
Abstract
Olanzapine, a second-generation antipsychotic, is used in both adult and pediatric populations for schizophrenia, bipolar disorder, and depression and has been associated with autonomic dysregulation in the setting of overdose. Guanfacine is a sympatholytic drug used in the treatment of attention deficit hyperactivity disorder and has also been associated with autonomic dysfunction. We present a unique case of a 17-year-old male who overdosed on 340 mg of olanzapine and 189 mg of extended-release guanfacine with a previously unreported adverse event. Specifically, five days after ingestion, he developed a 5–8 s sinus pause every time he forcefully swallowed any beverage, suggestive of a vagal hypersensitivity reaction. The report will review the autonomic dysfunction of olanzapine and guanfacine and management of asymptomatic sinus pause in the critical care setting.
Keywords
Introduction
Treatment of hyperactivity and impulse disorders in children and adolescents relies on several pharmacologic agents. While sinus pause is often a benign finding in both children and adults,1,2 sinus pause in the critical care setting must be distinguished from lethal arrhythmias. We present a case of sinus pause in the setting of olanzapine and guanfacine extended release (ER) overdose occurring after resolution of the patient’s bradycardia and presentation of hypotension. To our knowledge, the high dosage of guanfacine ER overdose (189 mg) has been unreported in the literature as well as the phenomenon of swallow-induced sinus pause in the setting of overdose.
Case report
A 17-year-old male with medical history of attention deficit and hyperactivity disorder (ADHD), mood disorder, and conduct disorder was transported to the local emergency department accompanied by his legal guardians after intentionally ingesting 68 olanzapine 5 mg tablets (340 mg total) and 63 guanfacine extended-release 3 mg (189 mg total) tablets in a suicide attempt. Upon presentation to the outside facility, he was given naloxone 2 mg intravenously and 3 l of normal saline for bradycardia and hypotension with limited response. Chest X-ray and CT head were normal and he was transferred to our tertiary care center for further workup.
On examination, the patient had a patent airway, a respiratory rate of 16 breaths per minute, and peripheral oxygen saturation of 98% on room air. His blood pressure was 108/74 mmHg, heart rate was 58 beats/min, and temperature was 36.1℃. He was oriented only to self but neither time nor place, and could only keep his eyes open for a few seconds before falling asleep. No focal neurologic deficits were noted. Pupils were 3 mm bilaterally and reactive to light. Other than his bradycardia, the cardiovascular exam was otherwise normal including a regular rhythm and no murmurs.
A collateral history from the patient’s legal guardian revealed that he had no prior suicide attempts and was completely well the evening before the event. Olanzapine and guanfacine ER were his only regular medications prior to admission. The amount ingested was estimated based on the remaining tablets left in the respective pill bottles. His family did not report a history of known drug, alcohol, or tobacco abuse or prior suicide attempts. In the emergency department, a urine drug screen, paracetamatol (acetaminophen) level, and salicylate level returned negative. Point-of-care glucose, basic biochemistry, creatine kinase, and complete blood count with differential returned within normal range. Electrocardiogram (ECG) revealed sinus bradycardia. The regional Poison Control Center was contacted and recommended naloxone as needed for bradycardia or respiratory depression but noted that it often had little effect as seen at the outside facility.
The patient was admitted to the pediatric ICU for hemodynamic monitoring and neurologic monitoring. The patient developed a waxing and waning sensorium with multiple episodes of agitation during his first night of hospitalization. His bradycardia remained stable with a heart rate in the low 50 beats per minute (bpm) and his sensorium fluctuated with moments of relative alertness during the first 24 h. His sensorium continued to fluctuate over the first 72 h of his admission, but by the fourth day of his admission, he became alert and oriented to person, place and time and was able to carry on full conversations with only mild slurring of his speech. As his coordination continued to improve, he was allowed to take ice chips without any issues. His guardians noted that overnight he appeared to be experiencing hallucinations, specifically pointing to people and animals not present. On his fourth day of admission, the bradycardia resolved (with a heart rate in the 70–85 bpm range) but the patient experienced a pre-syncopal episode when standing up. Workup revealed significant orthostatic hypotension, and he was subsequently kept in the ICU for further monitoring.
On the following day, the patient’s bedside monitor alarmed as “asystole” and the patient’s nurse quickly responded to the bedside to find the patient casually drinking a soda. The rhythm strip from the first event was captured and presented in Figure 1. When questioned about the event, the patient reported only drinking a soda prior to the event. He was asked to drink the same volume of water, and the bedside telemetry again demonstrated a sinus pause. The patient continued to remain asymptomatic during these events. Subsequent ECG demonstrated normal sinus rhythm. Over the next 24 h, this event could be repeated on command every time he consumed a beverage forcefully, as shown in the Supplemental Video.
