
Abstract
Background
Lung protective ventilation with tidal volumes (VT) of 6–8 ml per kg ideal body weight have been shown to reduce mortality in patients with acute respiratory distress syndrome and reduce post-operative pulmonary complications in major abdominal surgery. Following a local audit on weight recording, the Southcoast Perioperative Audit and Research Collaboration (SPARC) conducted a regional multi-disciplinary survey on the current practice in lung protective ventilation in the Wessex region. This resulted in a quality improvement project improving lung protective ventilation across these intensive care units.
Methods
Over one-week period in January over two consecutive years, lung protective ventilation parameters of mandatory ventilated patients (above the age of 18 years) were audited in intensive care units in the Wessex region.
Results
A total 1843 hours of mandatory ventilation were audited. The quality improvement project led to an improvement of lung protective ventilation with an average of 30% higher duration of ventilation with VT < 8 ml/kg ideal body weight. There was a suggestion that documentation of height and weight on admission to intensive care units improved compliance with lung protective ventilation.
Conclusions
Adherence to lung protective ventilation is variable across intensive care units but can be improved by recording patient’s weight and height accurately and using simple chart to help calculate the appropriate tidal volume. Additionally, this project demonstrates how a regional audit and quality improvement network can help to facilitate regional quality improvement.
Keywords
Background
In 2000, ARDSNet demonstrated that mechanical ventilation with tidal volumes (VT) of 6–8 ml/kg ideal body weight (IBW) improved mortality in patients with acute lung injury (ALI) and acute respiratory distress syndrome (ARDS) compared to the traditional tidal volumes (12 ml/kg IBW). Lower tidal volumes were associated with reduction in 28-day breathing without assistance, ventilator free days and non-pulmonary organ failures. 1 This strategy also appears useful for patients undergoing abdominal surgery. 2
In 2013, a small single-centre audit in Portsmouth ICU showed inadequate practice of documentation of patient’s weight. Following the local audit, the Southcoast Peri-operative Audit and Research Collaboration (SPARC) performed a survey to assess the current practice of the multidisciplinary team (MDT) in ICU on weight and height recording in all 12 ICUs in the Wessex region in 2014. A total of 451 responses to the survey were received, which highlighted that there were significant knowledge gaps in identifying what weight should be used for lung protective ventilation (LPV) strategies. Following this survey, SPARC audited the adherence to LPV in all ICUs in Wessex over one-week period in two consecutive years. It was identified that adherence to LPV protocols was variable in Wessex ICUs. The summation of these result identified that accurate documentation of IBW improves audited compliance with LPV.
This quality improvement project aimed to demonstrate the benefit of collaboration and identify areas of good practice to implement this practice in other regional ICUs. The goal was to improve adherence to LPV and the care of patients with ARDS.
Methods
Two-week long, multicentre audits of LPV were performed a year apart with an intervention led by trainee intensive care doctors in-between. Every patient over 18 years of age receiving mandatory mode ventilation in participating ICUs were included. Patients with suspected or actual raised intracranial pressure were excluded.
As part of the quality improvement (QI) project, local leads (doctors in training) were appointed in each ICU to initiate change and promote LPV. Ulnar length and VT tables (see online Appendix) were distributed to all bed spaces to assist documentation of IBW and VT for mandatory ventilated patients. Standardised teaching to the MDT was also provided by each local lead.
For each audit, IBW was calculated using the Devine formula from measured height or ulnar length. The recommended VT for each patient was calculated and assessed every 4 hours during times of mandatory ventilation. Additionally, patient age, primary diagnosis, FiO2, PEEP, peak pressures and fluid balance were recorded. Compliance with LPV was expressed as a percentage of total time ventilated.
