
Abstract
Ocular surface disease is common in the intensive care population with 20–42% of patients developing corneal epithelial defects. The ocular surface is normally protected by the ability to produce tears, to blink and to close the eyes with rest or sleep. All of these mechanisms can be disrupted in the intensive care population, increasing the risk of developing ocular surface disease. Despite the scale of the problem, eye-care protocols are commonly not instigated and documentation of eye care is often poor. This review details the risk factors for developing ocular surface disease. It also provides evidence-based guidance on protecting the eyes in vulnerable patients, identifying diseases affecting the eye in intensive care patients and delivering the best treatment to the eye. There is growing evidence that adherence to a correctly performed eye-care guideline prevents the majority of corneal problems encountered in the intensive care unit.
Introduction
Eye care is an important aspect of managing the critically ill patient, as many of the mechanisms normally involved in protecting the eye from infection and injury are compromised. The ocular surface comprises the sclera, an avascular cornea and conjunctival epithelium. Ocular surface disease (OSD) can involve any of these structures and can present as:
Direct injury to the cornea – most often a superficial corneal abrasion (scratch) Exposure keratopathy Chemosis (conjunctival swelling) Microbial conjunctivitis and keratitis
The development of OSD among intensive care unit (ICU) patients is common, affecting 23–60% of patients.
1
ICU eye care protocols are sometimes haphazardly followed, and documentation of eye care is often poor. However, having a clear protocol for assessment and intervention, which is applied rigorously and correctly, will prevent the majority of corneal problems.2,3
This document aims to provide advice and information for clinical staff who are involved in eye care in the ICU. It is primarily intended to help non-ophthalmic ICU staff to:
Protect the eye in vulnerable patients, thus preventing ICU-related eye problems Identify disease affecting the eye in ICU patients, and specifically those which might need ophthalmic referral Deliver treatment to the eye when it is prescribed
It concentrates primarily on the common problems of the eye surface but also touches on other less common conditions. As such, it should also be helpful to those ophthalmologists asked for advice about ICU patients. These guidelines have been reviewed and supported by the Joint Standards Committee of the Intensive Care Society (ICS) and Faculty of Intensive Care Medicine (FICM).
Risk factors
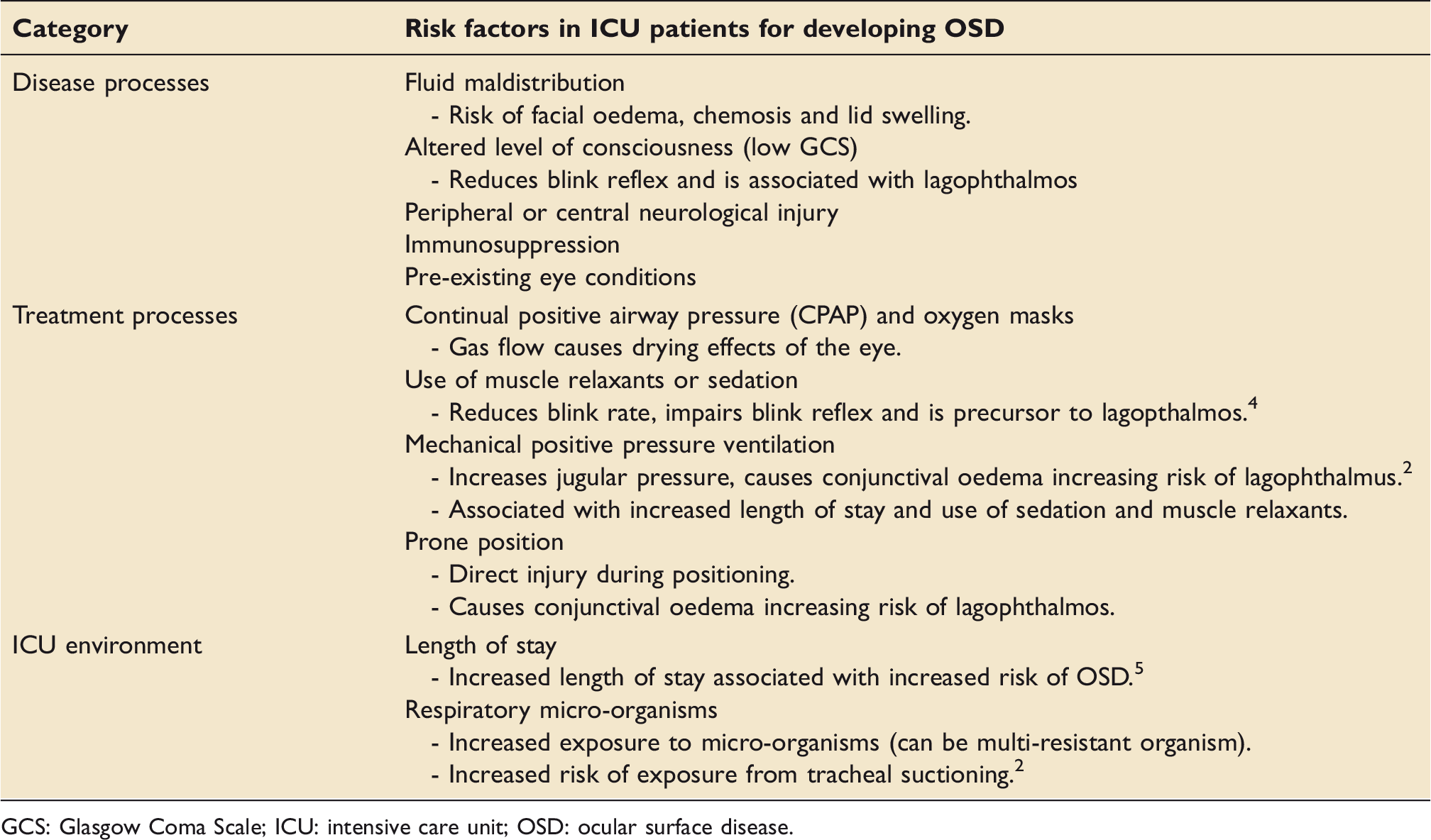
The health of the front surface of the eye, particularly the cornea (the clear front window of the eye), depends on the ability to produce tears, to blink and to close the eyes with rest or sleep. Incomplete eyelid closure is called lagophthalmos. All of these mechanisms can be impaired in patients in ICU by disease (e.g. facial oedema, reduced conscious level, peripheral or central neurological injury) or treatments (e.g. the drying effects of gas flows from CPAP or oxygen masks). In particular, muscle relaxants reduce the tonic contraction of the orbicularis muscle around the eye, which normally keeps the lids closed, and sedation reduces blink rate and impairs (and can eliminate) the blink reflex. Whatever the cause, those unable to close the eye for themselves, or in whom blinking rates are substantially reduced, are at increased risk of damage to the front of the eye. This risk is higher in those mechanically ventilated, due to greater length of stay, use of sedative/paralysing drugs and the effects of positive pressure ventilation. These risk factors are summarised in Table 1.
Protecting the eye of the vulnerable patient
Assessment: Identifying those at greatest risk of OSD
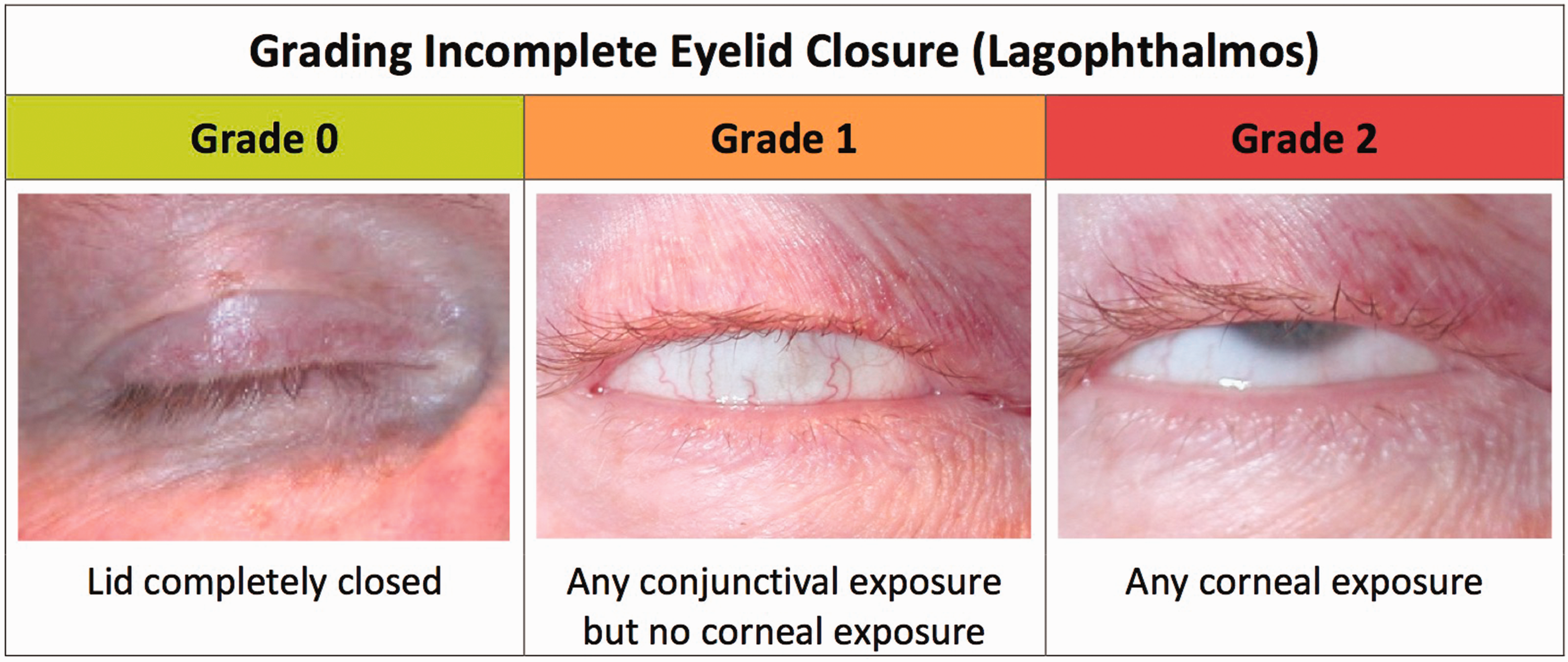
Assessment of eyelid closure must be done at the onset of the care plan, and then regularly throughout the patient’s stay. There is a strong correlation between lagophthalmos and the development of corneal erosion, which can then lead to keratitis or corneal ulceration. 4 The main aim of this assessment is to grade the severity of lagophthalmos from zero to two.
