
Abstract
Background
Elderly patients are frequently considered poor candidates for continuous renal replacement therapy in intensive care units, but with little evidence base.
Methods
We gathered data regarding patients requiring continuous renal replacement therapy at our institution’s intensive care unit during 2012–2014, and compared outcomes between patients of 75 years or older, and younger patients.
Results
Older patients had similar intensive care unit mortality to younger patients (41.5% vs. 36.1%, p = 0.21), but higher hospital mortality (54.2% vs. 44.0%, p = 0.02), and one-year mortality (63.6% vs. 50.6%, p = 0.005). There were no significant differences in dialysis-dependence rates between older and younger patients at intensive care unit discharge (31.9% vs. 35.8%, p = 0.50), and hospital discharge (18.5% vs. 24.2%, 0.32). Rates of new dialysis-dependence between older and younger patients at time of hospital discharge were similar (10.2% vs. 6.0%, p = 0.20).
Conclusions
Intensivists should not withhold continuous renal replacement therapy based on age alone. Other factors should be considered in triage of patients for intensive care unit and continuous renal replacement therapy.
Introduction
Continuous renal replacement therapy (CRRT) is a common necessity in intensive care units (ICUs), whether for established end-stage renal disease (ESRD) or acute derangements. Mortality is high in both situations, with reported rates frequently above 50% in centres of excellence.1,2 Recovery of renal function among survivors who suffered an acute insult is usually good.1,3 However, patients of advanced age are often presumed to have such poor prospective outcomes from ICU admission and CRRT that their care is not escalated to that level.4,5 In addition, given their poorer baseline renal function, 6 older patients may be considered to have a higher risk of long-term dialysis dependency. The evidence to support these perceptions is limited and it is an area worthy of further exploration.
Our aim was to examine long-term dialysis dependence and mortality among patients requiring CRRT in ICU. We aimed to compare outcomes between patients of 75 years or older, and younger patients, to see if there were meaningful differences. Our long-term goal was that findings from this study would help inform evidence-based decision making among ICU physicians when faced with critical illness among older patients.
Methods
Definitions
Our definitions and nomenclature regarding renal replacement therapy are based on the acute dialysis quality initiative (ADQI) definition document of 2002. 7 Our definition of baseline ESRD was a documented diagnosis of ESRD prior to admission, or evidence of regular dialysis prior to admission. Recovery of renal function was defined as the absence of need for renal replacement therapy (RRT) at hospital discharge as a meaningful patient outcome.
Study population
The inclusion criteria for our study were limited to admission to our institution’s ICU, and a requirement for CRRT. All patients admitted to a tertiary academic centre ICU between 1 January 2012 and 31 December 2014, who required CRRT, were included in the study. These included scheduled admissions post-operatively, emergency admissions from wards and emergency department, and transfers from other centres.
To avoid assessment of multiple outcomes for a single patient, patients who had multiple ICU admissions requiring CRRT had data recorded only for the first admission.
Data collection and categorisation
Our main data source was the critical care audit database for 2012–2014 of a tertiary academic 18 bed mixed general-surgical ICU (approximately 1300 admissions per annum). Each patient had a unique identifier (MRN number) and an electronic ICU and hospital record. Additional data collection was from the Mater Misericordiae University Hospital (MMUH) electronic patient record. Data collected included demographic information, medical history, laboratory results including estimated glomerular filtration rate (eGFR) on admission, admission criteria, dialysis documentation, mortality and discharge summary. Outcomes at discharge from ICU and from hospital were recorded from hospital records; outcomes at one year were collated from records of hospital follow-up (for example, outpatient clinic letters) or published death notices in newspapers and online.
Data analysis
Data were collated and analysed using Microsoft Excel software (Microsoft Corporation, Redmond, WA, USA). Comparison of eGFR between groups was performed with ANOVA. Differences were considered to be statistically significant at the level of p < 0.05.
Ethics
Research ethics committee approval was obtained from the MMUH Institutional Review Board.
Results
General demographics
There were 450 patient admissions included in the analysis. Of these, 157 patients pertained to 2012, 155 to 2013, and 138 to 2014; 292 patients were male and 158 were female. Mean age was 63.3 years, median age 66, range 18–93 (Figure 1). Demographic and admission characteristics of patient subgroups are presented in Table 1.