Results
LPV audit results January 2015
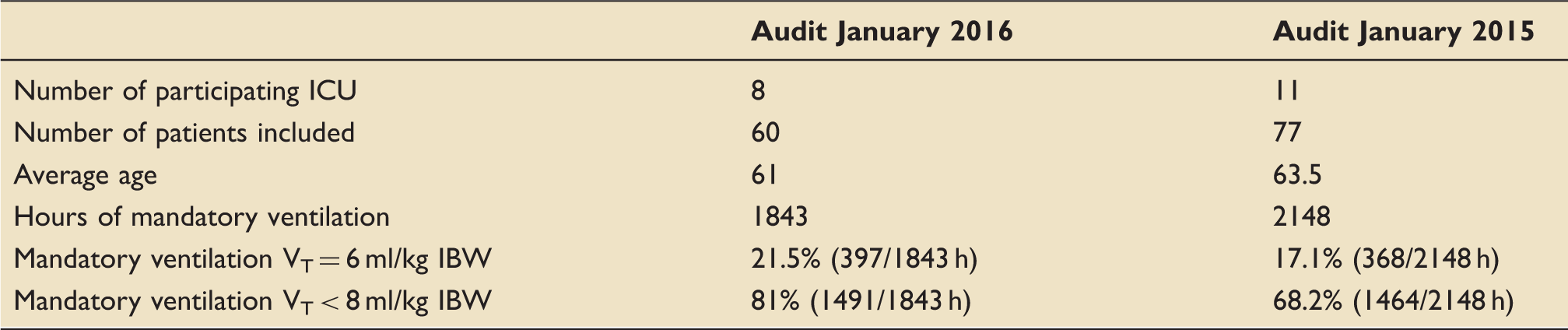
Seventy-seven patients (average age of 63.5 years) over 11 ICU in Wessex were included, and 2148 hours of mandatory ventilation were audited (see Table 1). Mandatory ventilated patients received VT < 8 ml/kg IBW in 68.2% (1464/2148 hours) of the time. In 17.1% (368/2148) of the time, mandatory ventilated patients received VT 6 ml/kg IBW. It came apparent that mandatory and accurate documentation of height and weight on admission to ICU improves audited compliance with LPV.
LPV audit results January 2016
Overview of results (see Table 1)
Sixty patients in eight of the original ICUs were included; mean age was 61 and 1843 hours of mandatory ventilation were audited. Mandatory ventilated patients received VT < 8 ml/kg IBW 81% of the time (1491, 1843 hours). In 21.5% (397/1843) of the time, mandatory ventilated patients received VT 6 ml/kg IBW. In 65% of cases, IBW was recorded which was either calculated from height or derived from ulnar length.
Group and subgroup analysis of LPV audit January 2016
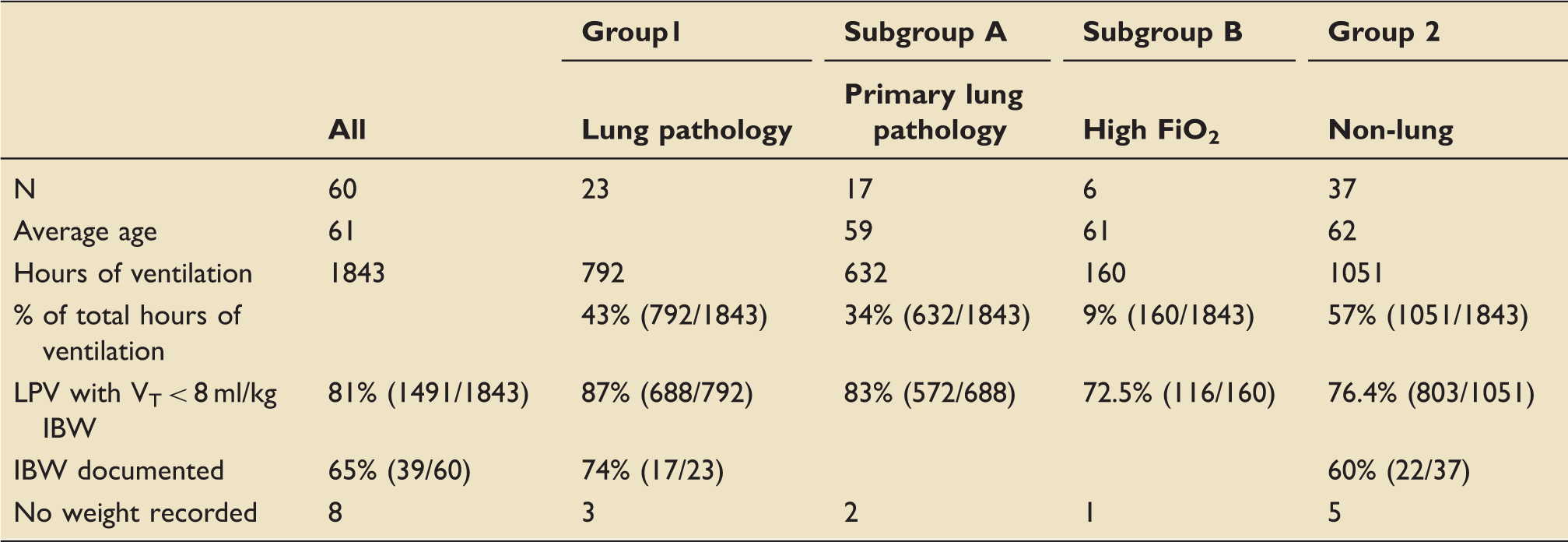
The 60 audited patients were divided into two groups (see Table 2). Group 1 consists of patients who had primary lung pathology or complications (n = 23). Group 2 (n = 37) were mandatory ventilated due to post-operative issues, cardiovascular compromise (sepsis other than chest, cardiovascular arrests) and neurological problems.
