
Abstract
In Intensive Care Units (ICUs), patients are at risk of developing ocular complications, especially exposure keratopathy. Plan, Do, Study, Act for PDSA cycle. Despite national guidelines, implementation remains challenging. Using the PDSA cycle, we devised an eye care protocol integrated into the electronic patient record system, complemented by a poster summary of guidelines. An initial audit showed 2% adherence to eye exposure guidelines; post-intervention, adherence rose to 76%. A 9-month analysis revealed 16% of patients experienced eye exposure in ICU. This initiative emphasises the new protocol’s efficacy and the role of education in its adoption, advocating a more standardised approach to eye care in ICUs.
Keywords
Background
In Intensive Care Units (ICUs), eye health can be compromised due to factors such as excessive corneal dryness, incomplete eyelid closure and exposure to respiratory support. 1 Exposure keratopathy can affect over half of mechanically ventilated ICU patients, and between 20% and 42% may develop corneal defects which can lead to infections.2,3 Although national guidance for ICU eye care has been formulated by The Royal College of Ophthalmologists (RCOphth) and the Intensive Care Society, awareness and consistent implementation are lacking.4,5
The primary goal of this quality improvement initiative was to ensure standardised eye care according to national guidelines in an ICU. 4 Objectives include evaluating alignment with existing eye care practices and identifying impediments to adherence to these standards.
Methods
Overview
Our Intensive Care Unit (ICU) quality improvement initiative in eye care utilised the Plan, Do, Study, Act (PDSA) cycle. A multidisciplinary team formulated a driver diagram, delineating aims, primary and secondary drivers, and change ideas, to systematically address issues. A local eye care protocol, tailored to our context and grounded in national standards, was developed, drawing on existing literature for an innovative and evidence-based approach. 6 This protocol was communicated through visually engaging posters and digitally via a local ICU mobile app, ensuring accessibility and reinforcement of principles (Figure 1). Individual variables of the protocol were integrated into our electronic patient record system (EPR), Philips Intellispace Critical Care and Anaesthesia (ICCA), 7 streamlining data collection and adherence checks. Education played a central role. We developed an educational program explaining the protocol, the normal functioning of the eye, disruptions caused by ICU conditions and common ICU-related ocular conditions. The recorded sessions were integrated into the induction curriculum for new nursing staff.
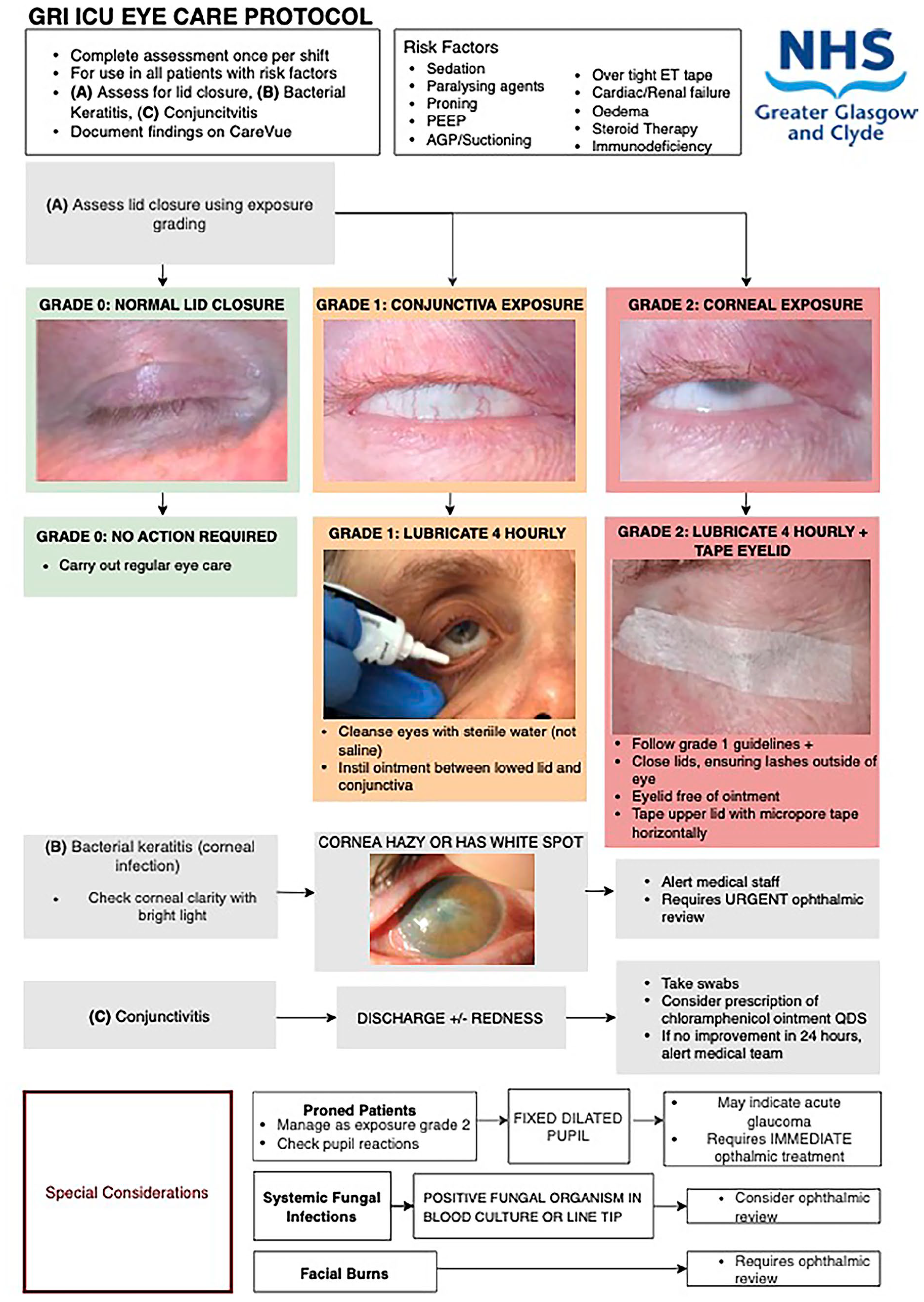
Eye care protocol poster.