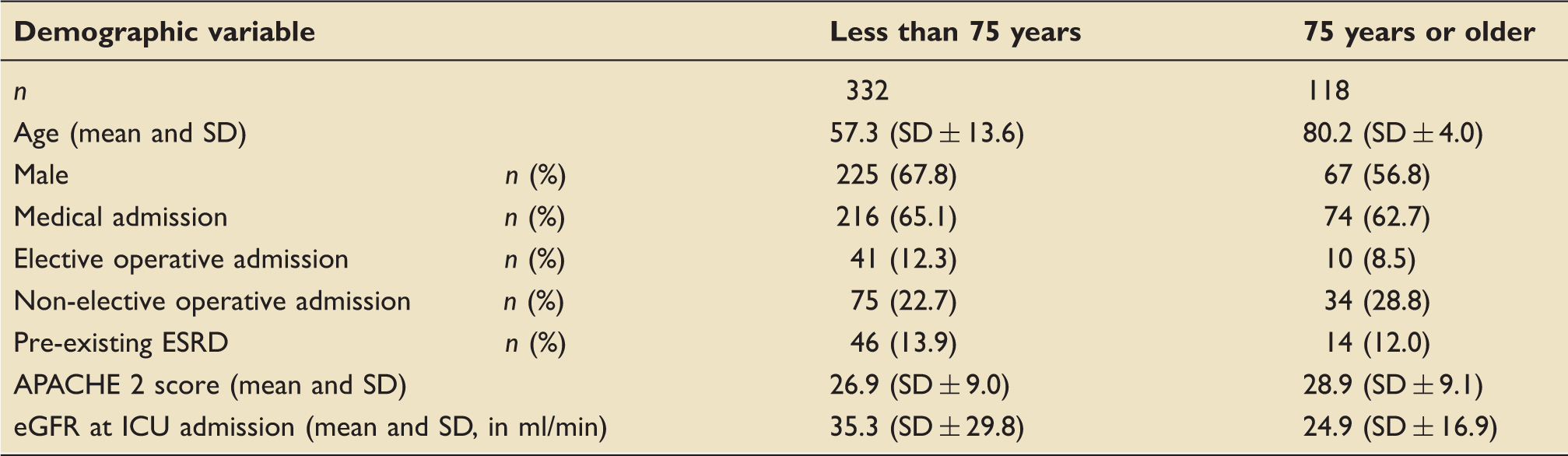
Patients admitted to ICU requiring CRRT 2012–2014, by age group and sex. Demographic and admission characteristics of older and younger patient populations. eGFR: estimated glomerular filtration rate; ESRD: established end-stage renal disease; ICU: intensive care unit.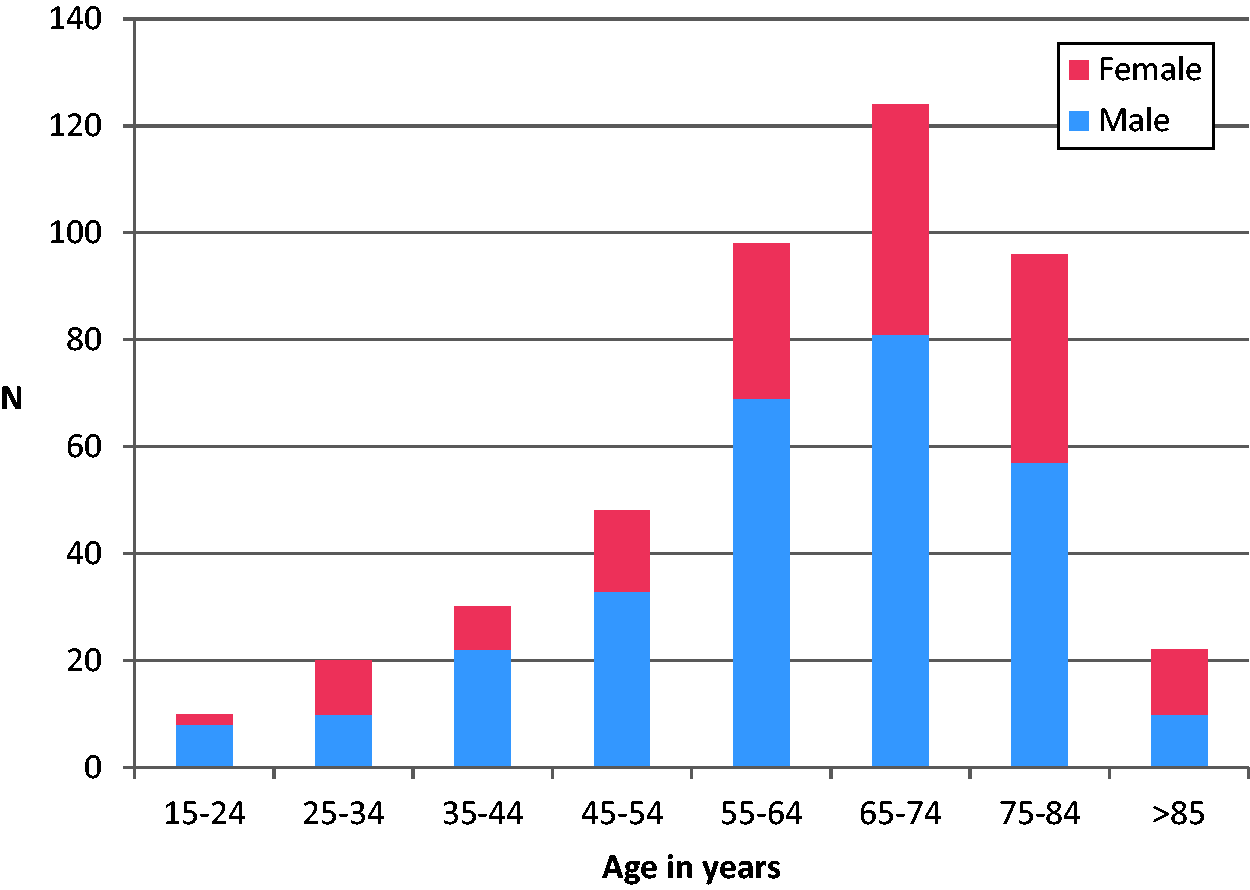
CRRT
The median interval to CRRT was 15 (IQR 4–44.5) h. Mean duration of CRRT was 7.7 days, with a median of 5 (IQR 3–10) days. Patients 75 years and older had a shorter mean duration on CRRT than younger patients (6.3 vs. 8.2 days), and a shorter median interval to commencement of CRRT (13.5 vs. 16.0 h).
Outcomes
Mortality and dialysis-dependence on ICU discharge and hospital discharge among patients admitted to ICU who required CRRT, 2012–2014.
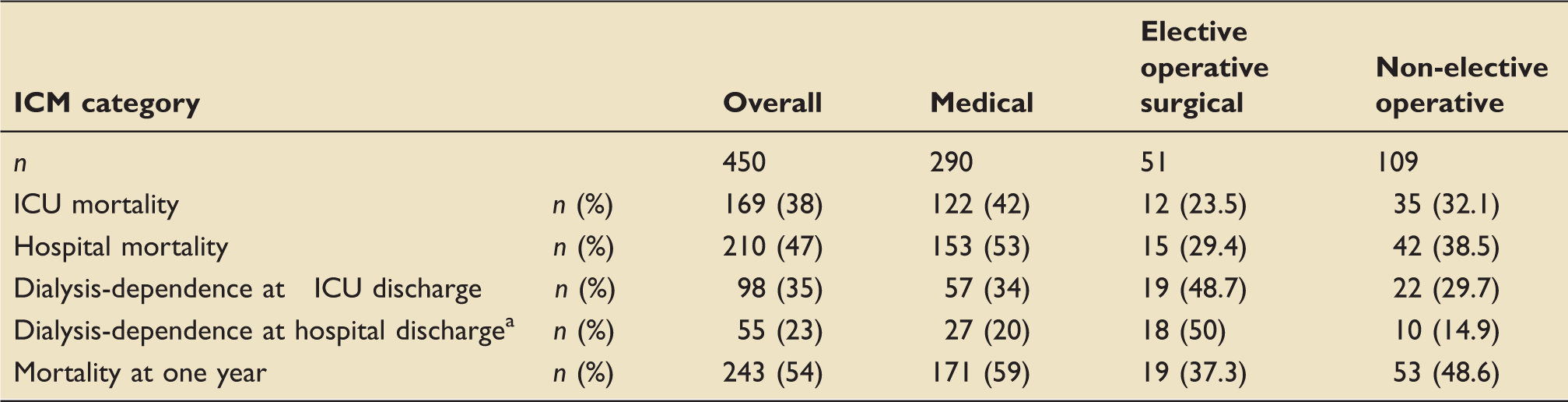
Dialysis-dependence was unknown for 3 of 240 patients at time of hospital discharge.