Protective measures
A variety of methods can be used to protect the eyes of ICU patients. These include:
Manual closure of the eyes or taping the eyes shut. Lid taping is not always necessary and can be distressing to relatives, and repeated removal may lead to some degree of facial skin or eyelid injury or irritation. It should therefore only be undertaken when definitely necessary. Liberal use of lubricants into the eye: ointment (such as simple eye ointment, Lacrilube™ and VitA-POS™) is recommended as drops do not last long enough. This needs to be applied correctly into the eye as demonstrated in Figure 2. Such action is superior to manual eye closure alone and to the (once prevalent) application of Geliperm™.
5
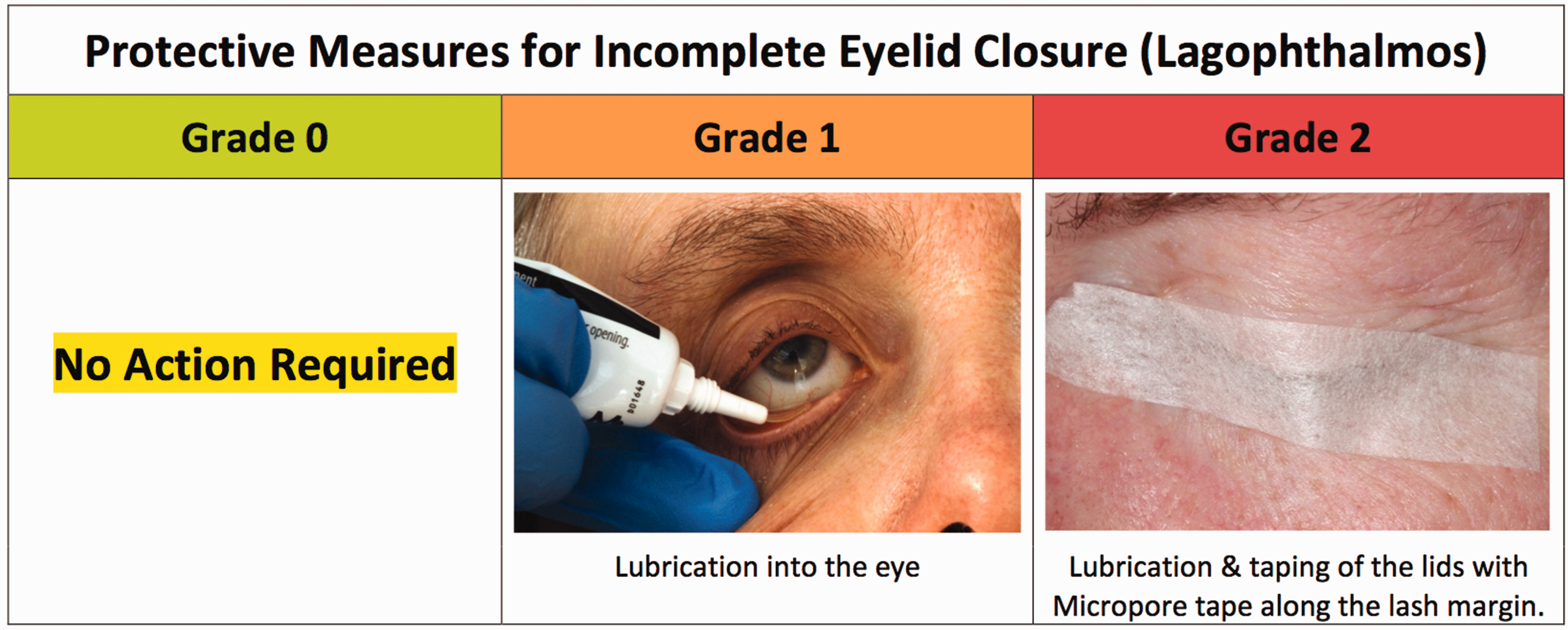
The action required is based on the grading of lagophthalmos (see Figures 1 and 2):
Grade 0 exposure (i.e. no exposure) requires no action. Grade 1 exposure requires lubrication Grade 2 exposure needs lubrication and taping of the lids with Micropore tape along the lash margin. Schematic showing the different grades of lagophthalmos. Schematic demonstrating action required depending on degree of lagophthalmos identified.