Data collection
A preliminary snapshot audit in September 2022 was conducted. All current inpatients were included, and data was collected from their date of admission to the date of the snapshot audit. There were 17 patients with a cumulative length of stay (LoS) of 147 days. For each day of admission, patients were assessed for risk factors prompting eye care review as per the national guidance. This was done through checking various variables such as Richmond Agitation Sedation Scale (RAAS), type of ventilation (intubation, tracheostomy), whether receiving dialysis indicating renal failure and use of prone positioning. Documentation of eye care was collected which included whether exposure grading was charted, lubricant used, eye lid taping utilised and whether referral was made for specialist review. From the risk factors and eye care documentation, we were able to identify compliance with the national guidance.
Between December 2022 and March 2023, a re-audit was conducted after implementation of the quality improvement initiative. In this re-audit, we selected all current inpatients and followed the cohort until their discharge. The EPR was updated to allow for easier documentation of the eye care protocol, which encompassed risk factors, eye exposure grading, use of lubrication, lid closure status and signs of conjunctivitis or corneal opacity/infection. This refinement, especially the introduction of a dropdown checklist, not only standardised the recording of information but also facilitated more straightforward data extraction.
To gain a greater understanding of the incidence of eye exposure grading in the ICU, we analysed data spanning 9 months. This analysis covered the period from the eye care protocol’s integration into the EPR in October 2022 to the end of data collection in June 2023. With the eye care protocol now embedded within the EPR, we were able to make a targeted data request. This provided a list of patients for whom the specific variable was present. Specifically, we extracted records of patients who had either a grade 1 or 2 eye exposure grading, as well as those who had been reviewed by ophthalmology. We also requested records for the total number of patients admitted to the ICU during this time period along with their LoS.
Results
The preliminary snapshot audit of 17 inpatients, with a cumulative LoS of 147 days, showed risk factors present for all 147 days. Eye exposure grading was assessed on just 7 of these days (5%), and correct treatment was administered on 3 days (2%).
Following the quality improvement initiative, the re-audit included 13 inpatients and had a cumulative LoS of 338 days. Regarding LoS, the median was 23 (IQR 11.0–36.5) days. Risk factors were identified for 303 days (90%) of the admissions. Among these patients, 7 out of 13 (54%) experienced grade 1 eye exposure, while 1 patient (8%) had grade 2 exposure. The grading of eye exposure occurred on 233 out of the 303 days, reflecting a 76% adherence to the protocol. Of these, 211 days (90.6%) were categorised as grade 0, 20 days (8.6%) as grade 1 and 2 days (0.8%) as grade 2. Treatments aligned with the exposure grading were consistently given, with a 100% compliance rate, even during prone positioning.
The extended 9-month analysis included 535 patients. Regarding LoS, the median was 6 (IQR 2.0–9.5) days. Of these patients, 63 (12%) had grade 1 exposure, while 16 (3%) had grade 2 exposure. Seventeen patients were recommended for an ophthalmology review.
Discussion
The audit findings highlight the significance for standardised eye care in the ICU. With risk factors present for 90% of admission time and over half of patients experiencing eye exposure, there is a clear need for consistent eye care. The data from the extended 9-month period provides additional context on the incidence of grades 1 (12%) and 2 (3%) exposure.
The observed 76% compliance rate in grading eye exposure and 100% adherence to treatment according to grading suggests the protocol’s utility. This is further supported by the structured quality improvement approach, including PDSA cycles.
However, limitations should be noted. The initial documentation for eye care prior to the quality improvement initiative might not have captured all the care provided. For instance, exposure grading and treatment might not have been recorded, especially in cases where eyes were assessed as grade 0 (normal). Additionally, the incidence of eye exposure grading was notably higher in the re-audit group compared to the broader group of 535 patients across 9 months, representing the general ICU population. This discrepancy could be attributed to the re-audit group’s greater average LoS, potentially resulting in more days with risk factors present. As a national burns and Hepato-Pancreato-Biliary (HPB) centre, our ICU receives complex patients which can require extended lengths of stay. A potential cause for the greater LoS in the re-audit cohort may be due to a higher proportion of these patients in the re-audit group.
Furthermore, the preliminary snapshot audit covered a different time frame compared to the re-audit, complicating direct comparisons. Given the diversity of conditions ICU patients present with, a larger sample size might offer a clearer understanding of the link between risk factors and ocular complications.
The integration of the eye care protocol into the EPR system has facilitated the monitoring of protocol compliance and simplified data collection. Digital tools like this enhance the documentation process and contribute to more efficient healthcare operations.
Recognising the complexities of ocular health and disease, it’s evident that education should be a component of quality improvement initiatives in this domain. An educational programme, integrated into departmental inductions, can provide the necessary foundation for consistent protocol compliance and better patient outcomes.
In conclusion, the project highlights the benefits of a standardised eye care protocol in ICUs. The goal remains to reduce ocular complications and improve eye care. As this approach continues to be refined, it’s expected that outcomes will improve, and ocular complications will decrease. The discussion underscores the value of digital tools and education in the successful implementation of the protocol, suggesting a positive direction for ICU eye care in the future.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.