Group 1 was divided into Subgroups A (patients with a primary lung diagnosis or complications (for example, respiratory failure secondary to pneumonia, ARDS) n = 17) and Subgroup B (all patients with high oxygen requirements (FiO2 > 0.5 in at least two consecutive data collection points), n = 6).
Patient data
Comparison of audit results of 2015 and 2016.
Subgroup analysis of data from LPV audit January 2016.
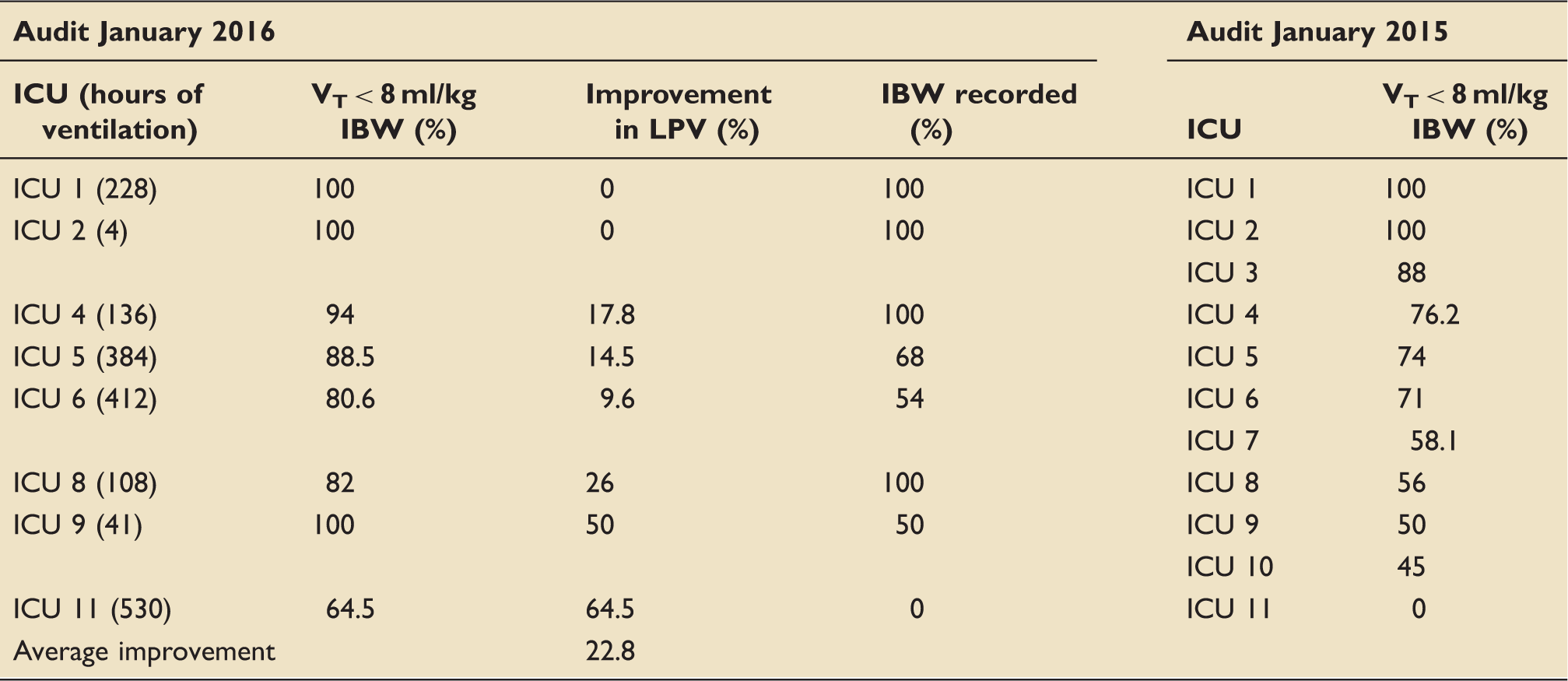
Quality improvement over time.
IBW: ideal body weight; ICU: intensive care unit; VT: tidal volume.
Adherence to LPV
VT < 8 ml/kg of IBW were used in 81% (1491/1843) of the time. The adherence to LPV with VT < 8 ml/kg of IBW was better in Group 1 (patients with primary lung pathology, 87% (688/792), see Figure 1). In Group 2, patients were ventilated with VT < 8 ml/kg of IBW in 76.5% of time.
Group 1 adherence to LPV with TV > 8 ml/kg, TV < 8 ml/kg IBW and TV = 6 ml/kg IBW.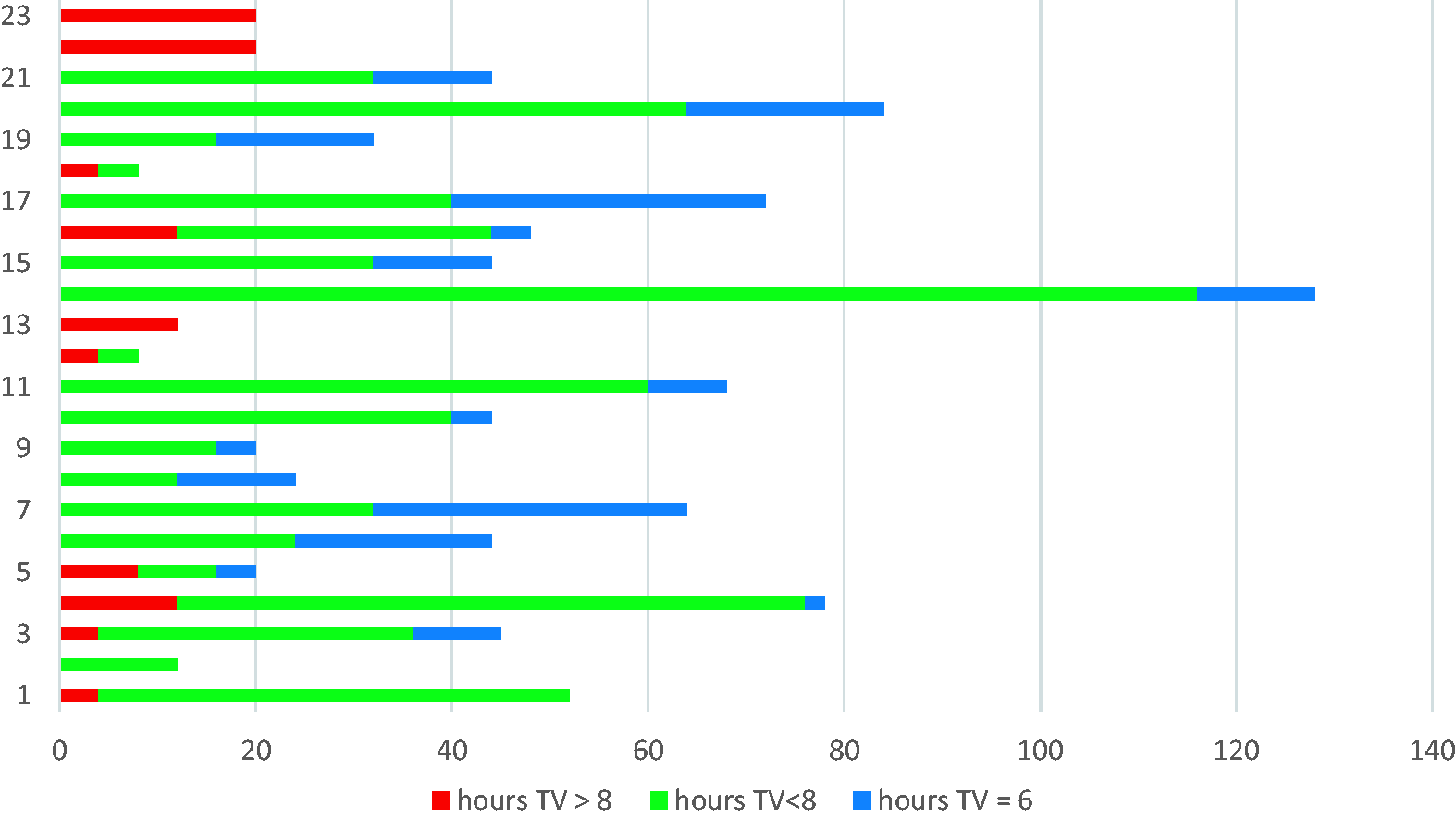
Other ventilator parameters: FiO2, PEEP and plateau pressure
In 100% of cases, FiO2 and PEEP was documented. In the examined patient cohort, the FiO2 was at an average of 0.45, whereas the average PEEP used was 8 cmH2O (minimum of 5 cmH2O, maximum of 20 cmH2O). In Group 1 (primary lung pathology or complication), an average FiO2 of 0.5 with an average PEEP of 9 (5–15) cmH2O was used. In 39 (39/60) patients, plateau pressure was documented. In 37 (37/39), plateau pressure was documented, which remained below 30 cmH2O as recommended.
Documentation of IBW as part of LPV: Subgroup analysis from LPV audit January 2016
In 65% of patients (39/60), IBW was documented. In eight cases, no weight or height recording was made. In Group 1 (patient with primary lung pathology or high oxygen requirements), IBW was recorded in 74% (17/23). In Group 2, IBW was recorded 60% (22/37) of the time.
Documentation of IBW as part of LPV: Quality improvement (QI) over time
The audit in 2015 demonstrated that ICU Number 1 and 2, who documented patients IBW on admission to ICU, were 100% compliant with LPV (see Table 3). IBW is calculated from the patient’s height. Patient’s height is either known, measured or derived from ulnar length (see online Appendix). The QI Project led to an improvement of LPV with an average of 30% higher duration of ventilation with low tidal volumes.
Discussion
The difficulties in the treatment of ARDS lie in the early diagnosis. The following new technologies help to recognise ARDS. Lung ultrasound assesses lung recruitment during ventilator adjustment. Electrical impedance tomography (EIT) identifies regional differences in ventilation. Current trials are running to understand how oesophageal pressure measurement can aid clinicians to understand the global lung stress and consequent ventilation adjustment. In small human studies, single-indicator transpulmonary thermodilution extravascular lung water (EVLW) correlates with lung injury severity and mortalities. 3
The prevalence of ARDS seems to be around 10% of ICU admission with a hospital mortality between 35% and 46% depending on the severity of ARDS. 4
As per the original ARDSNet protocol, the ventilation strategy should aim for initial VT of 8 ml/kg IBW. This should be reduced further with the aim to achieve VT of 6 ml/kg IBW if pH (7.30–7.45) and plateau pressure (<30 cmH2O) allows. 1
A prospective randomized Xtravent-study by Bein et al. suggested that the use of very low tidal volumes (VT ≈ 3 ml/kg IBW) combined with extracorporeal CO2 removal has the potential to further reduce ventilator induced lung injury (VILI) compared with a ‘normal’ lung protective management. 5
Further two ongoing trials aim to establish the benefit of very low tidal volumes (<6 ml/kg IBW) facilitated by extracorporeal CO2 removal. SUPERNOVA (Strategy of UltaProtective Lung Ventilation With Extracoporeal CO2 Removal for New-Onset Moderate to seVere ARDS) is a pilot feasibility and safety study on low-flow extracoporeal CO2 removal to achieve a safe reduction of VT to 4 ml/kg IBW in patients with moderate ARDS. The REST (pRotective vEntilation with veno-venouS lung assisT in respiratory failure) study is an ongoing randomized controlled trial which aims to determine whether Veno-Venous Extracorporeal Carbon Dioxide Removal (VV-ECCO2R) and lower VT in mechanically ventilated patients with hypoxaemic respiratory failure improves 90 day mortality.