On his sixth day of admission, the sinus pause phenomenon stopped, his hemodynamic parameters remained stable, and he continued to demonstrate an alert mental status. He was transferred to inpatient psychiatric facility for further management where he resumed his previous daily dosage of each drug.
Autonomic dysregulation of olanzapine and guanfacine in overdose
This case report, to our knowledge, is the first to report the unusual phenomenon of swallow-induced sinus pause in the setting of olanzapine and guanfacine overdose. Both of these medications will be reviewed. Since both drugs’ autonomic properties affect the brainstem, the delayed timeline of his vagal hypersensitivity cannot be clearly distinguished between olanzapine and guanfacine in this study due to simultaneous ingestion of both.
Atypical antipsychotic medications such as olanzapine are more frequently used in children and adolescents than the typical antipsychotics due to their apparently lower risk of adverse events. 3 Olanzapine has a half-life of 37 h in 10–18 year olds and 30 h in adults. 4 There have been several case reports of isolated intentional olanzapine overdose in adolescents, 5 which generally resulted in fluctuating metal status changes, respiratory depression, and non-fatal anti-cholinergic effects that resolved within 48 h of ingestion. 6 There have also been reported cases of olanzapine toxicity resulting in fatalities either as a sole agent or in combination with other medications. 7 There is evidence to suggest that olanzapine acts centrally on the brain stem, and specifically on the dorsal motor nucleus of the vagus nerve, which has been a proposed mechanism of its metabolic effects resulting in hyperglycemia in the liver. 8 The phenomenon of vagal hypersensitivity in the setting of olanzapine overdose resulting in sinus pause may result from these effects in the brainstem, although no formal in vivo studies have documented this phenomenon.
Guanfacine ER, an α-agonist, is currently approved to treat ADHD in children and adolescents. It was previously approved as an anti-hypertensive because of its selective stimulation of α2-adrenoreceptors in the brainstem, which explains the prolonged bradycardia and hypotension seen in case reports of its overdose. 9 Guanfacine ER, which provides fewer lapses in concentration compared to the immediate release form, has a half-life between 16.6 and 17.5 h and demonstrates linear pharmacokinetics with multiple daily doses. 10 While exact data of guanfacine extended-release use in the United States and Europe are not available, a recent retrospective cohort study utilizing the MarketScan Commercial or Multi-State Medicaid claims databases found that approximately 12% of patients with ADHD were initiated either atomoxetine or guanfacine in 2010. 11 It is likely that guanfacine use in this population is even higher in Europe, where guanfacine is approved as monotherapy for patients in which stimulants are not appropriate. 12 There have been few case reports of guanfacine overdose in children, though many of them involve much smaller doses than our patient ingested. In fact, our literature search revealed accidental ingestion of 6 mg by an 8-year-old boy, 9 25 mg by a 16-year-old female, 13 4 mg by a 2-year-old male, 14 and 9 mg by a 12-year-old boy. 15 Our patient ingested 189 mg of extended-release guanfacine, which represents over 60 times his daily dose. While he did benefit from fluid resuscitation for hypotension, he did not require pressor support and did not respond to naloxone, which demonstrates variable response in the literature.9,16
Management of sinus pause
Sinus pause, also known as sinoatrial arrest or sinus block, is a transient termination of electrical impulse in the heart that results from intermittent failure of sinus node impulse generation. A pause of 2 to 3 s does not necessarily indicate disease. Sinus pause has been documented in normal adults and children under 24 h continuous ECG monitoring.1,2 The etiology of sinus pause is broad, including ischemic causes, inflammatory and fibrotic infiltration of the sinoatrial node, sleep apnea, anti-arrhythmic medications, and excessive vagal tone. Unlike AV nodal blocks, which can be pathologic, sinus pause evaluation primarily rests on whether the patient is having symptoms. Asymptomatic patients often do not require treatment, with treatment of the underlying etiology as indicated. Occasionally, permanent pacemakers are used to treat sinus pause in the setting of sick sinus syndrome or in symptomatic patients. 17 Because our patient was asymptomatic and could induce the sinus pause phenomenon at will, our management plan involved continuous hemodynamic monitoring without any pharmacologic intervention. He recovered shortly thereafter, which supports the “watch and wait approach” to sinus pause in the critical care setting as described in the previous literature.
