
Abstract
Purpose
To identify variables associated with 24-h mortality after inter-hospital transfer.
Materials and methods
Single center retrospective study of adult patients transferred to a tertiary care medical ICU between 1 January 2010 and 15 April 2014. Demographic, clinical, physiologic, and laboratory data were collected. The Lasso method was used for logistic regression to identify predictors of 24-h mortality after inter-hospital ICU transfer.
Results
We identified 773 patients. Median age was 58 years (IQR 45–69), 49% were female, 83% Caucasian, and 48% had Medicare. The median length of stay at the transferring facility was 1.0 day (IQR 0–2). Median SOFA score on the day of ICU transfer was 5 (IQR 2–8). Twenty-two (3%) died within 24 h after inter-hospital transfer. SOFA score of 12–16 the day of inter-hospital transfer (odds ratio (OR) 7.77, 95% CI 1.21–66.26, p = 0.037), FiO2 0.8–1.0 on ICU arrival, and cardiac arrest prior to transfer (OR 4.94, 95% CI 1.43–15.96, p = 0.009) were associated with an increased risk for 24-h mortality after inter-hospital transfer.
Conclusions
Our study identified biologically plausible and potentially modifiable factors associated with 24-h mortality after inter-hospital medical ICU transfer, which may serve to inform patients and families of readiness and risk for mortality after inter-hospital transfer.
Introduction
Approximately 50,000 intensive care unit (ICU) admissions per year in the US are inter-hospital transfers, accounting for 4.5% of all ICU admissions. 1 Commonly cited reasons for transfer include ICU bed shortages at the transferring facility, provision of specialized services at the accepting facility, patient complexity and patient or family preference. 1 Transfers usually occur to either a tertiary care facility or one capable of providing a higher level of care.
Critically ill patients are at increased risk of morbidity and mortality during transport. 2 In-hospital mortality among transferred ICU patients is higher than direct admissions from the emergency room.3–5 Clough et al. 3 demonstrated that transferred patients to a tertiary care center have a 2.7-fold increased risk of dying in the hospital and contributed to 29% of deaths despite accounting for 10% of admissions, as compared to non-transferred patients. In a single center study, Ligtenberg et al. 6 demonstrated that 6% of patients died within the first 24 h after inter-hospital transfer. While numerous studies have evaluated factors predictive of overall ICU mortality, there have been no studies that specifically address risk factors in patients who are transferred from one hospital to another. The primary objective of this study is to identify factors which increase the risk for mortality within 24 h after inter-hospital transfer.
Methods
Setting
Froedtert and Medical College of Wisconsin Hospital is a 536 bed tertiary care academic medical center that primarily serves a large metropolitan area in southeastern Wisconsin and functions as a referral center for Wisconsin and northern Illinois. From a pool of approximately 350 referral centers, more than 200 critically ill patients are transferred to the Froedtert medical ICU each year. Transferring locations include emergency departments (EDs) and ICUs. The medical ICU at Froedtert Hospital is a 26-bed closed unit staffed by board certified academic medical intensivists and is separate from the institution’s surgical, cardiac, neurological, and transplant ICUs.
Study design
We performed an institutional review board (PRO00022374) approved single-center retrospective study of a prospectively maintained database. We included patients equal to or greater than 18 years old who were transferred to the Froedtert medical ICU from an outside hospital between 1 January 2010 and 15 April 2014. We excluded patients who were initially accepted for transfer but were not physically transferred to the Froedtert medical ICU.
Identification of patients
The Froedtert access center is the point of contact for all inter-hospital transfers. Patients were identified using the access center’s prospectively maintained database. All patients transferred to the Froedtert medical ICU between 1 January 2010 and 15 April 2014 were divided into two groups: those transferred who died within 24 h of arrival to the medical ICU and those who survived greater than 24 hours after arrival to the medical ICU.
Data collection
Data were independently reviewed and extracted from the electronic health record. Study team members received training to ensure fidelity and consistency with data extraction. Demographic, clinical, physiologic, and laboratory variables were extracted. Demographic variables such as age, gender, race, insurance status, and mode of transfer were collected. For example, clinical variables included primary reason for inter-hospital transfer and sequential organ failure assessment (SOFA) on the day of transfer. Physiologic variables included admission mean arterial pressure (MAP), heart rate, and oxygenation status for incorporation into severity of illness scores. Laboratory variables included admission creatinine, hemoglobin, and lactic acid.