CRRT: continuous renal replacement therapy; ICU: intensive care unit.
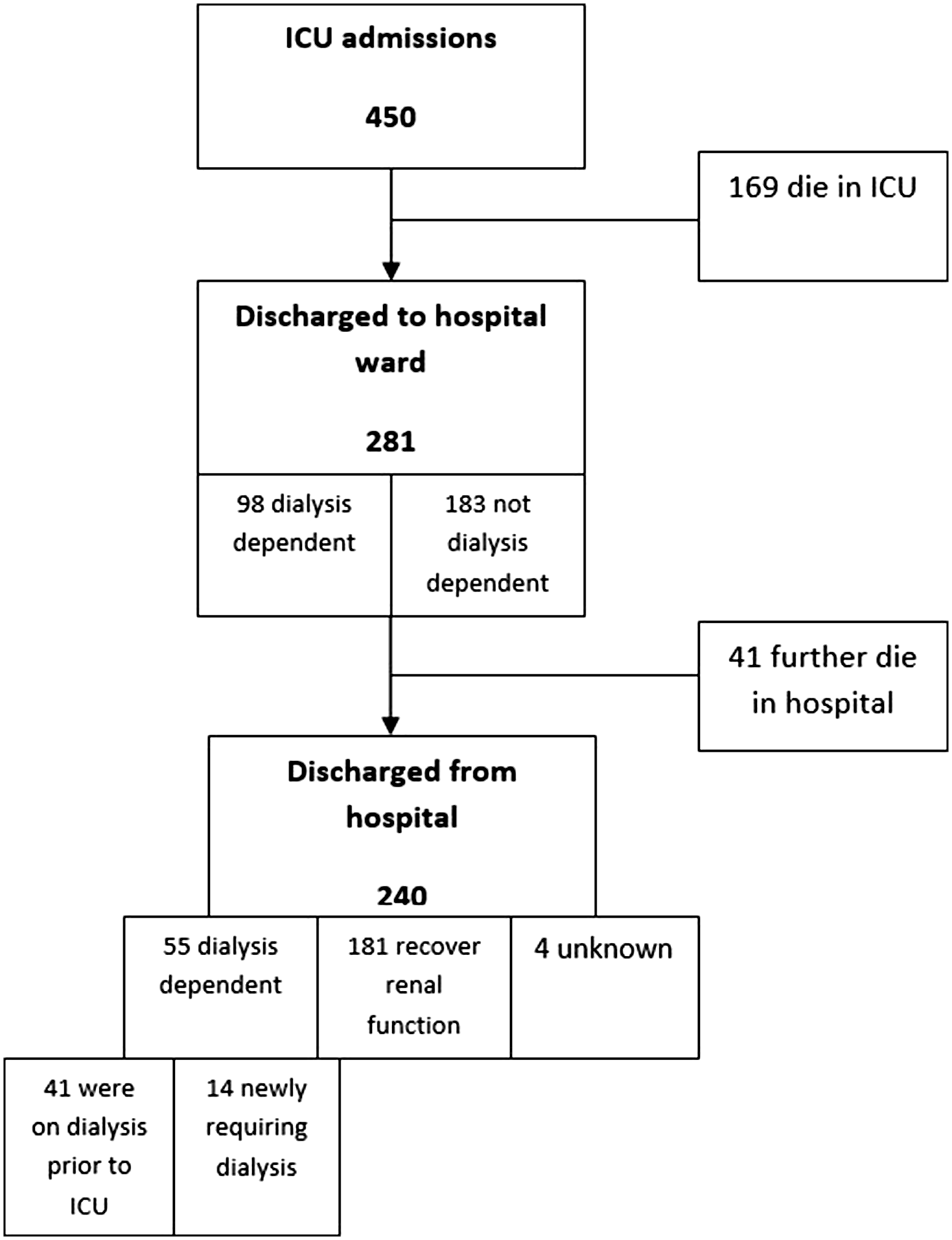
Flow chart of outcomes in study cohort.