Eyes should be bathed with warm water first to remove dried ointment. Before the next lubricant application, the eye should be examined with a bright light to look for redness, areas of chemosis or corneal dullness or opacity. If these are found, the medical staff should be alerted (and consideration of referral for ophthalmological opinion given) and considerably increased lubrication given. New ointment is applied to the eye surface: pull the lower eyelid down with a finger and insert the ointment over the top of the lower lid into the gap between the lid and the conjunctiva every 4 h (see Figure 2). If taping is also performed, ointment is put in first and the eyes are closed.6–9 The position of the lashes is then checked as the lashes must be clear of the cornea if iatrogenic corneal abrasion is to be avoided. The outside of the eye must be free of the lubricant ointment for tape to stick properly. Micropore™ tape is then applied horizontally across the lids to seal them shut as demonstrated in Figure 2. Horizontal taping is recommended, but if vertical taping is used, care must be taken to ensure the eye remains shut and is not open where there is no tape.
In those patients nursed prone, the eyelids and face can become oedematous and chemosis is common. As in all ventilated patients, exposure keratopathy (a drying of the corneal surface) can occur. 9 Direct eye compression can occur and can be avoided using a three-pin head holder as is used for prone spinal surgery. 10 The eyes should always be re-lubricated every 4 h and taped shut. Where there is severe oedema and the swollen conjunctiva prolapses through the closed eyelids, the medical staff should be contacted as the eyelids may need to be temporally closed with sutures.
Identifying diseases of the eye
Exposure keratopathy and corneal abrasion
The cornea can be accidentally injured and nearly always in ICU this is in the form of a corneal abrasion (a superficial scratch removing the surface epithelium) (see Figure 3). It will cause the eye to become red and is best seen using fluorescein dye eye drops and a blue light, where the epithelial defect glows bright yellow; a white light will also work but the injury is less obvious.
(a) Eye showing corneal abrasion without fluorescein. (b) Eye showing corneal abrasion stained with fluorescein under blue light.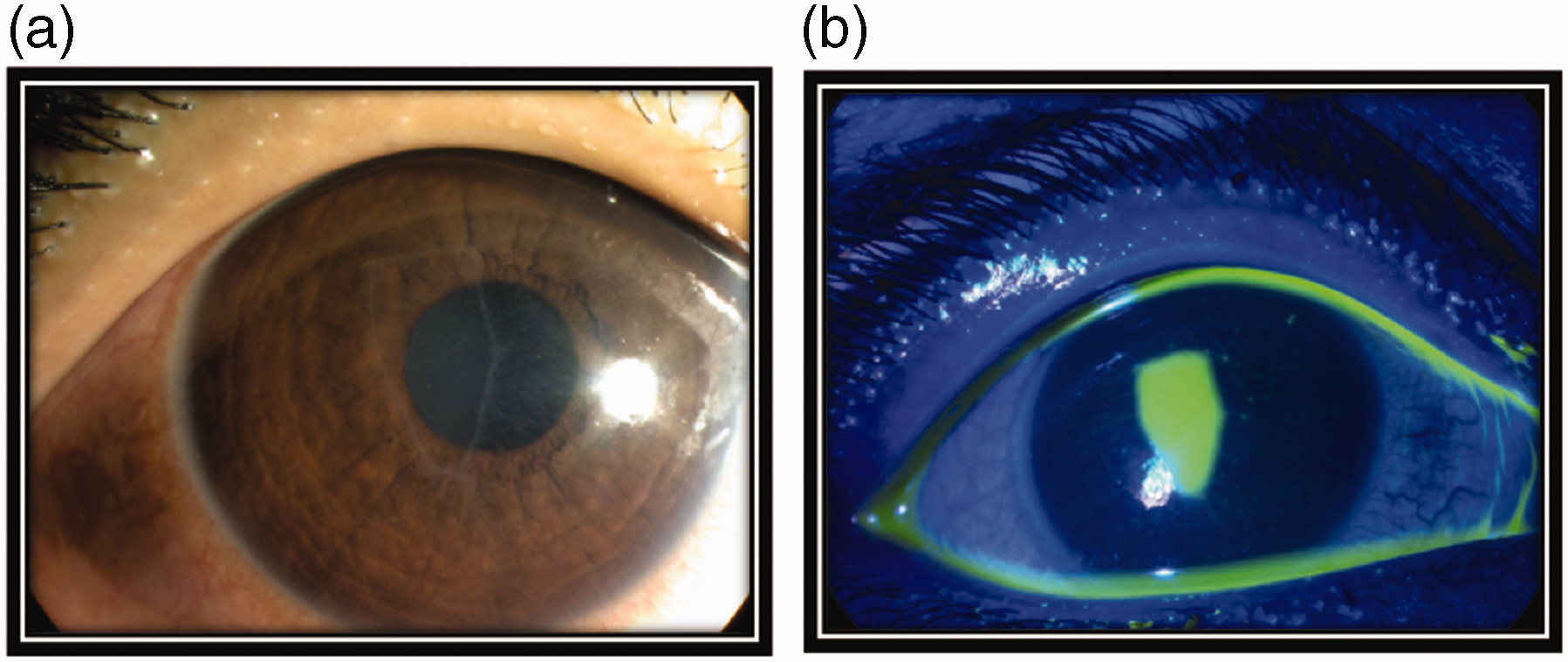