LUNG SAFE (Large observational study to Understand the Global impact of Severe Acute respiratory FailurE) reviewed data of ARDS patients in 50 countries. They established that adherence to LPV strategies was poor with only two-thirds of patients with ARDS receiving VT < 8 ml/kg of IBW. 4
An official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guideline for mechanical ventilation in adult patient with ARDS recommends the following intervention. Patients with ARDS should receive limited tidal volumes (4–8 ml/kg predicted body weight) and inspiratory pressures (plateau pressure < 30 cmH2O). Patients with severe ARDS should receive prone positioning for more than 12 hours per day. High-frequency oscillatory ventilation (HFOV) should not be used. Patients with moderate or severe ARDS should receive higher rather than lower levels of PEEP and should receive recruitment manoeuvres.
This project was a multicentre quality improvement project in LPV across Wessex ICUs. Following the quality improvement project, 22.8% more hours of LPV with VT < 8 ml/kg IBW was achieved. It demonstrated that documentation of height and weight on admission to ICU improves compliance with LPV. This project highlights how collaboration in medicine accelerates improvement in the quality of patient care.
Strength of this audit
This regional multicentre audit across up to 11 ICUs in the Wessex region captures a patient population and clinical practice which is likely to be representative for most regions in the UK.
The initial survey on the current practice in LPV showed a variety of current practice across the ICUs in the region consistent with current literature. 4 This study highlights how basic adjustment in clinical practice, like mandatory measurement of patient weight on admission to ICU, can have a huge positive impact on patient’s care. It demonstrates how important it is to get the basics of patient care right. The accurate documentation of patient weight achieved by this QI project has the potential to achieve an improvement in areas of antibiotic and vasopressor prescribing too, both of which are based on patient’s weight.
It demonstrates how a small local audit can lead to meaningful regional multicentre quality improvement project and enable regional and national improvement in patient care. It highlights the benefit of collaborative work between trainees across the region and the importance of collaboration groups like SPARC. This regional quality improvement project was shortlisted for consideration of national trainee project supported by the Research and Audit Federation of Trainees (RAFT). RAFT is the national trainee-led body representing multiple UK regional anaesthetic trainee research networks like SPARC in Wessex. RAFT is supported by the Royal College of Anaesthetist (RCoA) and other associations to improve access to research and promote collaboration of trainees across the country. Regional collaboration of trainees like SPARC and national collaboration like RAFT encourage trainees to come forward with their ideas and improve patient care on a bigger scale.
Furthermore, electronic platforms like Life QI, the health and social care quality improvement platform, can be used for collaboration of future project. It enables users to learn from and built on each other’s progress to enable more efficient and effective quality improvement. It could enable future trainees to perform further projects for example in LPV with ultra-low tidal volumes with the network of SPARC trainees supporting the quality improvement.
Limitation of this audit
The group of patients audited is very heterogeneous with a wide range of age, body weight and diagnosis and does not exclusively include patients with ARDS. ICU Number 2 and 9 have only had 4 hours and 41 hours, respectively, of mandatory ventilation which suggest that not all patient data was captured. ICU 11 had the highest data collection with over 500 hours of mandatory ventilation but the poorest performance in LPV which potentially skewed the overall results.