Outcomes according to age category and renal diagnosis among patients admitted to ICU who required CRRT, 2012–2014.
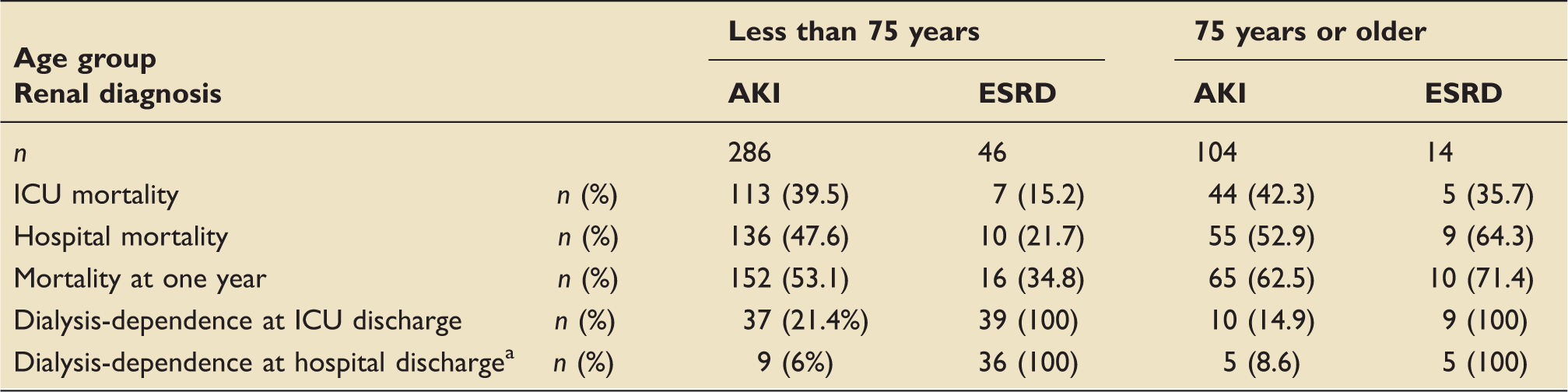
Dialysis-dependence was unknown for 3 of 240 patients at time of hospital discharge.
ESRD: established end-stage renal disease; ICU: intensive care unit.
There was no significant difference in dialysis dependence in older patients compared to younger patients at ICU discharge (31.9% vs. 35.8%, p = 0.50), or at hospital discharge (18.5% vs. 24.2%, p = 0.33). Among all patients 75 years or older without pre-existing ESRD who survived their admission, 5 of 49 (10.2%) had a new requirement for dialysis. The difference between this and the rate in younger patients, which was 9 of 150 (6.0%), did not reach statistical significance (p = 0.20). Admission eGFR was significantly lower in the older patients than in the younger patients (p = 0.0003).
The ESRD patients of 75 years or greater had no statistically significant differences in mortality rate compared to non-ESRD patients of 75 years or greater at ICU discharge (36% vs. 42%, p = 0.63), hospital discharge (64% vs. 53%, p = 0.39) or at one year (71% vs. 62.5%, p = 0.49) (Table 3).
Discussion
Given growing and competing demands on scarce critical care resources, and an associated ageing population, the question of patient triage for critical care grows in importance. Information regarding prognosis, both relating to mortality and long-term morbidity, is of major importance to these decisions. In particular, recent work has focused on the significance of frailty in outcomes of older patients, rather than solely considering patient age. 8
Our comparison of outcomes between older and younger patients who required an escalation of care to CRRT in ICU demonstrates a significantly higher mortality among older patients during their entire hospital admission, but not during the ICU admission alone. There was no significant difference in long-term dialysis dependence between the groups.
