
Abstract
Background
For patients on invasive mechanical ventilation (MV), it is unclear if knowledge of intubation grade influences intensive care unit (ICU) outcome. We aimed to determine if there was an independent relationship between knowledge of intubation grade during ICU admission and in-hospital mortality.
Methods
We performed a retrospective cohort study of all patients receiving invasive MV at the Alfred ICU between December 2011 and February 2015. Demographics, details of admission, the severity of illness, chronic health status, airway detail (unknown or known Cormack–Lehane (CL) grade), MV duration and in-hospital mortality data were collected. Univariable and multivariable analyses were conducted to assess the relationship. The primary outcome was in-hospital mortality, and the secondary outcome was the duration of MV.
Results
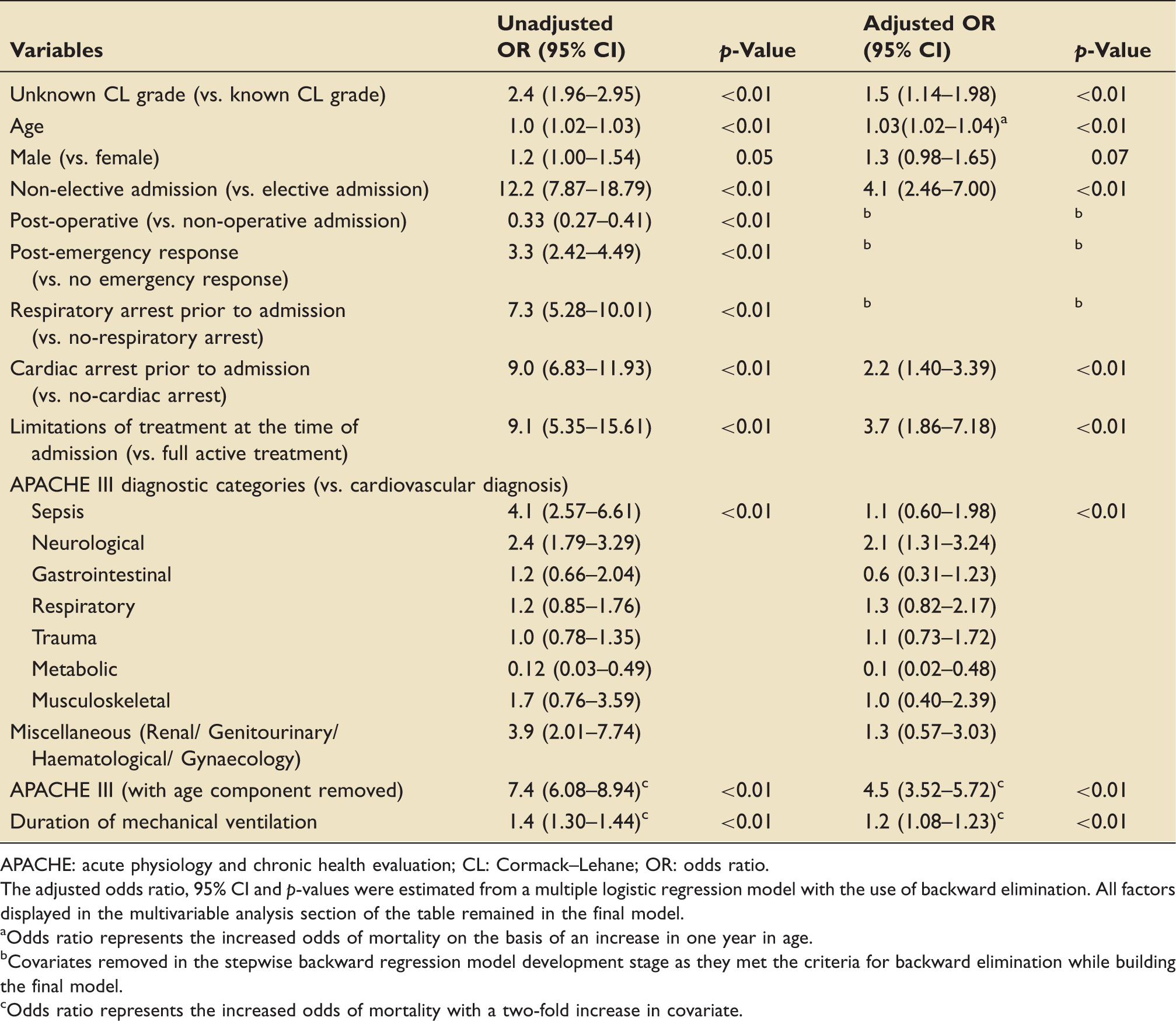
Amongst 3556 patients studied, 611 (17.2%) had an unknown CL grade. Unadjusted mortality was higher in patients with unknown CL grade compared to known CL grade patients (21.6% vs. 9.9%). After adjusting for age, sex, severity of illness, type of ICU admission, cardiac arrest, limitations to treatment and diagnosis, having an unknown CL grade during invasive MV was independently associated with an increase in mortality (adjusted OR 1.5, 95% CI 1.14–1.98, p < 0.01).