This study does not audit all parts of the ARDSNet study and does not include analysis of PEEP, FiO2 and plateau pressures. These parameters were part of the data collection but due to variation in ventilator settings and small numbers of patients an analysis of these parameters was not appropriate. However, where documented, the plateau pressure remained in recommended range 100% of the time.
Unanswered questions and future research
Since the publication of the initial ARDSNet study, 1 there have been multiple trials aimed to establish the best treatment options for patients with ARDS. These suggest that VT < 8 ml/kg IBW, plateau pressures < 30 cmH2O and prone positioning have significant positive impact on patient with ARDS. However, the exact impact of ventilator strategies like PEEP/FiO2 ratio and mandatory vs. supported ventilation are yet to be re-examined. With the regional project of improving LPV in Wessex, we raised awareness of LPV. The future in ARDS treatment lies in the early recognition of ARDS, which remains poor4 and the individualised treatment.
The impact of new ventilators with automated modes such as adoptive supportive ventilation (ASV) is yet to be established. ASV aims to deliver an effective alveolar ventilation while taking patient’s ideal body weight, maximal plateau pressure, desired minute ventilation, resistance, compliance and auto-PEEP into account. It should lead to an optimal ventilator pattern and reduce complications such as volutrauma or barotrauma and air trapping. 6
Conclusions
The regional study conducted by SPARC confirms the finding in literature. Adherence to LPV is variable across ICUs. The majority of patients fail to receive LPV which has shown to reduce mortality in patients with ARDS. 7 The documentation of other ventilator parameter like plateau pressure and PEEP is variable and further studies are required to establish factors contributing to outcome in patients with ARDS. The first step in improving outcome in ARDS is improving the awareness of ARDS to enable early recognition and treatment to optimise outcome.
By conducting a multidisciplinary survey in Wessex followed by auditing the current practice in ICUs in Wessex, awareness of ARDS has been improved. The re-audit after a year of quality improvement and education demonstrated an improvement of LPV and awareness of ARDS in the Wessex region.
Supplemental Material
Appendix -Supplemental material for From a small local audit to a regional quality improvement project – Improving lung protective ventilation
Supplemental material, Appendix for From a small local audit to a regional quality improvement project – Improving lung protective ventilation by Sarah Birkhoelzer, Matt Taylor, Ben Harris, Kayode Adeniji and on behalf of collaborators from the Southcoast Perioperative Audit and Research Collaboration (SPARC) in Journal of the Intensive Care Society
Footnotes
Author contributions
SB led both the initial regional survey as well as initiated and coordinated the re-audit in January 2016. SB recruited the contributors and organised the data collection and project management. MT recruited the contributors and contributing to the drafting of the manuscript. KA provided leadership for the project and contributed to the drafting of the manuscript. SPARC contributed to the data collection and organization of service improvement. All the above authors have read and approved the final manuscript.
Acknowledgements
SPARC wishes to thank all local data collectors and local leads: Emma Fitzgerald, Neil Richardson, Rebecca Fry, Russell Goodall, Sarah Bates, Ben Thomas, Sonya Daniel, Andy Burton, Phil Mcglone, Aidan Joyce, Fiona Linton, Alex Belcher, Claire Swarbruck, Joe Kinsella, Chris Schopflin, Ian Jenkins, Anthony Sheperdson, Andrew Nash, Chris Couzens, David Walker, Jonarthan Thevanayagam, Sarah Bury, Sam Goodhand, Dale Duncombe, Nick Daines, Dom Melville, Benjamin Harris.
This study was presented in part at the European Society of Intensive Care Medicine Annual Congress Berlin 2015, at the Research and Audit Federation of Trainees (RAFT) at Group of Anaesthetists in Training (GAT) Annual Scientific Meeting in Nottingham in June 2016 and the Wessex Intensive Care Society Summer Meeting in Winchester 2016. RAFT is a network of regional groups of Anaesthetic Trainee Research Groups like the Southcoast Audit and Research Collaboration (SPARC) in Wessex.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.