Exposure keratopathy represents a dryness of the cornea due to incomplete lid closure allowing excessive tear evaporation and a consequent failure of the tears to spread adequately across the eye surface. It manifests as a red eye, and fluorescein dye drops reveal smaller or larger epithelial defects which look identical to corneal abrasions. It affects 20–42% of ICU patients, 11 and 60% of those sedated for >48 h develop corneal epithelial defects (42% within the first week) as a result.12,13 Prolonged epithelial defects can cause scarring or even, in severe cases, perforation of the cornea. Secondary infection (microbial keratitis, see Figure 6) can occur.
Treatment of a simple corneal abrasion without secondary infection can be with chloramphenicol ointment four times daily for five to seven days, and increased lubrication and lid taping if there is significant unwanted corneal exposure.
Chemosis
Conjunctival oedema which causes the conjunctiva to bulge out (chemosis) is common in ICU patients (see Figure 4). Risk factors include compromised venous return from the ocular structures (positive pressure ventilation, escalating positive end expiratory pressures or tight endotracheal tube taping); those states associated with generalised oedema (such as fluid overload or hypalbuminaemia); gravitational causes of increased hydrostatic pressure (prolonged recumbency or prone ventilation); or states that increase capillary leak (such as systemic inflammatory response syndromes).
14
Chemosis can cause impaired eyelid closure, whilst incomplete eyelid closure can also predispose to chemosis.
Eye showing swollen conjunctiva (chemosis) (*).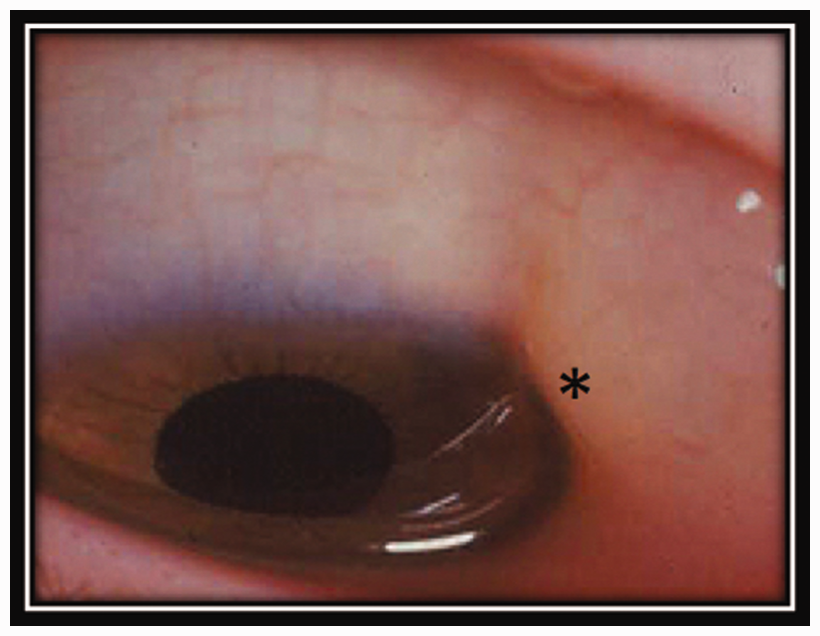
Microbial infections
The eye commonly becomes colonised with bacteria (in a time-dependent fashion) in ICU: as many as 77% of ventilated medical patients are colonised by at least one abnormal bacterial species in 7–42 days and multiple abnormal bacteria colonise up to 40% of those with prolonged ventilation and sedation. The most commonly isolated organisms are Pseudomonas aeruginosa, Acinetobacter spp. and Staphylococcus epidermidis. 15
Respiratory secretions are thought to be the major source of ocular surface infection, with aerosols from tracheal suctioning and direct contact from suction catheters both being implicated. Pseudomonas infection rates can thus be reduced if open endotracheal suctioning is done from the side (rather than head) of the patient and with their eyes covered.2,5,14
Conjunctivitis
ICU staff should look for a sticky eye, which is usually (but not always in ICU) red (see Figure 5). Note that if the eye is very red but not sticky, this might not be conjunctivitis and staff must seek expert ophthalmological help. Conjunctivitis in the ICU setting is usually bacterial and can be very infectious and virulent. Without due care it can be spread to other patients and staff.