Conclusion
Amongst ICU patients receiving MV, not knowing CL grade appears to be independently associated with increased mortality. This information should be communicated and documented in all patients receiving MV in ICU.
Keywords
Introduction
Mechanical ventilation (MV) is the most common indication for intensive care unit (ICU) admission across the world. It accounts for more than 50% of ICU admissions in the tertiary units of Australia and New Zealand (ANZ). 1 For the bed-side clinicians, it is essential to know the intubation details of these patients as it impacts their airway management in ICU. This information, however, is not always available to the bed-side clinicians as a significant number of patients admitted to ICU are intubated outside ICU. In an emergency department (ED) study, which looked at the airway documentation after intubation, the information about the airway grade was found in only 36% of the patients. 2 Such inadequate documentation may lead to loss of critical data during hand-over resulting in morbidity and mortality.
Cormack–Lehane (CL) classification of glottis view during direct laryngoscopy is a widely used system in ANZ for communication of patients at risks of difficult laryngoscopy and subsequent difficult tracheal intubation.3–5 The grades 3 and 4 of this system equate to the American Society of Anaesthesiologists’ ‘difficult laryngoscopy’ definition. It has an estimated incidence in ICU of 11–12%. 5 Such views are associated with prolonged intubation attempts with a resultant increase in peri-intubation complications, particularly in ICU, where patients have limited physiologic reserve and significant comorbidities.6–11 If a patient is known to have grade 3 or 4 views, it is possible to plan and prevent such complications.
It is not known, whether the lack of information about the CL grade of ICU patients receiving MV influences their ICU outcome. It is also not clear whether patients with difficult laryngoscopy grades have worse ICU outcomes. Following a sentinel event and subsequent Coroner’s inquest (see below), 12 a process of routine mandatory CL grade recording was initiated for all patients admitted to our ICU. This provided a unique opportunity to study this relationship. We hypothesised that documentation of CL grade (unknown vs. known; and also the various CL grades) would be independently associated with mortality for patients receiving MV in ICU, even after adjusting for confounding factors.
Sentinel event – Coroners case 12
In 2009, a 42-year-old male had an acute myocardial infarction (AMI) and cardiac arrest at a metropolitan tertiary hospital. Despite coronary artery bypass surgery, he remained in cardiogenic shock and was transferred to the Alfred ICU for consideration for extra-corporeal membrane oxygenation therapy. His cardiogenic shock improved with conservative measures and four days after admission, he had a trial of extubation. Within 1 h he required re-intubation for cerebral irritation and hypoxia. Unfortunately, the re-intubation procedure was complicated. The patient’s known difficult airway at the former hospital was not communicated on inter-hospital transfer. This contributed to shortcomings in extubation and re-intubation planning. This culminated in a cardiac arrest, severe hypoxaemic ischaemic encephalopathy and death.
While there were numerous patients, personnel and system factors contributing to this adverse outcome, the coroner made this recommendation:
“… that when a patient is transferred from one public hospital to another, information about their intubation status and any difficulty with intubation be recorded and conveyed to the receiving hospital.”
Methods
This was a retrospective cohort study, which involved analysis of data from the hospital’s ICU database. Only de-identified patient information was used for analysis.
The study was conducted on patients admitted to the Alfred Hospital ICU, Melbourne, Australia. The unit is a 45-bed quaternary (principally adult) ICU with mixed medical and surgical admissions. It also provides state service for trauma, heart and lung transplantation, mechanical circulatory assistance, cystic fibrosis, HIV, burns and stem cell transplantation.
All intubated patients admitted to the ICU between 1 December 2011 and 28 February 2015 (four years and two months) who had their airway grade entered in the database (individual CL grades or as unknown) were eligible for enrolment. Patients with no airway details entered in the database, patients admitted for end-of-life care, or organ donation were excluded from the study. For patients with readmissions, only the outcomes for the first ICU admission were included in the analysis.