This event, to our knowledge, is the first reported case of a delayed, inducible sinus pause in the setting of olanzapine and guanfacine ER overdose. As the use of these medications becomes more widespread in the adolescent population, this rare event may occur in the setting of massive guanfacine ER overdose during suicide attempts. The management solution supported both by our patient and the literature is no further intervention for the sinus pause itself with hemodynamic monitoring until resolution.
Telemetry readout demonstrating swallow-induced sinus pause.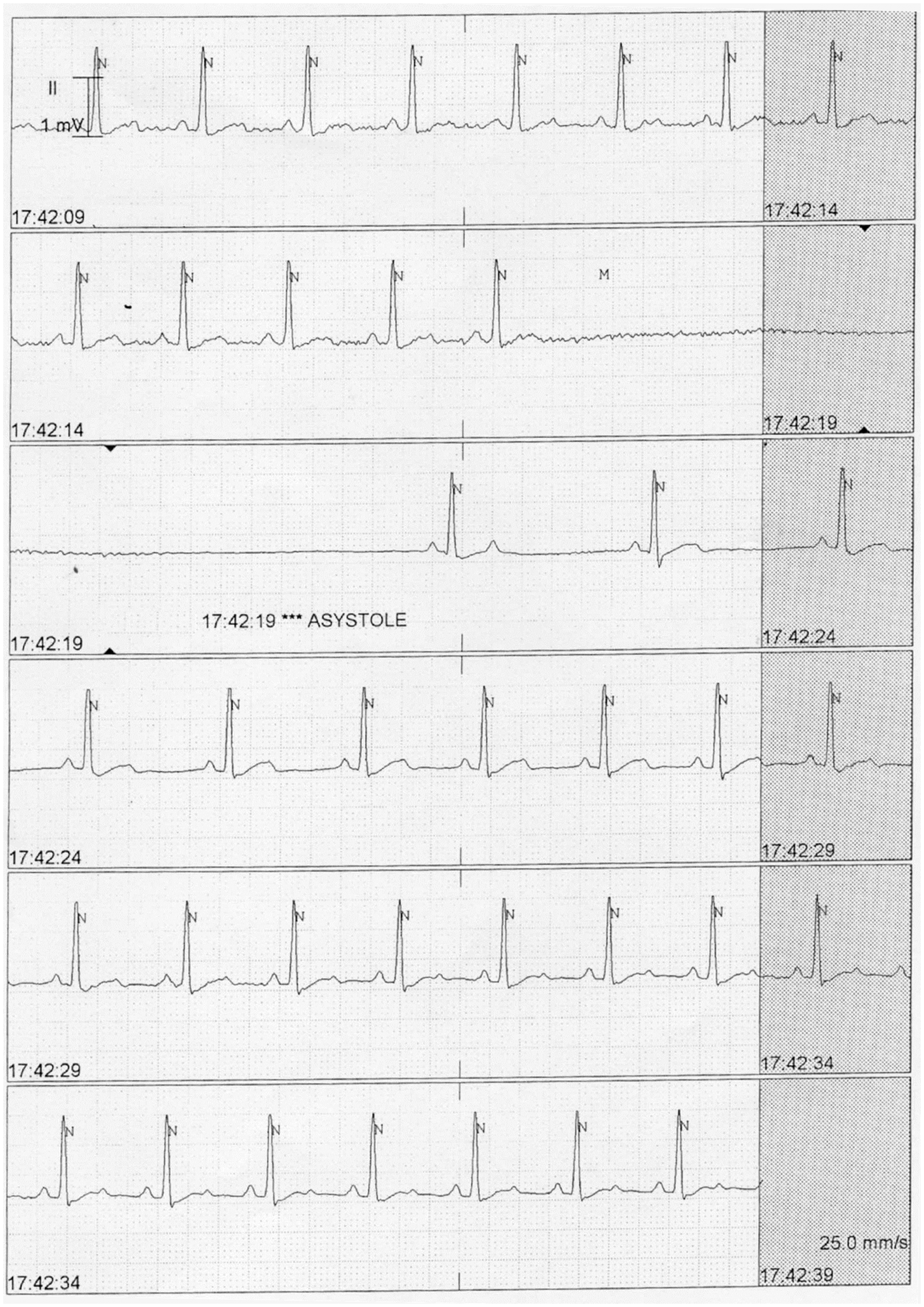
Footnotes
Patient consent
Written consent was obtained from the patient’s legal guardian.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article