(a) An eye that is red and sticky is most likely bacterial conjunctivitis. (b) An eye that is very red but not sticky might not be conjunctivitis, so seek an ophthalmology opinion.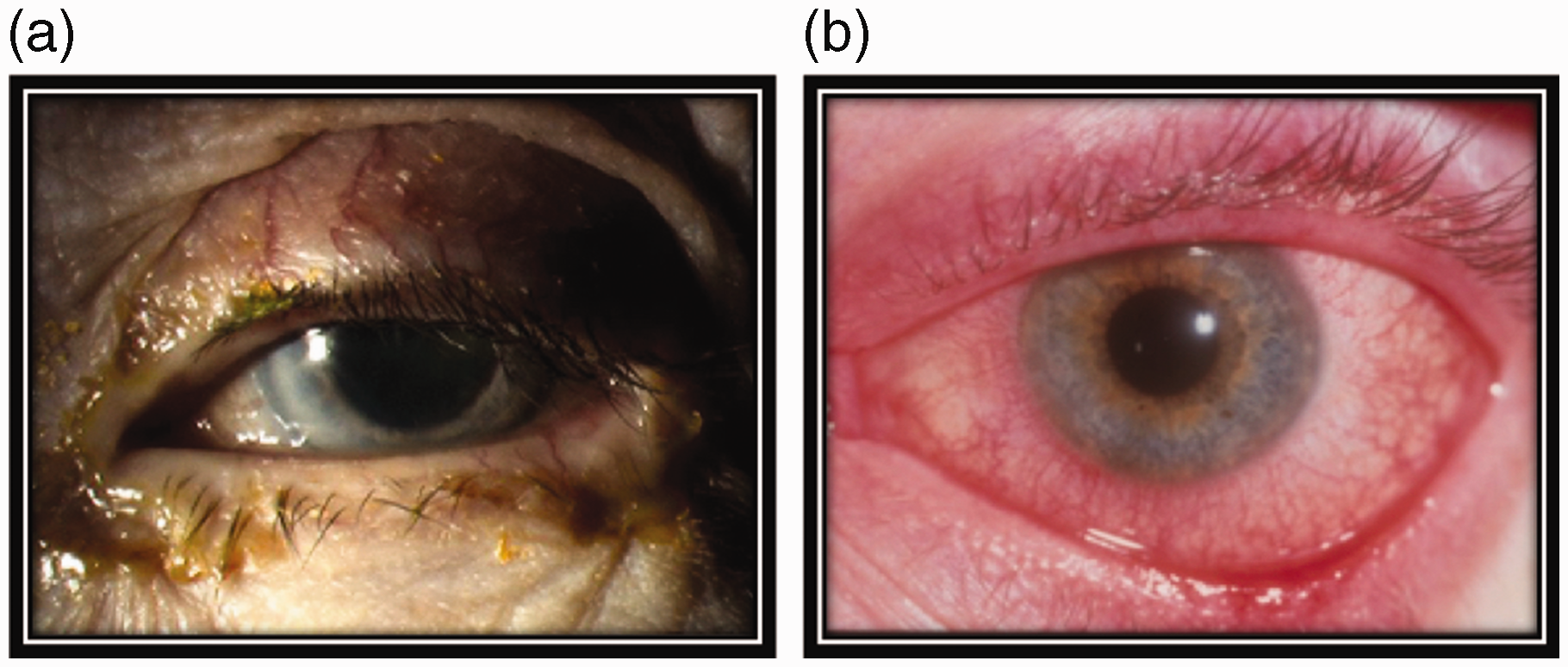
Management of conjunctivitis
It is wise to take a swab of the eye discharge and send it for microbial culture because of the increased possibility of infection with unusual organisms.
The discharge can be removed by bathing the eyelids with warm water, using separate gauze for each eye. Chloramphenicol ointment (rather than drops to utilise the continued good lubrication from the ointment) is applied in the eye four times a day for 5–7 days.
If the microbial results suggest that the organism is not sensitive to chloramphenicol, but the eye is better, leave alone and do not change this. If the eye is still sticky or red, then the ointment can be changed to one containing an antibiotic to which the organism is sensitive, or other antibiotic drops can be used in addition to simple lubricant ointment. If the discharge and redness have not markedly improved in 48 h, the medical staff must be informed, and ophthalmic help sought. If the cornea becomes dull or a white patch appears, an urgent ophthalmological opinion must be sought.
Microbial keratitis
The damaged cornea (for instance, that affected by exposure keratopathy) is especially vulnerable to bacterial invasion which can occur very rapidly (see Figure 6a). Whilst superficial infection can result, deeper infection can lead to permanent and severe damage, and loss of vision.
Most cases are due to bacteria and appear as a red eye, which may be watery or sticky, with a corneal ulcer (an epithelial defect – which stains with fluorescein dye on top of an underlying white/grey/yellowish opacity). Less commonly, debilitated patients may develop herpes simplex keratitis which takes the form of typical “dendrites” in the corneal epithelium and/or ulcers that stain yellow with fluorescein dye, but which can also appear as non-staining grey areas in the cornea (see Figure 6b). If any of these corneal problems are seen, urgent ophthalmic help must be sought.
(a) A red eye with a white patch on the cornea, this is likely microbial keratitis. (b) A red eye stained with fluorescein dye showing a dendrite on the cornea, this is likely Herpes Simplex keratitis.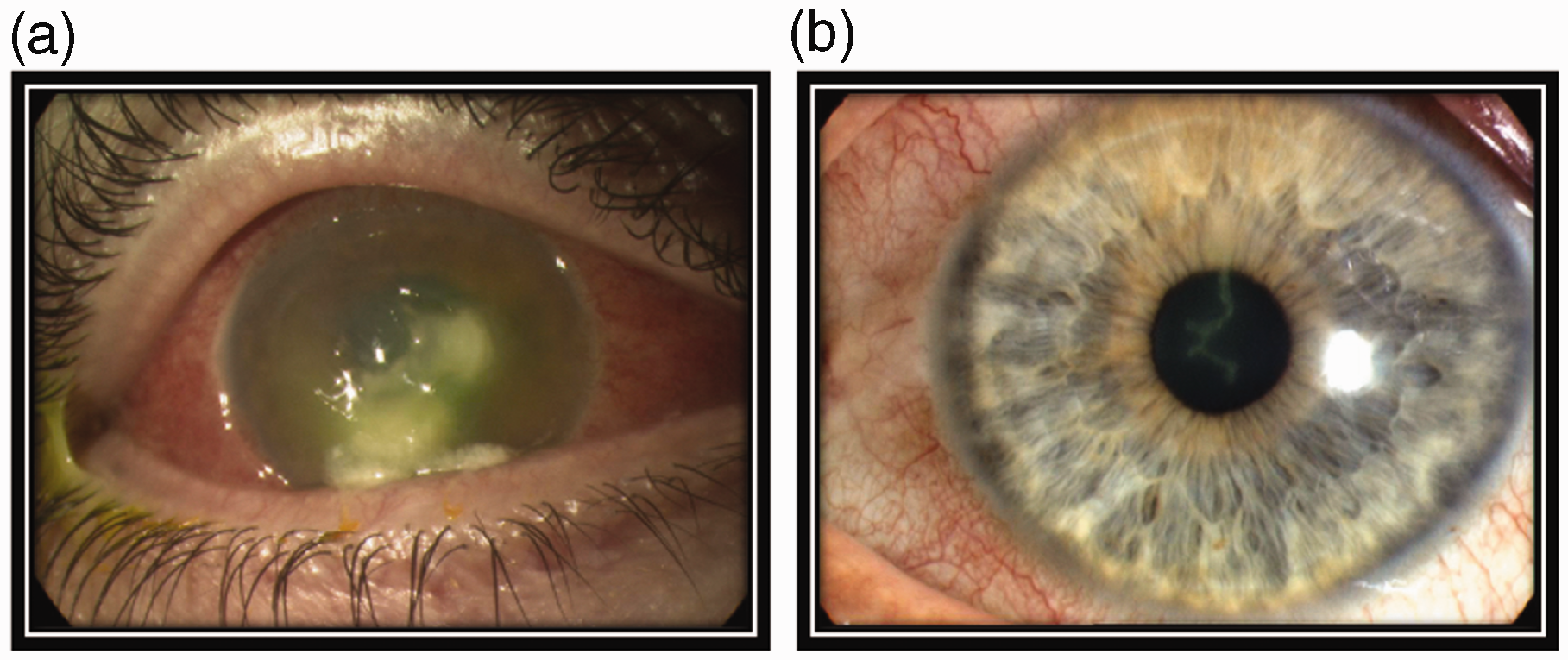
Rare eye conditions in ICU
Endogenous endophthalmitis
This is a very serious problem caused by spread of systemic infection in the blood stream to the inside of the eye. The eye may be red, although sometimes much less red than might be expected. Endophthalmitis is to be suspected if a white line is visible in the eye in front of the iris, which represents a level of pus in the anterior chamber of the eye (hypopyon, see Figure 7). Immediate ophthalmic help needs to be sought as this is a sight-threatening emergency and it also indicates systemic active sepsis.