The Alfred ICU prospectively compiles an electronic database of all patients admitted to the ICU. This includes data provided to the Adult Patient Database of Australian and New Zealand Intensive Care Society (ANZICS) regarding patient demographics, severity scores and mortality outcomes. From December 2011, information about the patient’s CL grade was added to this database (either grade 1, 2, 3, 4 or unknown), as a result of the sentinel event and Coroner’s recommendation outlined. 12
Outcomes
The primary outcome measure was in-hospital mortality. The secondary outcome measure was MV duration in hours. Patients were separated into either known or unknown CL grade. Patients with known CL grade were further categorised into an individual CL grade (1, 2 and 3 or 4) based on the assessment of the laryngoscopist at the time of intubation. The CL grades 3 and 4 were combined into one group as these are considered as difficult laryngoscopy grades. 6 Other variables extracted from hospital database included: age, sex, severity of illness score (Acute Physiology, Age and Chronic Health Evaluation, calibrated for Australian hospitals [APCHE III-j]), 13 APACHE-III risk of death, APACHE-III diagnostic categories, ICU admission type (elective vs. non elective), operative status (post-operative vs. non-operative admission), admission following cardiac or respiratory arrest, admission following emergency calls and details of any limitations to treatment.
Ethics
The study was approved by the Alfred Hospital Human Research Ethics Committee (Project 585/15).
Statistical analysis
Data analysis was performed using STATA, version 11.2 (StataCorp LP, College Station, TX, USA). Parametric data are shown as means and SDs, non-parametric data as medians and interquartile ranges (IQR). Difference between groups was determined by Student’s t-test, Wilcoxon rank-sum tests or Kruskal–Wallis test, as applicable. Categorical variables were described as numbers, percentage and proportions, with Chi-square test or Fischer’s exact test to compare two or more groups. Two-sided p < 0.05 were considered to be significant.
For the primary outcome of in-hospital mortality, we performed multivariable logistic regression. Stepwise regression with backward elimination using ‘change in estimate’ method was used for model building. For all models, the CL grade (known vs. unknown or individual CL grades) remained in the model as this was the exposure variable of interest. All other variables entered the model if they had a p-value of <0.25 on univariable analysis and remained in the model if the p-value was significant at 0.05 level or if it was a confounder. A confounder was defined as a covariate, which altered the coefficient of the primary variable by more than 10% when it was removed from the model. The results are expressed as odds ratios (OR) with 95% confidence interval (95% CI). The calibration and discrimination of the model were assessed using Hosmer–Lemeshow C statistic (with its associated p-value) and area under the receiver operating characteristic curve (ROC), respectively. We removed the age component from APACHE III-j score to avoid confounding due to age in the analysis.
For the secondary outcome of MV duration, we performed univariable linear regression after logarithmic transformation of the duration of MV. The results are expressed as geometric mean ratios with 95% confidence interval.
Results
During the study period, there were 8387 ICU admissions. Of these, the following admissions were excluded from the study: 1927 did not have any airway data entered in the database, 2381 patients were not intubated, 76 patients were admitted for palliation or organ donation and 447 were readmission episodes. We had 3556 participants for analysis after these exclusions. Amongst these patients, CL grade was entered as known in 2945 (82.8%) patients and as unknown in 611 (17.2%) patients (Figure 1). Amongst the known CL grade patients 2176 (73.9%), 602 (20.4%) and 167 (5.7%) patients had grades 1, 2 and 3 or 4 views, respectively.
Patient consort diagram.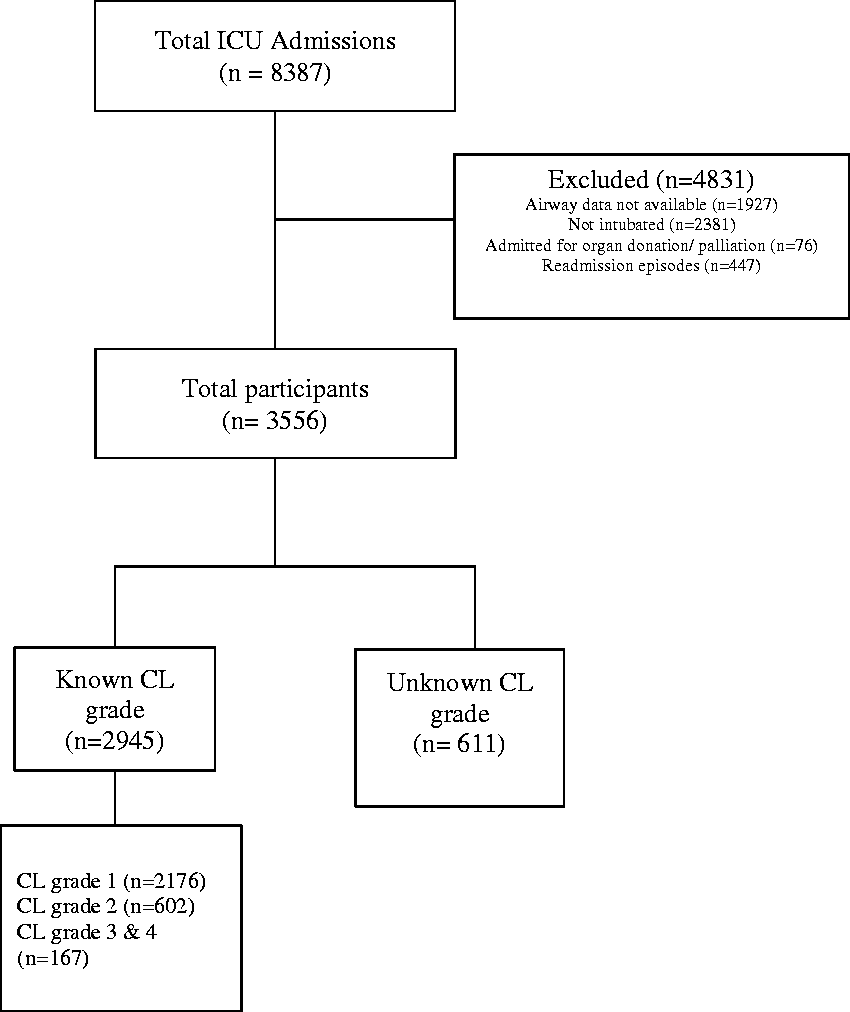
Patient demographics, severity of illness, admission characteristics and diagnostic groups.