Statistical analysis
The primary objective of this study is to identify factors which increase the risk for mortality within 24 h after inter-hospital transfer. The secondary objective is to identify factors which increase the risk for in-hospital mortality after inter-hospital transfer.
Baseline covariates were summarized by the mean, standard deviation, median and range for continuous variables and frequency and percentage for categorical variables. Variables with 10 or greater missing data points were reported. For each outcome (24-h mortality and in-hospital mortality), univariate analysis was performed using Wilcoxon rank-sum tests for continuous predictors and Fisher’s exact tests for categorical predictors. A multiple logistic regression prediction model was developed using the Lasso (least absolute shrinkage and selection operator) method for variable selection. All demographic variables, pre-transfer/transfer variables, and other measurements upon arrival were considered for the prediction model. Receiver operating characteristic (ROC) curves were generated to visualize model performance; the area under the curve (AUC) was calculated as a measure of predictive ability. A predictive nomogram was generated for each model to serve as a practical tool for predicting the probability of mortality for an individual patient. All statistical analyses were performed using R version 3.3.1 (R Foundation for Statistical Computing, http://www.R-project.org). All p-values (p) were two-sided and a p of less than 0.05 was considered statistically significant.
Results
Demographic and clinical variables
Between 1 January 2010 and 15 April 2014, there were 793 requests for transfer to our medical ICU. Of these, 16 were cancelled by the referring facility and four were denied. Seven-hundred and seventy-three patients were transferred to our medical ICU. Median age was 58 years (interquartile range (IQR) 45–69), 49% were female, 83% Caucasian, and 48% had Medicare. The median length of stay at the transferring facility was 1.0 days (IQR 0–2). Seventy-five percent of patients were transferred >20 miles. Median SOFA score on the day of ICU transfer was 5 (IQR) 2–8). Twenty-two of 773 (3%) died within 24 h of arriving to the medical ICU. One-hundred and eighteen of 773 (15%) died during the same hospital admission. Median ICU-free days (out of 30) were 27 (IQR 20–28).
Demographic, clinical, and outcomes characteristics.
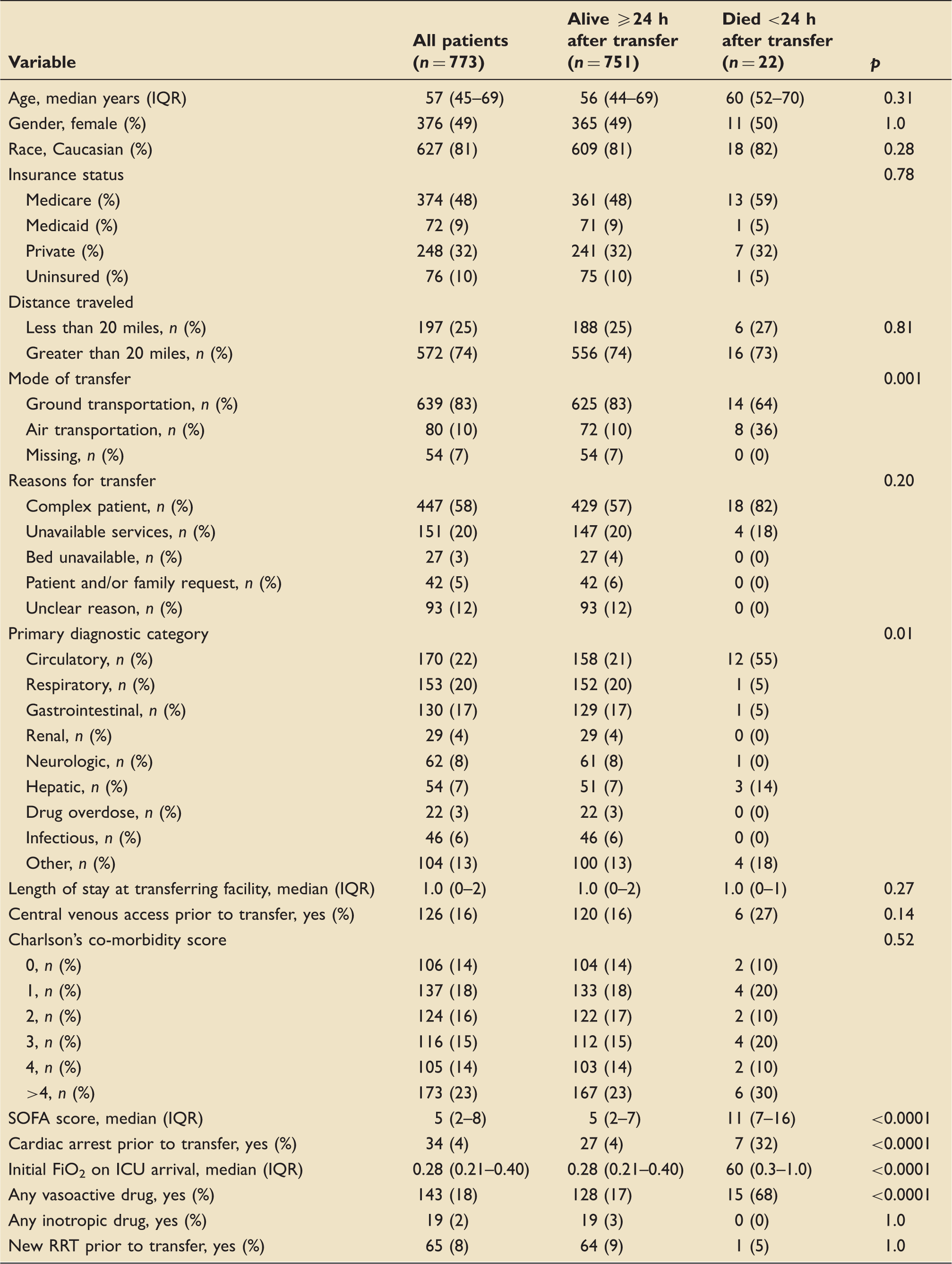
FiO2: fraction of inspired oxygen; ICU: intensive care unit; IQR: interquartile range; RRT: renal replacement therapy; SOFA: sequential failure organ assessment.
Primary outcome
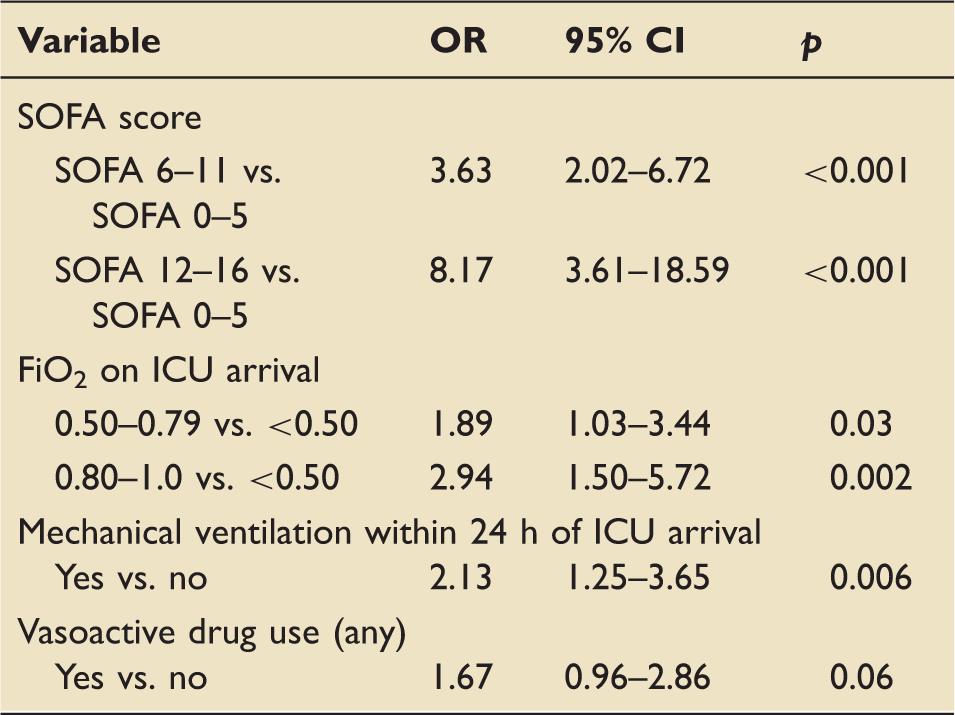
Multivariate logistic regression of factors independently associated with mortality within 24 h after inter-hospital transfer (n = 741).