An eye with a level of pus in the anterior chamber, this is called a hypopyon (↓). Suspect endogenous endophthalmitis and request immediate ophthalmology review.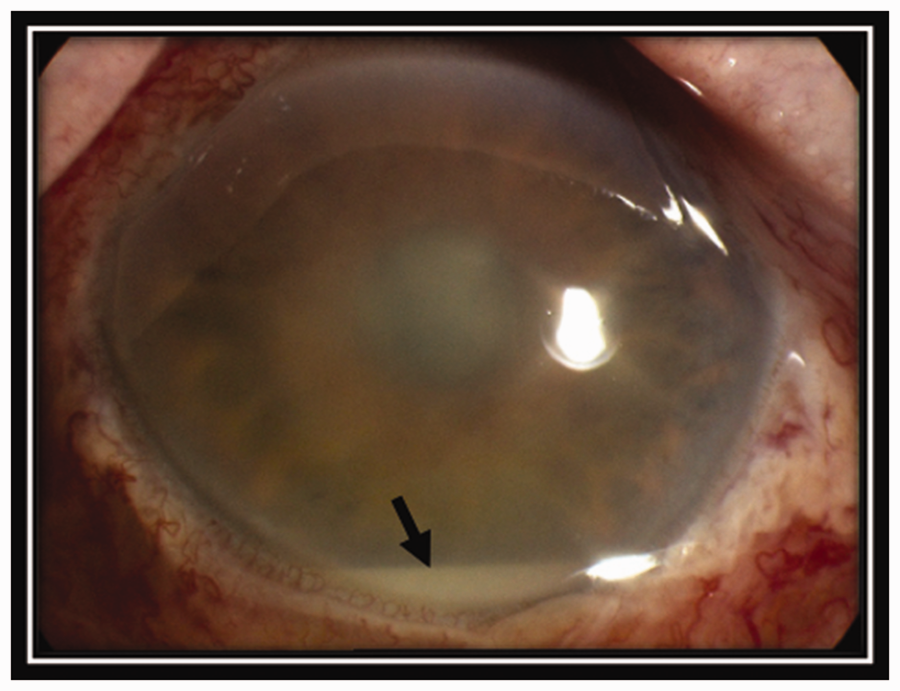
Other problems
Other eye problems can complicate ICU care. Severe or recurrent hypotension can cause blindness from ischaemic optic neuropathy.10,16 In those ventilated prone, increased intra-ocular pressures or intraorbital pressure with marked periocular swelling can decrease ocular perfusion pressures (worse with concurrent systemic hypotension), leading to ischaemic optic neuropathy, central retinal artery occlusion and permanent visual loss. 10
Rarely, those nursed prone can develop bilateral acute glaucoma in which there is a sudden rise in intraocular pressure which can cause visual loss very quickly as a result of retinal or optic nerve ischaemia. In this condition, the cornea becomes cloudy and grey and the pupil becomes fixed at a mid-dilated position and unresponsive to light. This needs immediate ophthalmic treatment.
Delivering treatment to the eye
This is usually given in the form of drops or ointment. Sometimes several different drops are required.
When giving several different drops, do not give them at the same time as one drop may wash out another, thereby reducing its effectiveness. Ideally, allow 5 min (and at least 1 min as a minimum) between each medication. Always put drops in before ointment. The ointment is water repellent and prevents the drops from getting into the eye tissues. When putting in ointment in poor lid closure, after instilling ointment manually shut eyelids to ensure ointment is spread over whole eye surface. Summary of common risk factors for OSD in ICU patients GCS: Glasgow Coma Scale; ICU: intensive care unit; OSD: ocular surface disease.
Supplemental Material
Appendix - Supplemental material for Eye care in the intensive care unit
Supplemental material, Appendix for Eye care in the intensive care unit by Benjamin J Hearne, Elewys G Hearne, Hugh Montgomery and Susan L Lightman in Journal of the Intensive Care Society
Footnotes
Consent
The authors confirm that consent has been given for the publication of images contained within this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Hugh Montgomery is partially funded by the National Institute for Health Research University College London Hospitals Biomedical Research Centre.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.