specific factors to be taken into account. The degree of disorientation for a military patient is unparalleled, with rapid transition from a highly stressed, hostile and militarised environment to the clinical, alien environment of a civilian ICU. It has been reported that when emerging from sedation, military patients may believe that they are still involved in the incident in which they were injured. 14 Military casualties are now surviving unprecedented degrees of trauma, 15 resulting in substantial tissue damage and corresponding ISS. This usually means the requirement of multiple surgical operations. This in turn limits the opportunity to implement sedation holds, a strategy of recognised benefit in the sedated patient. 16 The link between delirium and withdrawal from alcohol and recreational drugs was considered inconsequential in this patient group, due to the heavily policed, dry environment of modern military operations.
The management of delirium in our population was variable, with an emphasis on pharmacological intervention. There is now increasing support for the adoption of standardised management bundles, such as the ABCDE bundle. 17 This incorporates formal screening, for example with the validated CAM-ICU tool, in addition to rationalising polypharmacy and utilising non-pharmacological approaches. However, there is currently insufficient evidence that treating delirium reverses negative outcomes. On the 30.8% of delirium-positive days when no intervention was attempted, it is not clear whether this represents a failure of recognition or no perceived benefit of intervention.
An important limitation is the use of a retrospective diagnosis of delirium. To ensure that this was as robust as possible, a case note review method was developed based on the DSM-IV criteria 8 and on piloting this had good inter-rater reliability. We recognise that this method is likely to have a low sensitivity suggesting that the incidence of delirium may have been an underestimation. This method of assessment did not allow differences in delirium motor subtype to be explored; therefore, hypoactive delirium in particular may have been underestimated. A recent validation of a similar method to ours showed a sensitivity of 0.58, specificity of 0.93 and an area under the receiver operating characteristic curve of 0.86. 9
A further limitation is the introduction of selection bias in our method of patient selection. Our sample was formed from patients who had survived to hospital discharge and who had attended an ICU follow-up clinic (reported as 60% attendance of invited cohort). 2 Additionally, as our patients were all survivors, we were not able to examine the relationship between delirium and mortality. Significantly increased mortality has been previously described amongst older patient groups, 18 with a smaller absolute mortality recognised across all ages, in addition to increased days of mechanical ventilation and prolonged ICU admissions,19,20 However, the mortality rate in this patient population, once arrived in the UK, was 7.65%, a which is low relative to the mortality rate of the general ICU population. This suggests that reviewing mortality as an outcome is less useful in this patient group.
Perhaps of greater relevance would be reviewing the association between delirium and longer-term psychological morbidity. ICU survivors have been found to frequently suffer from post traumatic stress disorder (PTSD), depression and sexual dysfunction, with acute psychological reactions and delirious symptoms in the ICU being the strongest and most modifiable risk factor. 6 The incidence of PTSD has been reported to be as high as 15%. 21 In a group of young, working men, who as a consequence of their occupational exposure are prone to psychological morbidity, such adverse outcomes are particularly relevant. Further work is needed to determine the relationship between ICU delirium and psychological morbidity in survivors.
Conclusion
Delirium is common in military ICU patients following battlefield injuries, and is strongly associated with severity of injury. Management remains inconsistent, possibly because optimal management remains unclear. We recommended further studies and prospective analysis of delirium and its management in this population, including review of the longer-term psychological outcomes in these patients.
Footnotes
Acknowledgements
We are grateful to Flt Lt Lucy Nell, Capt Michael West and Fiona Lovett for their involvement in data collection. The Clinical Information Exploitation Team and Defence Statistics Health are thanked for their assistance in collecting and collating data for this paper. Critical Care clerks at Queen Elizabeth Hospital Birmingham are thanked for their assistance in obtaining APACHE II scores. We thank Dr Peter Nightingale for his help in the statistical analysis and Col Peter Mahoney, Surg Cdr Tim Scott, Wg Cdr Kristina Birch and Dr Kaye England for proof reading and advice.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CB, SR and JW are members of HM Forces and CS previously served as a member of HM Forces.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: TJ is supported jointly by the Research into Ageing Fund; a fund set up and managed by Age UK and the British Geriatrics Society (#367).
Research Ethics
All data used in this cohort analysis were recorded as part of each patients’ routine clinical management. Local registration with QEHB’s audit department as a service evaluation project was obtained to access patient notes; reference CAA-05821-14. Ethical approval not required.