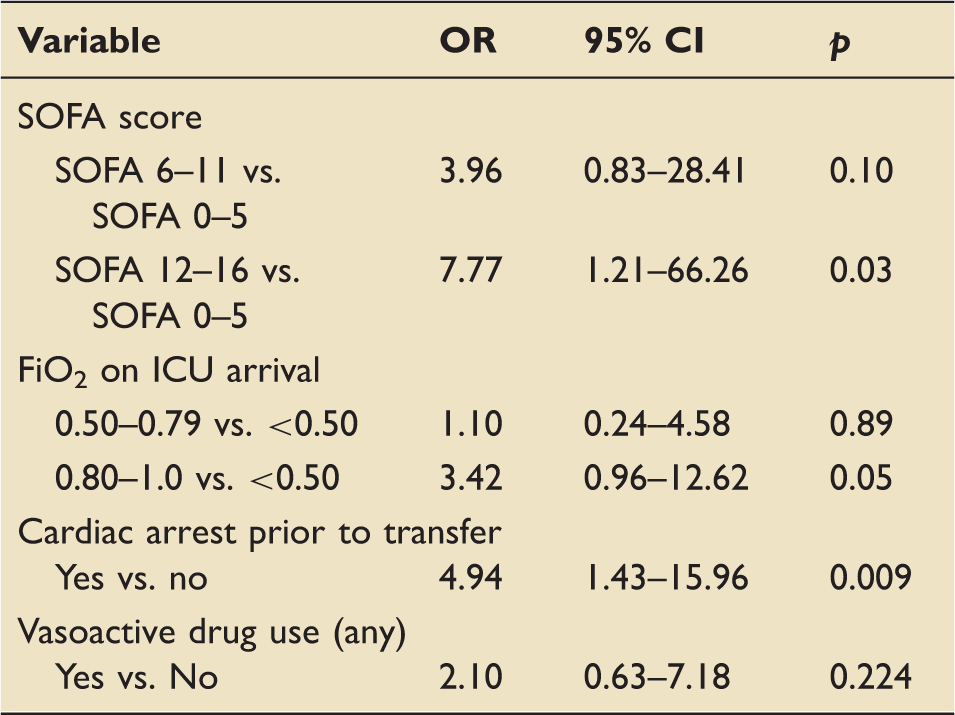
CI: confidence interval; FiO2: fraction of inspired oxygen; ICU: intensive care unit; OR: odds ratio; SOFA: sequential organ failure assessment.
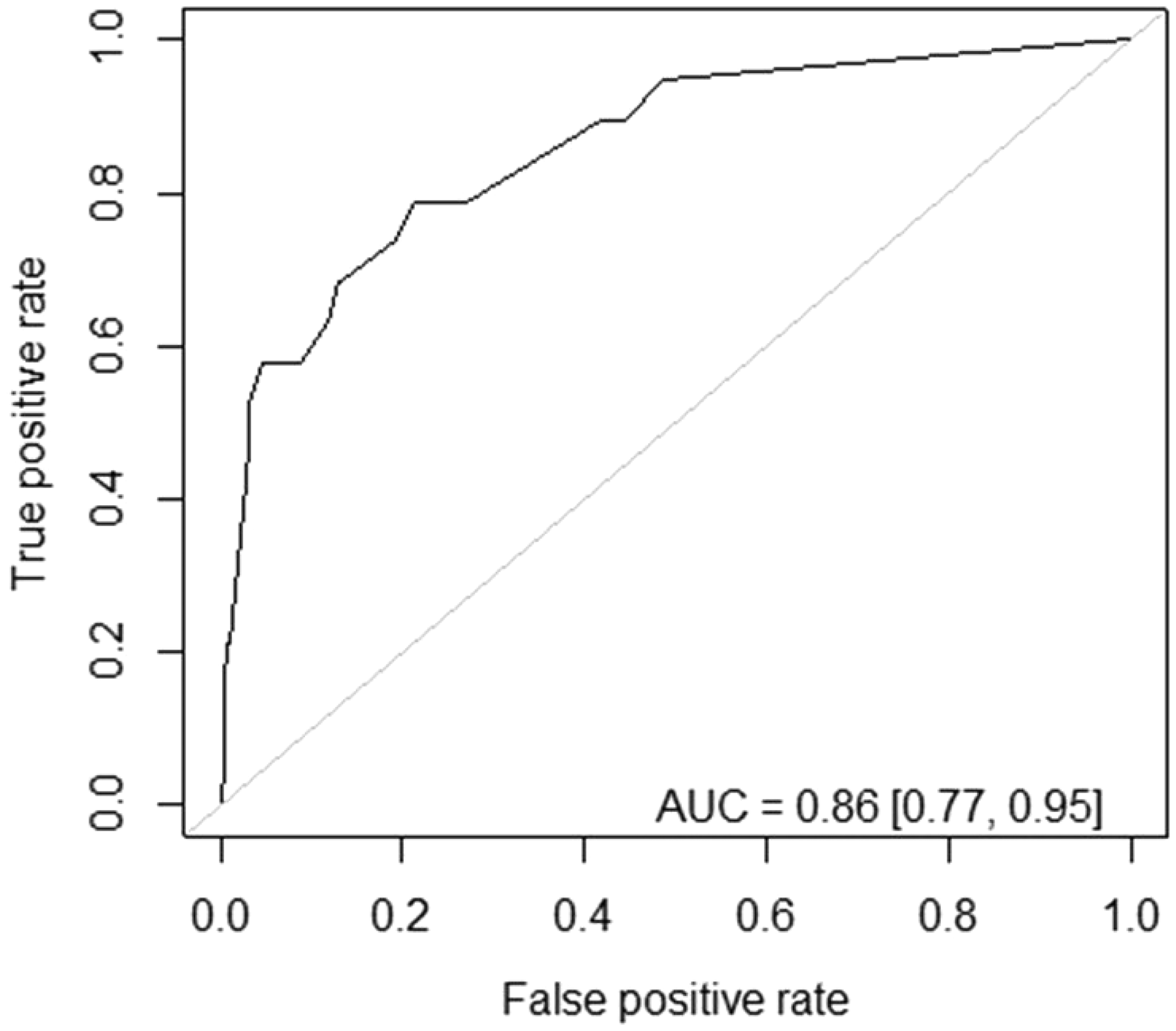
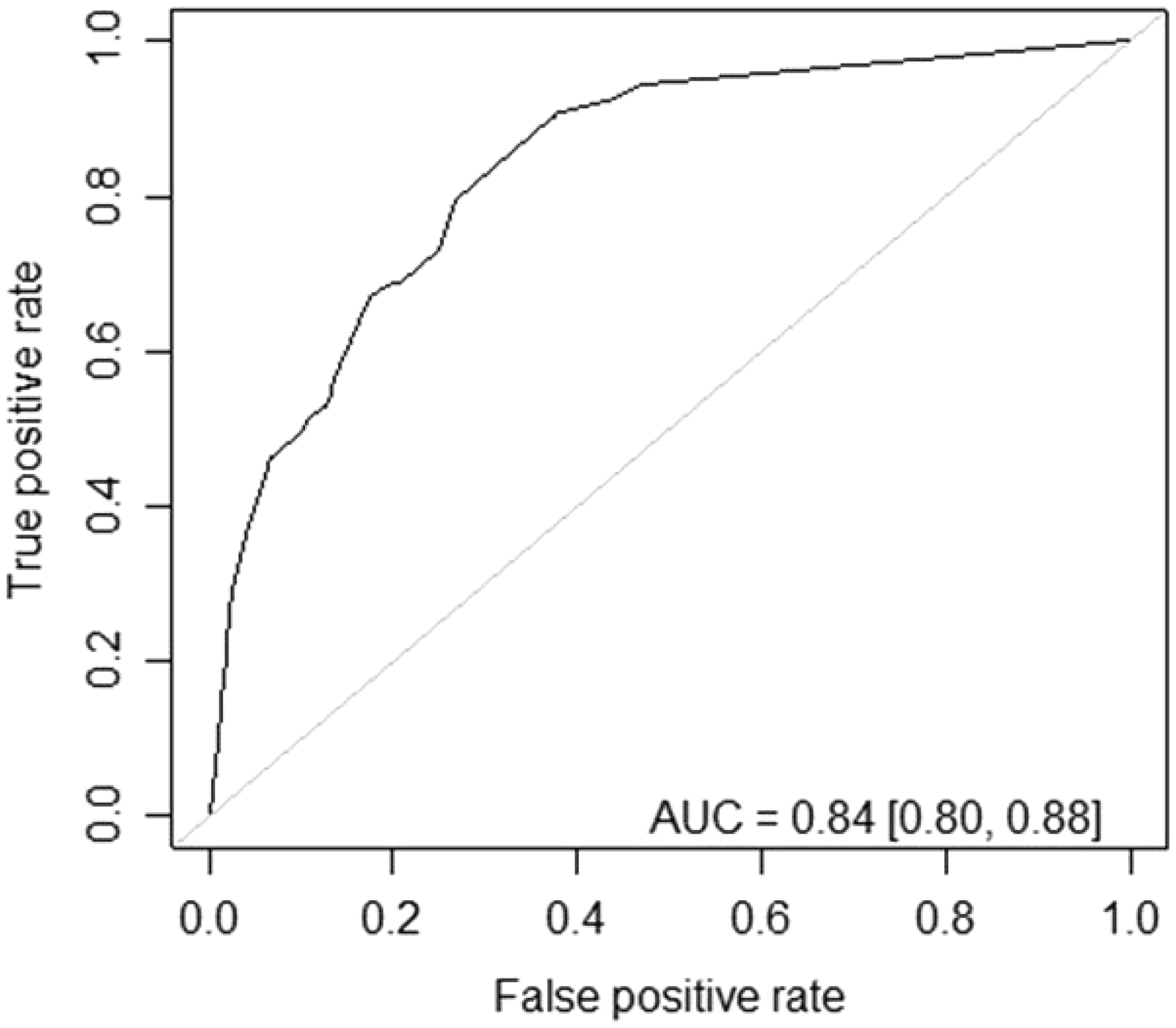
The receiver operating characteristic (ROC) curve shows the true positive rate (y-axis) and false positive rate (x-axis) for each threshold of the predicted probability of mortality within 24 h after inter-hospital transfer from the multiple logistic regression model. The area under the curve (AUC) is provided as a measure of model performance. For reference, an AUC of 1 is perfect prediction and an AUC of 0.5 means our model is no better than random guessing.
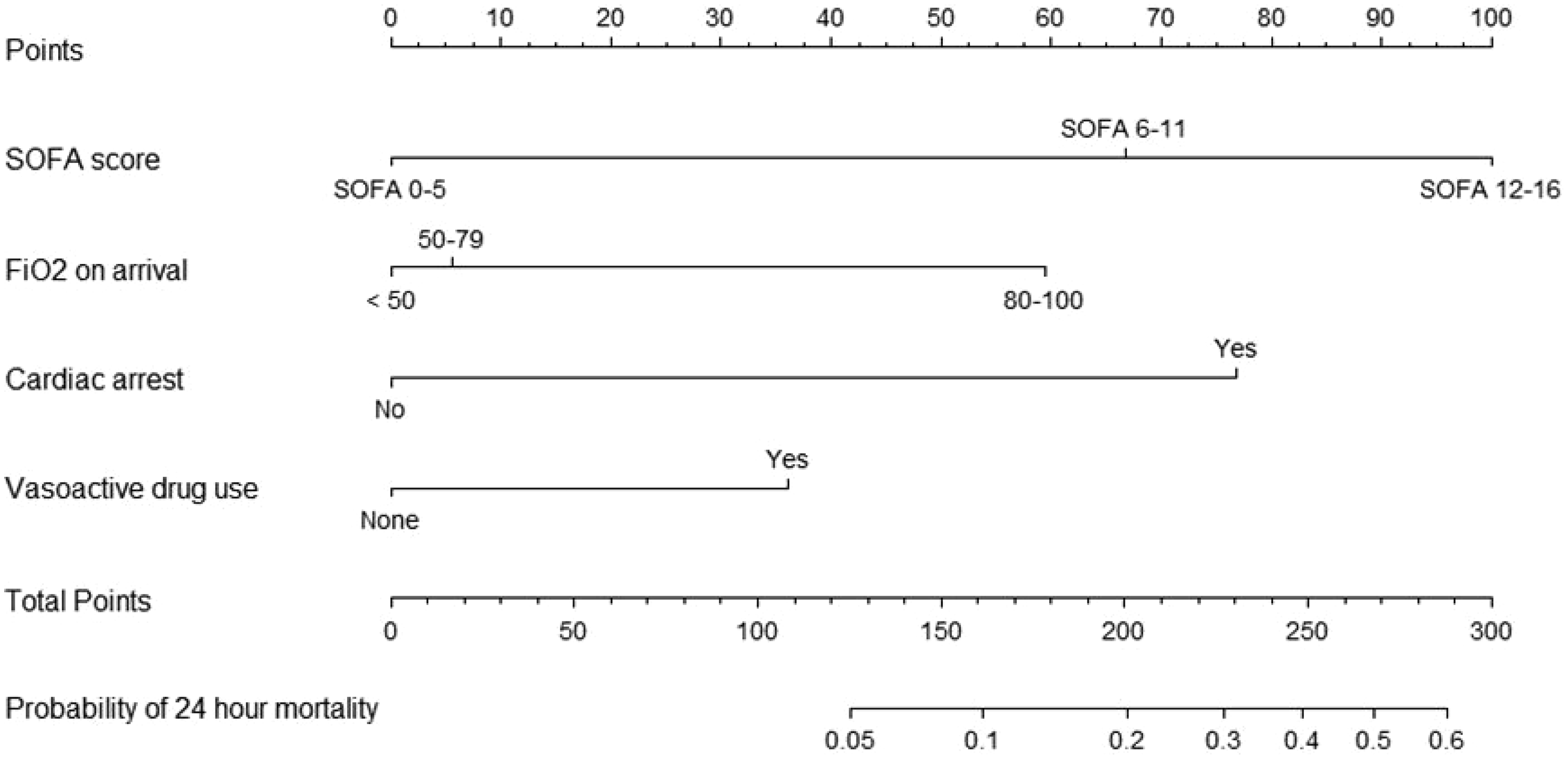
A nomogram for 24-h mortality after inter-hospital ICU transfer. The nomogram is a graphical tool, which simplifies manual calculation of the predicted probability of mortality from the multiple logistic regression model. The top row shows the reference point-scale for individual predictors in the model. A total score is calculated by taking the sum of all individual predictor points. The predicted probability is linked to the total point score using the scale at the bottom.