With regard to mortality, the absence of a significant difference in mortality between older and younger patients at the point of ICU discharge, which might intuitively be expected, may reflect clinician triage decisions. Specifically, intensivists may be selecting out elderly patients with fewer comorbidities and perceived greater likelihood of survival, which has been described in other work.9–11 It may also, however, reflect a true change in outcome, as suggested in ELDICUS II: that elderly patients enjoy a greater benefit from ICU admission than non-elderly patients. 5
When mortality outcomes are examined according to renal diagnosis as well as age, however, some differences become apparent. For those with an AKI diagnosis, ICU mortality and hospital mortality are persistently similar between older and younger patients. By contrast, when comparing the ICU and hospital mortality of ESRD patients of 75 years or older, and ESRD patients younger than 75, there is a large difference apparent, with higher mortality for the older group. A possible explanation for this is that the older group are more unwell than the younger group at time of ICU admission, given their higher APACHE 2 score (median 25.0 vs. 22.5) and the greater proportion being non-elective admissions (85.7% vs. 41.3%). While a difference in APACHE 2 score also exists between older patients with AKI and younger patients with AKI, the effect on mortality is likely amplified among ESRD patients due to the small numbers involved.
With regard to the higher one-year mortality for older ESRD patients than for younger patients, an explanation may be found in the work of Allegretti et al. 1 They noted age to be a predictor of post-discharge mortality among patients with ESRD. The one-year mortality of patients 75 or greater and with ESRD in our study was very high (71.4%, 10/14 patients). By contrast, one-year mortality among patients less than 75 years with ESRD was 34.8% (16/46 patients). In another population-based study of 619 ESRD patients admitted to ICU, age was the only demographic factor independently associated with mortality at one year. 12
Among patients 75 years or older, our study did not identify a significant difference in ICU, hospital or one-year mortality between patients with pre-existing ESRD and those without ESRD. Prior work has identified illness severity on admission, rather than ESRD status per se, as the main driver of in-hospital mortality among elderly patients with ESRD, 13 and that short-term outcomes are favourable among ESRD patients compared to those admitted with AKI requiring CRRT. 14 Interpretation of findings is limited by the small numbers involved with these characteristics in our study(14 patients of 75 years or older had pre-existing ESRD).
With regard to dialysis-dependence among elderly patients requiring CRRT, intensivists’ perception of their increased risk of ESRD is likely attributable to the established relationship between ageing and decline in glomerular filtration rate. 6 Concerns have been raised in some work, however, that reduced eGFR among older adults may not represent “disease,” as most of these patients will never develop ESRD, and the use of age-specific cut-points for staging CKD has been proposed. 15
Our examination of dialysis-dependence rates at time of ICU discharge and hospital discharge demonstrated no significant difference between elderly and younger patients, despite a lower mean eGFR on admission among the older patient group. Of particular interest is the rate of new ESRD in those originally admitted with AKI, as opposed to pre-existing ESRD. Our analysis identified no significant difference in the risk of new ESRD between elderly patients or younger patients at time of hospital discharge. This may reflect the hypothesis that reduced eGFR in the elderly does not confer the same increased propensity to ESRD as it does in younger patients.
The rates of new dialysis-dependence among patients with AKI requiring CRRT in our work (10.2% for older patients, 6.0% for younger patients) are similar to those identified at 180 days in a large cohort study in Denmark (10.1% for those 70 years or older, 5.6% for those 15 to 49 years, and 8.3% for those 50 to 69 years). 3
Limitations
Ours is a single-centre retrospective study, with a mixed population of elective operative, non-elective operative and medical admissions.
While we were able to analyse in detail those who were admitted to ICU, a limitation was that, as a retrospective study, we could not include those who were not accepted for ICU admission. This concern, that intensivists may consciously or subconsciously select for admission a cohort with better survival prospects, has been a focus of much work in recent years. 4
Follow-up was incomplete, as outcomes regarding mortality were unavailable for 54 patients (12% of the total cohort at admission) at one year, and consistent outcomes regarding dialysis-dependence were not available beyond hospital discharge.
Small sample size is a limitation of this study when examining subgroups, such as older patients with ESRD.
Conclusions
Our findings do not support the conclusion that intensivists should withhold CRRT based on age alone. Mortality rates at time of ICU discharge among CRRT patients aged 75 years or older do not differ significantly from mortality rates in younger patients. Older patients do, however, have a higher mortality at time of hospital discharge and one year from initial admission. In addition, there is a persistently high mortality risk among older patients even in an elective operative setting. The poor long-term outcomes in the older patient group with ESRD may influence patients’ and intensivists’ care decisions in times of critical illness, and necessitate a broader assessment of the patient’s functional independence prior to escalation of care. Regarding the assessment and triage of such patients, factors such as a Clinical Frailty Score should be included rather than the need for CRRT on its own.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.