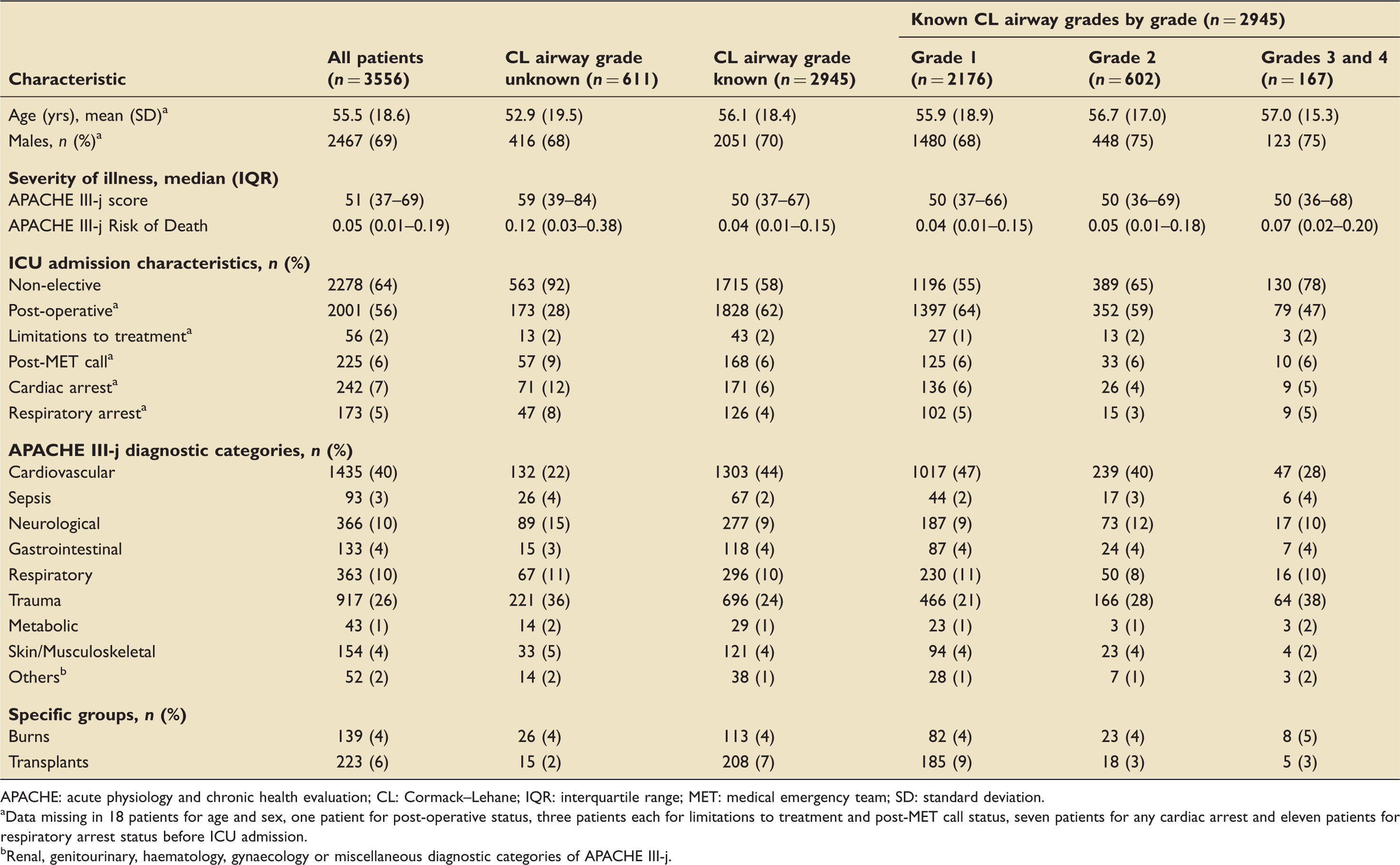
APACHE: acute physiology and chronic health evaluation; CL: Cormack–Lehane; IQR: interquartile range; MET: medical emergency team; SD: standard deviation.
Data missing in 18 patients for age and sex, one patient for post-operative status, three patients each for limitations to treatment and post-MET call status, seven patients for any cardiac arrest and eleven patients for respiratory arrest status before ICU admission.
Renal, genitourinary, haematology, gynaecology or miscellaneous diagnostic categories of APACHE III-j.
In-hospital mortality
Primary outcome: in-hospital mortality.
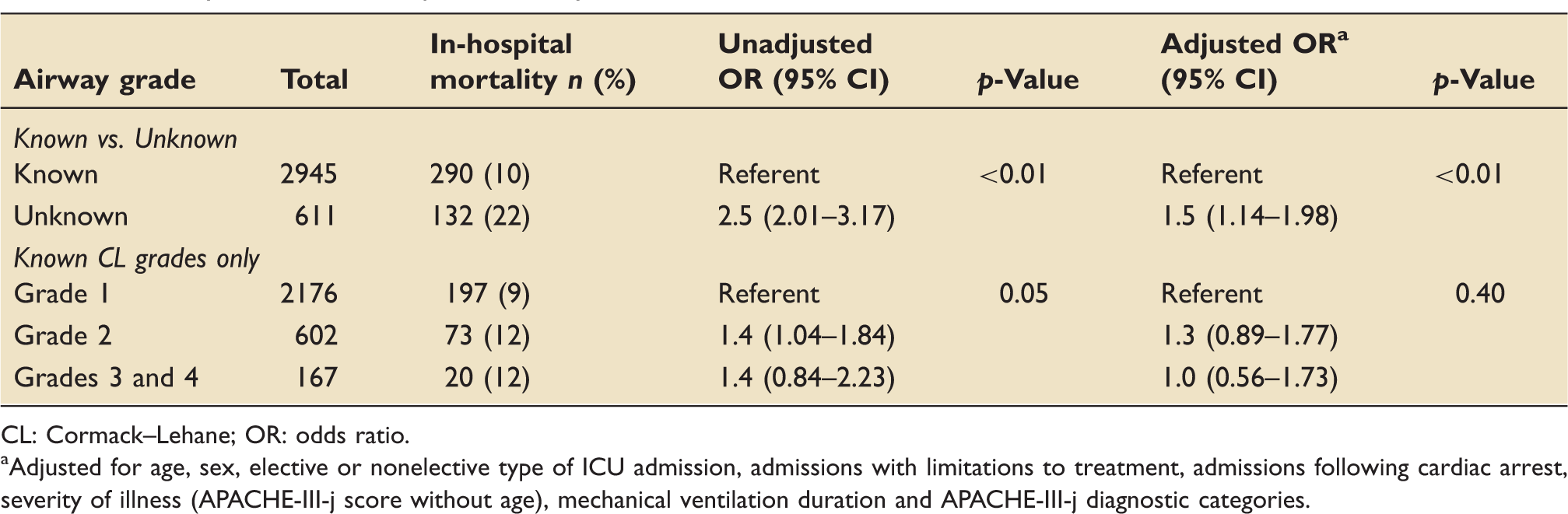
CL: Cormack–Lehane; OR: odds ratio.
Adjusted for age, sex, elective or nonelective type of ICU admission, admissions with limitations to treatment, admissions following cardiac arrest, severity of illness (APACHE-III-j score without age), mechanical ventilation duration and APACHE-III-j diagnostic categories.
Secondary outcome: duration of mechanical ventilation.
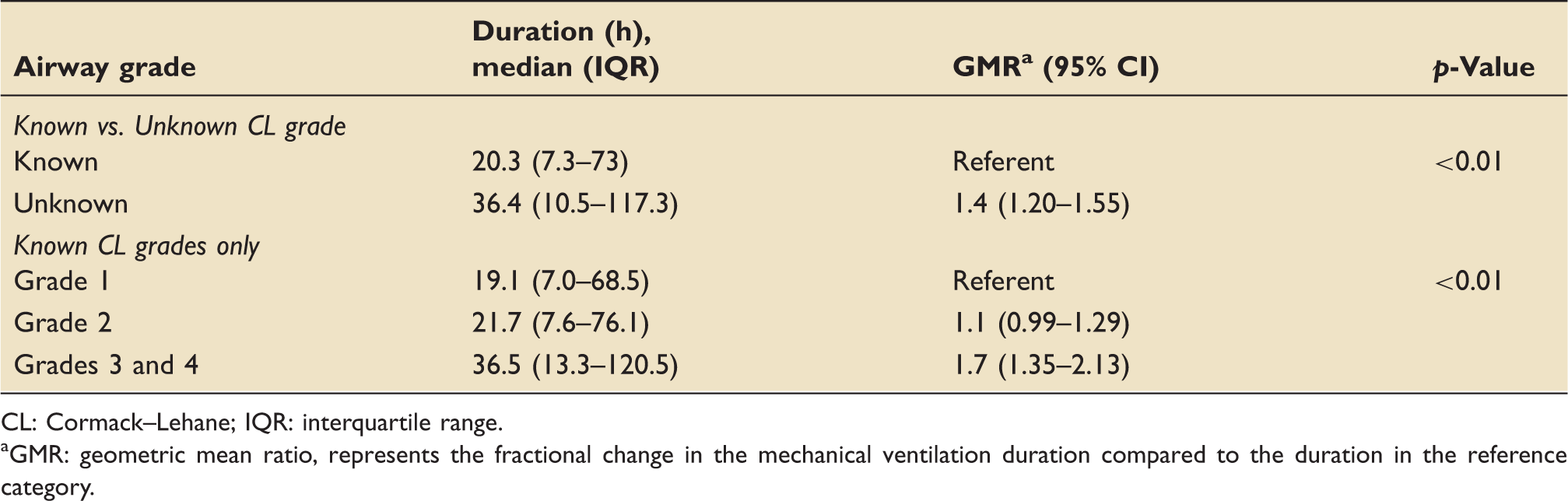
CL: Cormack–Lehane; IQR: interquartile range.
GMR: geometric mean ratio, represents the fractional change in the mechanical ventilation duration compared to the duration in the reference category.
Univariable and multivariable analysis for the association between unknown vs. known CL grade of intubation, covariates and mortality.
APACHE: acute physiology and chronic health evaluation; CL: Cormack–Lehane; OR: odds ratio.
The adjusted odds ratio, 95% CI and p-values were estimated from a multiple logistic regression model with the use of backward elimination. All factors displayed in the multivariable analysis section of the table remained in the final model.
Odds ratio represents the increased odds of mortality on the basis of an increase in one year in age.
Covariates removed in the stepwise backward regression model development stage as they met the criteria for backward elimination while building the final model.
Odds ratio represents the increased odds of mortality with a two-fold increase in covariate.
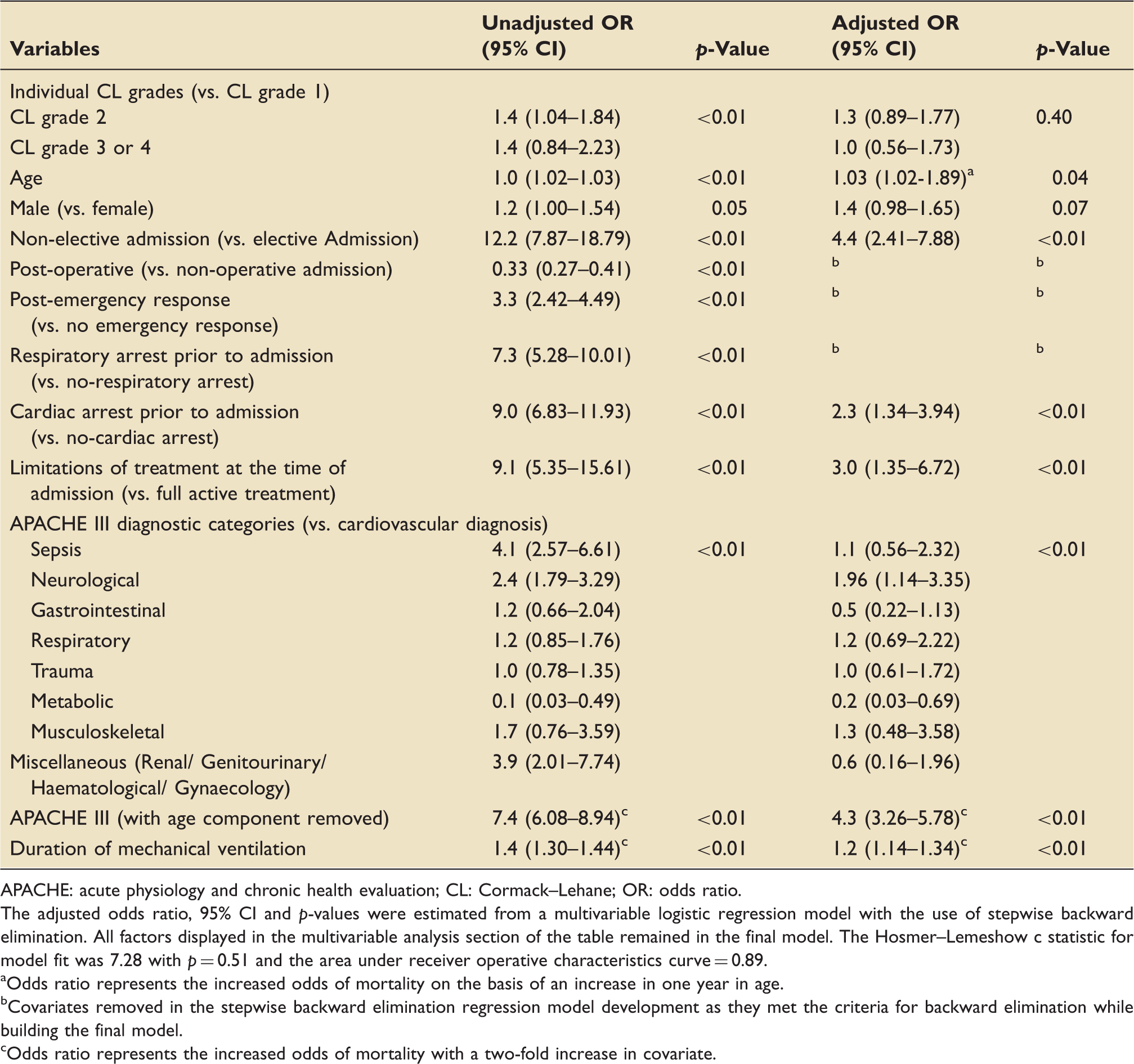
Univariable and multivariable analysis for the association between individual CL grades, covariates and mortality.
APACHE: acute physiology and chronic health evaluation; CL: Cormack–Lehane; OR: odds ratio.
The adjusted odds ratio, 95% CI and p-values were estimated from a multivariable logistic regression model with the use of stepwise backward elimination. All factors displayed in the multivariable analysis section of the table remained in the final model. The Hosmer–Lemeshow c statistic for model fit was 7.28 with p = 0.51 and the area under receiver operative characteristics curve = 0.89.
Odds ratio represents the increased odds of mortality on the basis of an increase in one year in age.
Covariates removed in the stepwise backward elimination regression model development as they met the criteria for backward elimination while building the final model.
Odds ratio represents the increased odds of mortality with a two-fold increase in covariate.
Duration of MV
Duration of MV (Table 3) was longer in those with unknown CL grade compared to those where CL grade was known (median (IQR) 36.4 (10.5–117.3) hours in the unknown vs. 20.3 (7.3–73) hours in the known CL grade group). In the known CL group, there was an increase in MV duration with increasing CL grade (median (IQR) 19.1 (7.0–68.5) hours in grade 1 vs. 21.7 (7.6–76.1) hours in grade 2 vs. 36.5 (13.3–120.5) hours in CL grades 3 or 4 group).
Discussion
In this retrospective study of ventilated patients admitted to a large tertiary hospital ICU, we found that approximately 1 in 6 patients had their CL grade documented as unknown and these patients had 50% higher risk of death than the patients in whom CL grade was recorded even after adjusting for age, sex, severity of illness and various other pre-admission characteristics (adjusted OR, 1.5; 95% CI: 1.14–1.98; p < 0.01). We also found that the MV duration was longer in these patients. When the CL grade was known, higher CL grade patients had longer MV duration compared to lower CL grade patients.
It is well known that airway management in the critical care environment is more challenging compared to elective operating room environment. Simpson et al. 14 found higher episodes of desaturation, hypotension and cardiac arrests during the peri-intubation period in a critical care setting. Mort, 15 in another study of emergency intubations outside the operating theatre, found that multiple attempts at intubation were associated with a dramatic increase in the incidence of hypoxemia, gastric regurgitation, aspiration, bradycardia and cardiac arrest. The fourth National Audit Project (NAP4) from the UK Royal College of Anaesthetists reported 36 critical airway complications in their one year audit of ICU intubations.16,17 Majority of them resulted in either brain death or death. Hence, for ICU clinicians, it is essential to know the CL grade during the previous laryngoscopy to prevent such complications. In a recently published guideline formulated in response to NAP4 findings, Higgs et al. emphasised the importance of human factors and meticulous planning while managing airway in all critically ill patients. In the section of special circumstances, authors mention that patients with known difficult airway should be identified and explicit airway management plan signposted at the bedhead to improve patient safety. However, only case reports, 18 Coroner’s review 10 and anecdotal evidence support the importance of this information. Our research shows that CL grade information is essential and lack of such information is associated with increased risk of mortality for ICU patients.
The reason for this association, however, is not clear. One might hypothesise that unknown CL grades of the patients might result in adverse events during subsequent airway management resulting in higher mortality risk. A study by Jabre et al. 19 found that in emergency intubations, difficult intubation, measured by an intubation difficulty score, was associated with increased morbidity and mortality. In our ICU, during the study period, there were no reports of any critical airway incidents. There were much more vigilance and quality assurance during airway management following the sentinel event. Therefore, observed association may not entirely be due to increased complications related to airway management.
A likely reason for the higher mortality risk seen in our unknown CL group is unknown confounders for which we have not been able to adjust. Another explanation is that CL documentation may be a marker of improvement in the quality of care reflective of a more ordered and thorough documentation process. This has been suggested previously by Phelan et al., 20 in an endotracheal tube placement confirmation study in patients following cardiac arrest.
The percentage of patients in our study with an unknown CL grade (17.2%) is higher than past ‘pre-hospital’ (0.4%) 9 and ICU / emergency studies (5.3%). 14 However, in contrast to our study, which is retrospective and involved a large number of patients over a period of more than three years, both of them were prospective studies conducted over short periods of time. In this study, we included patients as unknown airway if they were explicitly entered as unknown airway in the database. We speculate that unknown grade classification may have been registered due to the following reasons: the airway grade was not known due to poor documentation and hand-over at the time of admission to ICU, CL grade was not known on admission as patient was only intubated during in-patient stay, CL was unknown due to intubation by an indirect laryngoscopy method (i.e. video-laryngoscopy) or CL grade was available but entered by the ICU admission doctor as unknown, in error. Due to the retrospective nature of the study, it was not possible to know the contribution from each of these. Poor documentation and handover is possible and would have higher propensity to occur in emergent non-operative admissions compared to post-operative admissions (unknown CL grade in post-op admissions, 8.7% vs. 28.2% in non-operative admissions in our study). The use of indirect laryngoscopy (mainly via video laryngoscopy) may have contributed to some of the unknown CL grade percentage in our study as video laryngoscopes were introduced in the unit for difficult airway intubation during the study period. Video laryngoscopy is typically used in patients with predicted difficult airways and positional limitations, and it is not always possible to interchange the view obtained on them with the CL grade views. 5 A recent Australian Emergency and ICU department audit found that 45% of intubations were via video laryngoscopy. 21 All these factors may have introduced unmeasured confounders in our study.
With regard to the individual CL grades, our intubation grade distribution was consistent with a previous study. 14 We found no difference in mortality. These findings are similar to past studies which demonstrated that difficult intubation (CL grades 3 and 4 or repeated laryngoscopy attempts) created higher peri-intubation complications.9,10,15,22 However, these were not associated with higher mortality. 14 Only the study by Jabre et al. 19 found a positive association between the intubation difficulty score and mortality for emergency intubations.
Strengths and limitations
Our study represents a large, mixed adult ICU population over a period of more than three years with clear, concise methodology and statistics. Data collected was part of the formal hospital ICU database that was prospectively recorded, independently managed and quality assured by personnel outside of the research group. The primary and secondary outcomes were objective, easy to measure and not explicitly collected for this study, thereby limiting ascertainment bias. Multivariable regression analysis was conducted to adjust for age, the severity of illness and other known confounding factors.
However, several limitations warrant note. Firstly, the study’s retrospective nature means causality cannot be proven. Secondly, the ICU database was not explicitly designed for capturing peri-intubation information. Apart from CL grade, the peri-intubation details and complications were not available. We only included cases entered as unknown intubation in the database for analysis and did not include the patients for whom this data was missing. Also, we did not use imputation for missing data in our analysis. As the database did not have information available for patients after discharge, we used in-hospital mortality rather than the standard 90-day mortality for reporting mortality outcome.
For the individual CL grade comparisons, further limitations surround the subjective nature and significant inter and intra-observer variability of CL grading.4,7 The individual CL grades 3 or 4 contain small numbers that may have resulted in type II error in the analysis.
Generalisability
The findings of this adult-based study, from a robust prospectively created ICU database, would apply to other mixed tertiary medical and surgical ICU settings. However, these factors also limit its generalisability to a general ICU patient population.
Conclusions
Lack of the knowledge of CL grade appears to be independently associated with an increased risk of mortality for the patients receiving MV in ICU. It is not possible to determine whether the observed mortality difference is linked to airway management during ICU stay or whether it is the result of unmeasured confounders in this study. Future prospective studies should be designed to look at the factors associated with the lack of details of CL grade during ICU stay and their association with mortality.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.