Secondary outcome
Multivariate logistic regression of factors independently associated with in-hospital mortality (n = 741).
CI: confidence interval; FiO2: fraction of inspired oxygen; ICU: intensive care unit; OR: odds ratio; SOFA: sequential organ failure assessment.
The receiver operating characteristic (ROC) curve shows the true positive rate (y-axis) and false positive rate (x-axis) for each threshold of the predicted probability of in-hospital mortality after inter-hospital transfer from the multiple logistic regression model. The area under the curve (AUC) is provided as a measure of model performance. For reference, an AUC of 1 is perfect prediction and an AUC of 0.5 means our model is no better than random guessing.
Discussion
This single center retrospective study identifies predictors of 24-h and in-hospital mortality after inter-hospital medical ICU transfer. Independent predictors of 24-h mortality after inter-hospital transfer include SOFA score 12–16, FiO2 0.8–1.0 on ICU arrival, and cardiac arrest prior to inter-hospital transfer. There were similar predictors for both 24-h mortality and overall in-hospital mortality, including SOFA score 12-16 the day of transfer and FiO2 0.8–1.0 on ICU arrival.
In our study, “complex patient” and “unavailability of services” were the most common indications for inter-hospital transfer. Transfer for these reasons is intended to improve patient prognosis. 1 In fact, previous studies have evaluated patient-based and systems-based predictors of poor outcome after inter-hospital transfer.3,7–10 Durairaj et al. 7 identified male gender, summer season, admitting service, diagnostic related group level, Charlson co-morbidity score, insurance type and major diagnostic category as predictors of early mortality, defined as <72 h, after inter-hospital medical ICU transfer. The biologic plausibility of the identified risk factors, including male gender, summer season, and admitting service, predicting mortality at 72-h is not apparent and the factors are not modifiable. Furthermore, the Charlson’s co-morbidity score takes into account pre-existing comorbidities and not the acuity of illness warranting transfer. 11 In our study, there was no significant difference in Charlson’s co-morbidity score between those who died within 24 h after inter-hospital transfer and those who survived (p = 0.52). We identified modifiable variables defining severity of acute illness, such as SOFA, FiO2, and cardiac arrest prior to transfer, which may be more biologically plausible than Charlson’s co-morbidity score in explaining the associated poorer outcome within a narrower timeframe. Post-transfer variables associated with 72-h mortality were not identified in the Durairaj study. In a retrospective study of 100 consecutively transferred ICU patients, 6 of 100 (6%) died within the first 24 h after inter-hospital transfer. 6 In this study, there were no differences in arrival vital signs between those who died within 24 h after inter-hospital transfer and those who survived. Similarly, in our study, there was no significant difference in ICU arrival heart rate, MAP, or respiratory rate in those who died within 24 h as compared to those who survived. However, patients who died within 24 h after inter-hospital transfer had a significantly lower temperature on arrival (median 36.4℃ (IQR 35.9–36.8°F) vs. 36.8℃ (IQR 36.6–37.2℃), p = 0.001) and greater arrival FiO2 requirements (median 0.60 vs. 0.28, p < 0.001). Furthermore, our study identified the need for mechanical ventilation within 24 h after arrival as an independent predictor of in-hospital mortality.
The mode of travel, distance traveled, and general transfer process may pose a risk of harm to the critically ill patient. Single-center studies have identified preventable errors during inter-hospital ICU transfer in up to 70% of cases, which may be related to traveling longer distances.6,7 Our study did not find distance traveled to be a predictor of 24-h mortality after inter-hospital transfer. Instead, our study identified air transportation to be a univariate predictor of 24-h and in-hospital mortality after inter-hospital ICU transfer. The median SOFA score of air transported patients in our study was 7 (IQR 7), as compared to 4 (IQR 5) for ground transported patients (p < 0.001), suggesting sicker patients may be more likely to be air transported.
Our study has several limitations. First, outcomes are reported from a single-center medical ICU in a tertiary care academic care center, limiting the study’s external generalizability. However, we identify factors present at multiple outside hospitals and transport systems. Second, despite using validated methods to identify risk factors for mortality, the retrospective nature of our study subjects it to unmeasured confounding. We remained internally consistent in identifying overlapping predictors of 24-h and overall in-hospital mortality. Third, we were unable to determine whether referring hospital or peri-transfer variables, such as availability of resources or complications during transfer, impacted post-transfer mortality. Fourth, the CIs for predictors of 24-hour mortality were wide, likely due in part to the low number of patients (22/773) who died within 24 h after inter-hospital transfer. Fifth, limitations of the statistical methods include the use of automated model selection procedures which compare multiple candidate models to select the final prediction model. Our results were not corrected for multiple testing associated with this procedure. Stepwise selection is also subject to overfitting and problems with collinearity between predictors. To address this, we used a model selection procedure, LASSO (elastic net variation), which performs better in these areas. Due to the limited frequency of events, we were unable to split the dataset into a testing and training for model development and evaluation. Future validation of the predictive nomogram is warranted in a separate cohort. Lastly, studies have demonstrated ED-to-ICU transfer was associated with significantly better outcomes, as compared to ICU-to-ICU transfer.9,10 Patient location was not reported in our study and it is unclear whether an ED-to-ICU or an ICU-to-ICU transfer impacted 24-h mortality in our cohort. Despite this limitation, our findings can be applied to either setting to identify which patients are at-risk of 24-h mortality.
Conclusion
Our study sheds light on biologically plausible and potentially modifiable variables associated with 24-h mortality after inter-hospital medical ICU transfer. Identifying variables associated with 24-h mortality is important for several reasons. First, examining mortality at 24-h identifies risk factors in a potentially vulnerable population that may not benefit from inter-hospital transfer, and instead, may be harmed by the potential complications and expense of transfer. Knowledge of the risk factors within the framework of our proposed nomogram risk stratifies patients for referring hospitals and accepting providers before considering inter-hospital transfer. Second, patients and families can be informed of their risk for mortality after inter-hospital transfer to guide shared-decision making on appropriateness and readiness of transfer. Third, the organ dysfunctions which summate into a SOFA score are potentially modifiable. It is unclear if optimizing therapies prior to transfer reduces the risk of mortality after inter-hospital transfer. Finally, the Emergency Medical Treatment & Labor Act (EMTALA) of 1986 regulates which patients should be accepted, refused, and/or re-assessed for transfer. 12 Pending validation, our proposed nomogram can serve as a dynamic research tool to inform changes to EMTALA regulations and inter-hospital transfer guidelines. 2 Further studies evaluating the validity of our findings are needed.
Footnotes
Acknowledgements
The authors would like to thank Dr. Elizabeth Jacobs for her thoughtful review of the manuscript.
Authors’ contributions
JJP had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. JJP contributed to study design, data analysis, interpretation, and writing the manuscript. JSK, KT, and SM contributed to data acquisition, analysis, and writing of the manuscript. LR, AS, and SQS contributed to data analysis and writing of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the National Center for Advancing Translational Sciences, National Institutes of Health, through Grant Number UL1TR001436. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH.