
Abstract
Introduction
Decision-making regarding admission to UK intensive care units is challenging. Demand for beds exceeds capacity, yet the need to provide emergency cover creates pressure to build redundancy into the system. Guidelines to aid clinical decision-making are outdated, resulting in an over-reliance on professional judgement. Although clinicians are highly skilled, there is variability in intensive care unit decision-making, especially at the inter-specialty level wherein cognitive biases contribute to disagreement.
Method
This research is the first to explore intensive care unit referral and admission decision-making using the Critical Decision Method interviewing technique. We interviewed intensive care unit (n = 9) and non-intensive care unit (n = 6) consultants about a challenging referral they had dealt with in the past where there was disagreement about the patient’s suitability for intensive care unit.
Results
We present: (i) a description of the referral pathway; (ii) challenges that appear to derail referrals (i.e. process issues, decision biases, inherent stressors, post-decision consequences) and (iii) potential solutions to improve this process.
Discussion
This research provides a foundation upon which interventions to improve inter-specialty decision-making can be based.
Introduction
Intensive care units (ICUs) are essential for the care of patients requiring organ support and a higher level of nursing input, but are disproportionately expensive to run due to equipment and staffing costs. 1 In the UK demand typically exceeds capacity, 2 creating a difficult set of inter-specialty (i.e. between medical and surgical specialties and intensive care services) decisions about patient referral and admission: non-ICU clinicians are responsible for referring patients whilst ICU clinicians are responsible for deciding whether to admit to the unit. Both groups are required to do this with outdated 3 or overly generalised 4 guidelines on how to make patient referral or admission decisions, and in the face of external pressures from the remainder of the hospital in improving patient flow. 5 When working in ambiguous, pressured and risky contexts, limited guidance can derail decision-making due to variations in perspectives of what constitutes the ‘right decision’, 6 based on different perspectives of risk, decision framing, past experiences, patient preference and organisational norms. 7 Biases such as these were reflected in variation in intensive care decision-making between Australian and New Zealand intensivists, wherein Australian doctors were more likely to admit patients than their New Zealand counterparts, 8 and a Pan-European study found wide variations in decision-making across the continent. 9 Such biases may be further exacerbated at the inter-specialty level.
There is little published research exploring ICU inter-specialty referral decisions in the UK. Moreover, the very nature of the NHS means that research in non-UK settings is largely incomparable, as care is funded by the state creating larger bed and fiscal pressures compared to non-UK hospitals. 10 The majority of ICUs in the UK are ‘closed’, meaning that specialist ICU clinicians (‘intensivists’) are responsible for admitting, caring for and discharging patients; 11 this makes many ICU clinicians in the UK the ‘gatekeepers’ who decide when not to admit patients, which contrasts to privately funded healthcare systems where patients and families have a greater role in deciding whether they opt for high-cost treatment. 12
Ultimately, decision-making regarding ICU admission is inherently complex and exacerbated by a lack of guidance at both individual and inter-specialty levels. Whereas ongoing studies are assessing the processes and rules behind such decisions,
13
the purpose of this research was to explore inter-specialty decision-making via an in-depth qualitative exploration of the experience of both ICU and non-ICU consultants, with a view to identify issues and develop potential recommendations for future research and practice. It had three research questions:
What are the steps involved in a patient referral to ICU? How might decision-making be derailed during the referral process? What are the potential solutions that might overcome derailments and facilitate inter-specialty decision-making?
Methods
Participants
An experienced sample of ICU consultants (n = 9, 18 years’ mean experience) and non-ICU consultants (n = 6, from oncology emergency medicine, neurology, renal and gastroenterology) was interviewed about their experiences of patient referrals. This sample was based on opportunity sampling until the point of thematic saturation (i.e. when the same themes repeatedly occur across participants and no new information emerges). Participants were recruited from a 700-bedded tertiary referral (Neurosciences, vascular, upper gastrointestinal and head and neck surgery) hospital and Major Trauma Centre in the North West of England with a closed, mixed level 2 and level 3 critical care unit receiving both general and specialist services.
Data collection
Participants were interviewed in a quiet private room located at their place of work. Interviews used the Critical Decision Method (CDM) 14 technique to identify the core challenges, and possible solutions, to ICU referral decisions. CDM was chosen as it is designed to identify how experts problem solve and the common strategies used to cope with uncertainty during choices with few guidelines. Incident-based approaches like this have also been found to increase accuracy of recall and richness of detail compared to unstructured interviews. 14 Interviews involve a multi-pass, retrospective discussion of a challenging decision made by the doctor in the past. We asked participants to recall a decision that was particularly challenging and stood out in their memory (rather than one that was recent but routine) in order to gather as much detail as possible about a memorable episode. Specifically, we asked consultants who were not from ICU to discuss a referral where a patient was refused admission, and ICU consultants were asked to identify a referral that they refused or believed was inappropriate. The CDM process involved four phases: incident identification (free narrative recall of the event); timeline verification (identification of crucial decision points); cognitive probing (identifying the factors that guided or hindered cognitive processing) and hypothetical consideration (alternative options/outcomes). Interviews ranged between 41 and 70 min, with a mean average length of 51 min.
Data analysis
Interview transcripts were thematically analysed 15 with support from the computer software NVivo. 16 Thematic analysis involves a process of inductive coding (i.e. generating new themes from the data) to identify emerging themes, refinement of themes into codes and further deductive coding (i.e. coding the data using existing themes) to produce a rich and detailed description of the data to answer our research questions. Coding was performed by an independent psychologist in the research team to enhance objectivity and reduce risk of prior assumptions about the ICU context, and themes were then discussed and refined to reach consensus with the rest of the research team, who have subject matter expertise to help contextualise findings.
Results
Results are split into three sections. First, we outline the general referral process as described by consultants from both ICU and non-ICU backgrounds. Second, we identify how decision-making might be derailed during this process. Third, we describe the potential solutions identified by participants that offer recommendations for future research and protocol design.
Patient referral process
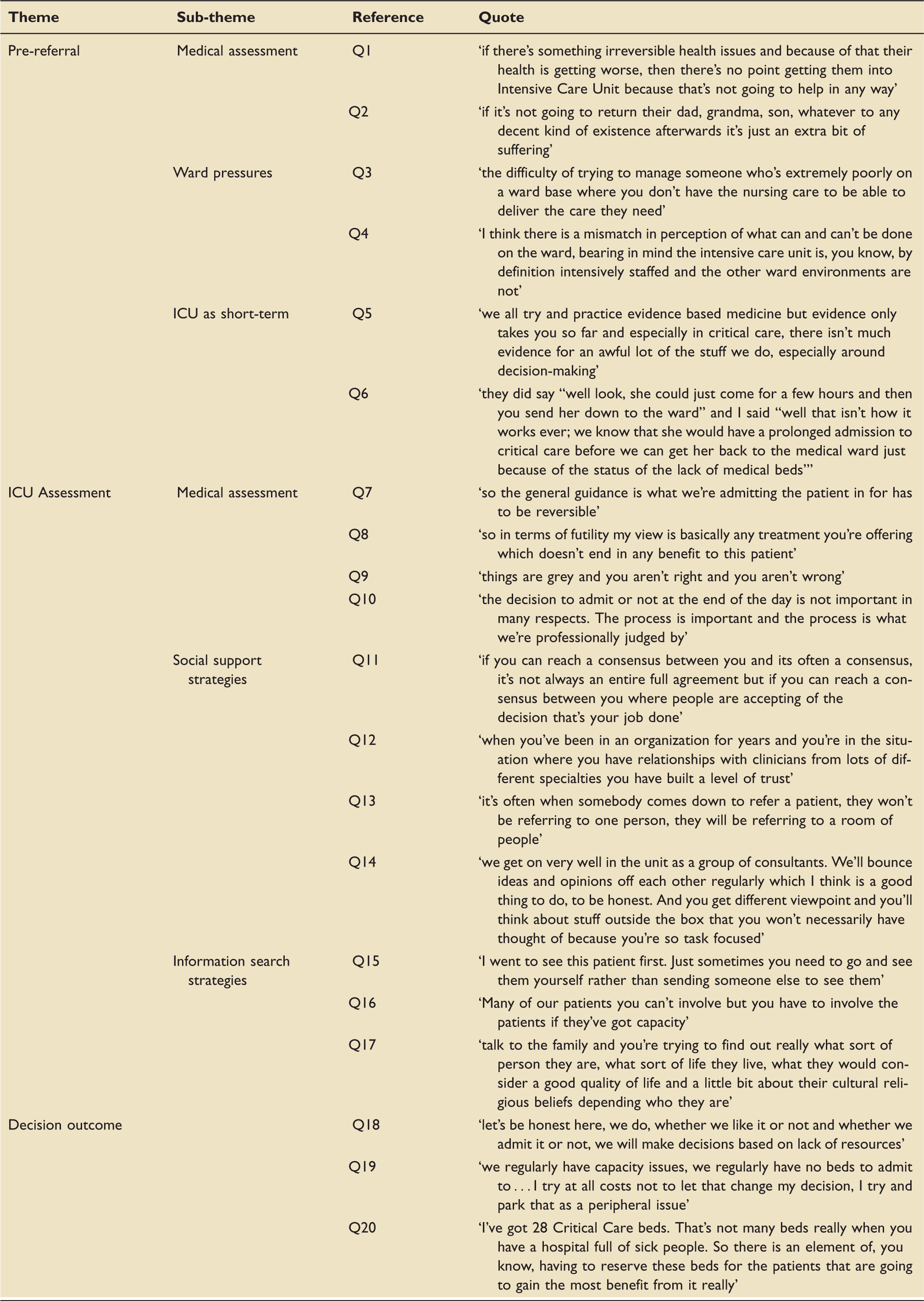
Interviews were coded to identify the different stages involved during a patient referral (Figure 1: black boxes = decision points; blue balloons = information sources that inform decision-making) (see Table 1 for quotes).
Patient referral pathway flow chart. Quotes from the general patient referral process section.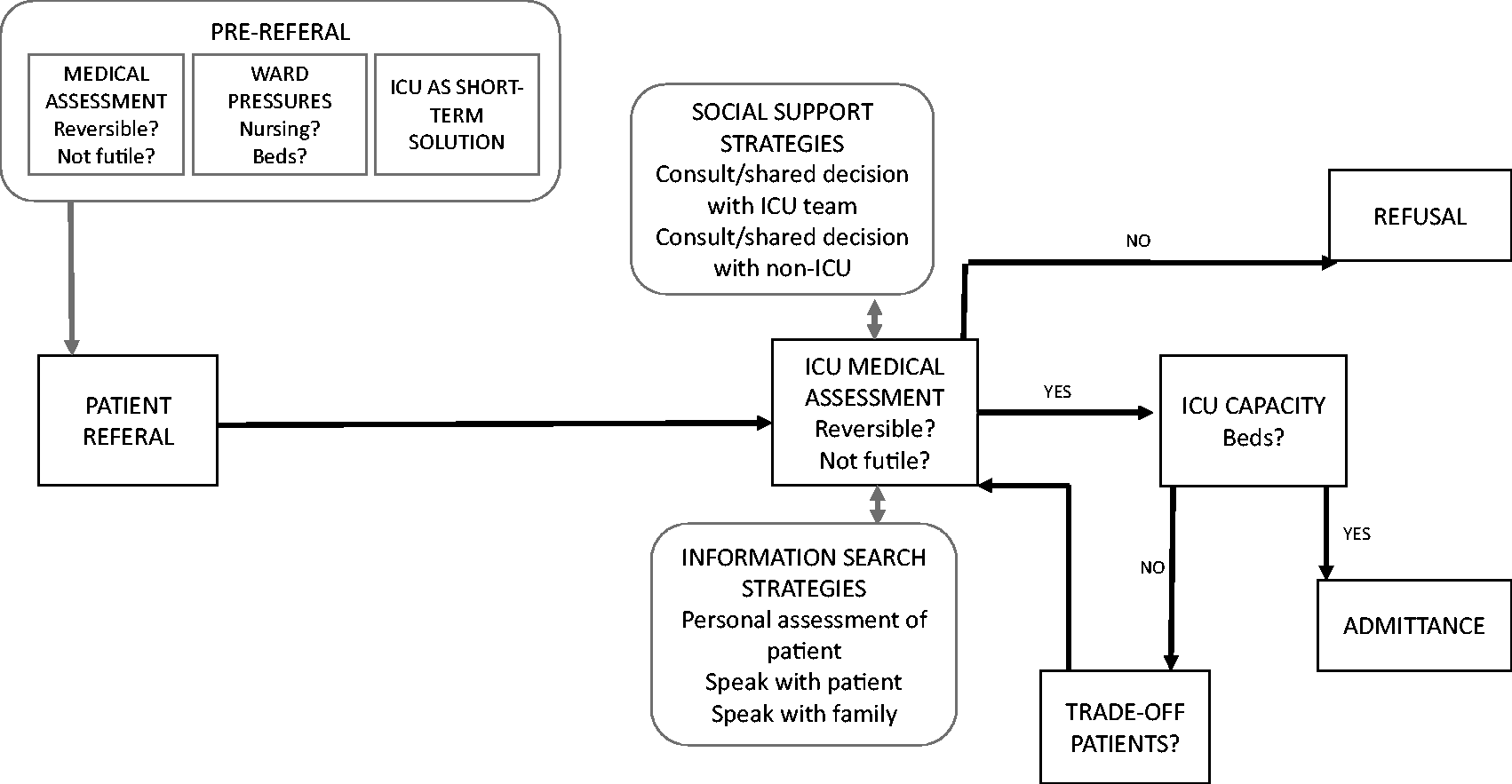
Pre-referral
The pre-referral phase describes the information sources used by non-ICU consultants when considering whether to refer a patient to ICU. As expected, a core consideration when deciding whether to refer a patient to the unit is the medical assessment, which was largely oriented around considering whether the patient’s condition was reversible (Q1), and whether treatment for the patient was futile or not (Q2).
A second consideration by non-ICU consultants was current ward pressures. Consultants described how they found themselves in a difficult position wherein staffing or bed occupancy levels on the ward made it challenging to treat the patient, and so ICU was a safer place to treat them, for example, when patients took up too much nursing time (Q3), or when non-ICU consultants felt available treatment on the ward was unsuitable to deliver in that setting (Q4).
A third consideration made by non-ICU consultants was using ICU explicitly as a short-term treatment option (Q5). However, there was a conflicting perspective from ICU consultants who described how patients inevitably spend a prolonged time on ICU, even if original admission was intended for a short period (Q6).
ICU medical assessment
When a patent referral is received by ICU, the primary considerations mirror those made by non-ICU consultants; specifically, reversibility (Q7) and futility (Q8). However, ICU consultants acknowledged there is often no clear right or wrong answer (Q9), and so the decision process must be clear and transparent to understand why decisions have been made (Q10). To alleviate uncertainty, consultants described two strategies: (i) social support strategies and (ii) information search strategies.
Social support strategies
To reduce uncertainty when deliberating over patient admission, ICU consultants described how they conferred with others to help make their choice. This might be via deliberation with doctors who had referred the patient (Q11) where it was noted that pre-existing relationships were beneficial (Q12); however, the largest social facilitator identified was reliance on the broader ICU team. Consultants described how decisions were rarely made in isolation (Q13) and described a sense of psychological safety in their team wherein they were able to critically reflect on decisions by considering the different viewpoints of the team (Q14).
Information search strategies
ICU consultants sought to reduce uncertainty about patient admittance by searching for information from different sources. The most efficacious method was via personal assessment of the patient on the ward (Q15), and they also identified that, where possible, it was important to get information from the patient themselves (Q16) or, if the patient was not capable of providing information, from family members or carers (Q17).
Decision outcomes
Decision outcomes were binary. If the ICU doctor judged the patient’s medical status as unsuitable for admission, based on grounds of irreversibility and futility, the patient was refused. Alternatively, if a patient was deemed suitable for admission, capacity to treat on ICU was then assessed (Q18). Indeed, consultants tried not to factor bed pressures in their decision (Q19), but acknowledged that this created a threshold for acceptance based on trade-off between current and prospective patients (Q20).
Derailments to referral process
A second goal to this study was to identify ways decision-making might be derailed during patient referrals. Derailments refer to the points in which decision-making deviates from the pathway model and the reasons why this seemed to occur. We thematically coded derailments into four superordinate categories: (i) process issues (i.e. complications that arose during the process of referring); (ii) inherent stressors (i.e. endogenous features of the intensive care environment that challenge decision-making); (iii) decision biases (i.e. preconceptions that might influence decision-making) and (iv) post-decision issues and consequences (i.e. issues that outlast the referral incident and inform subsequent interactions) (see Figure 2 and Table 2).
Points of derailment from patient referral pathway. Quotes from the derailments to the referral process section.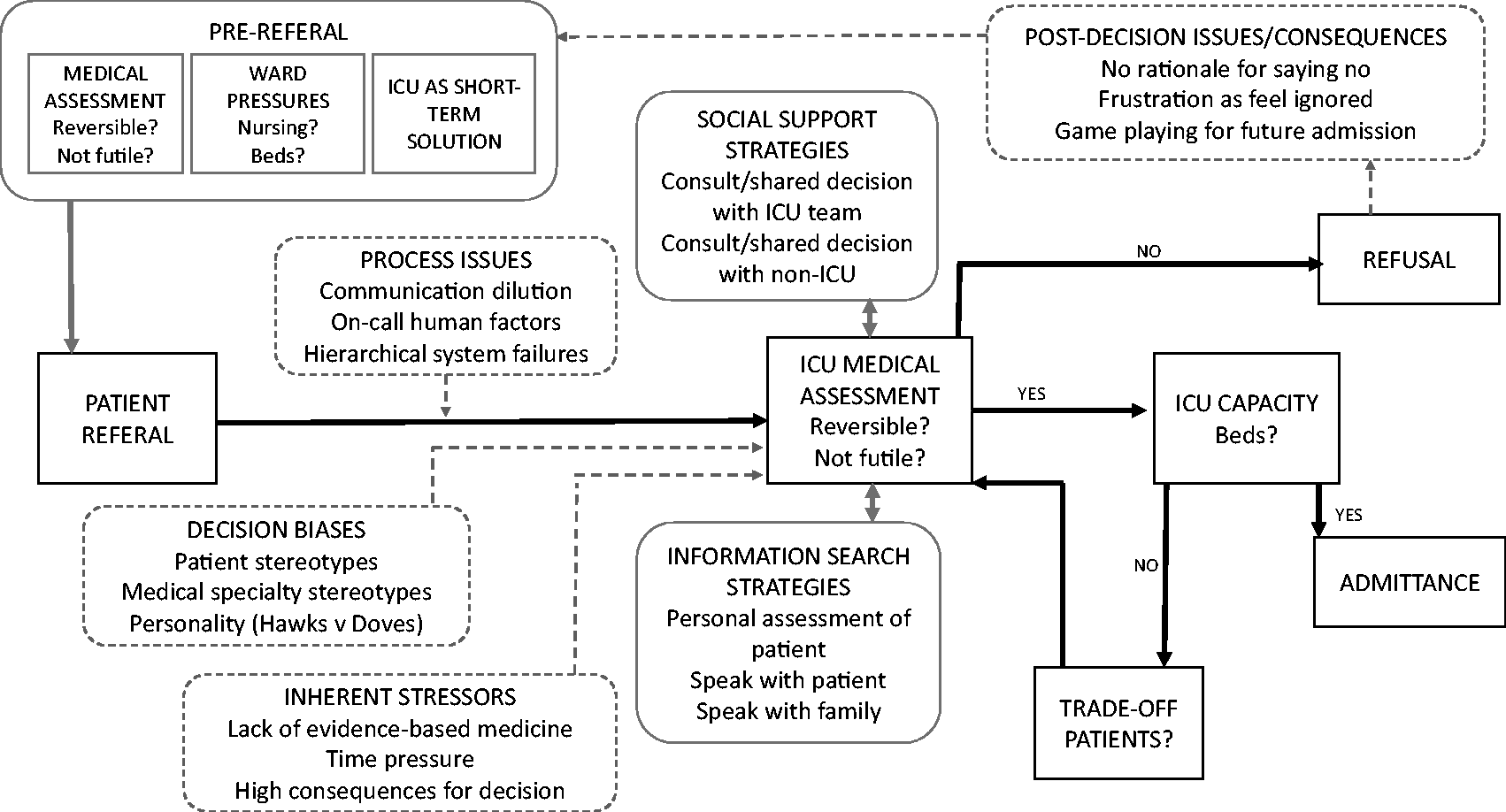
Process issues
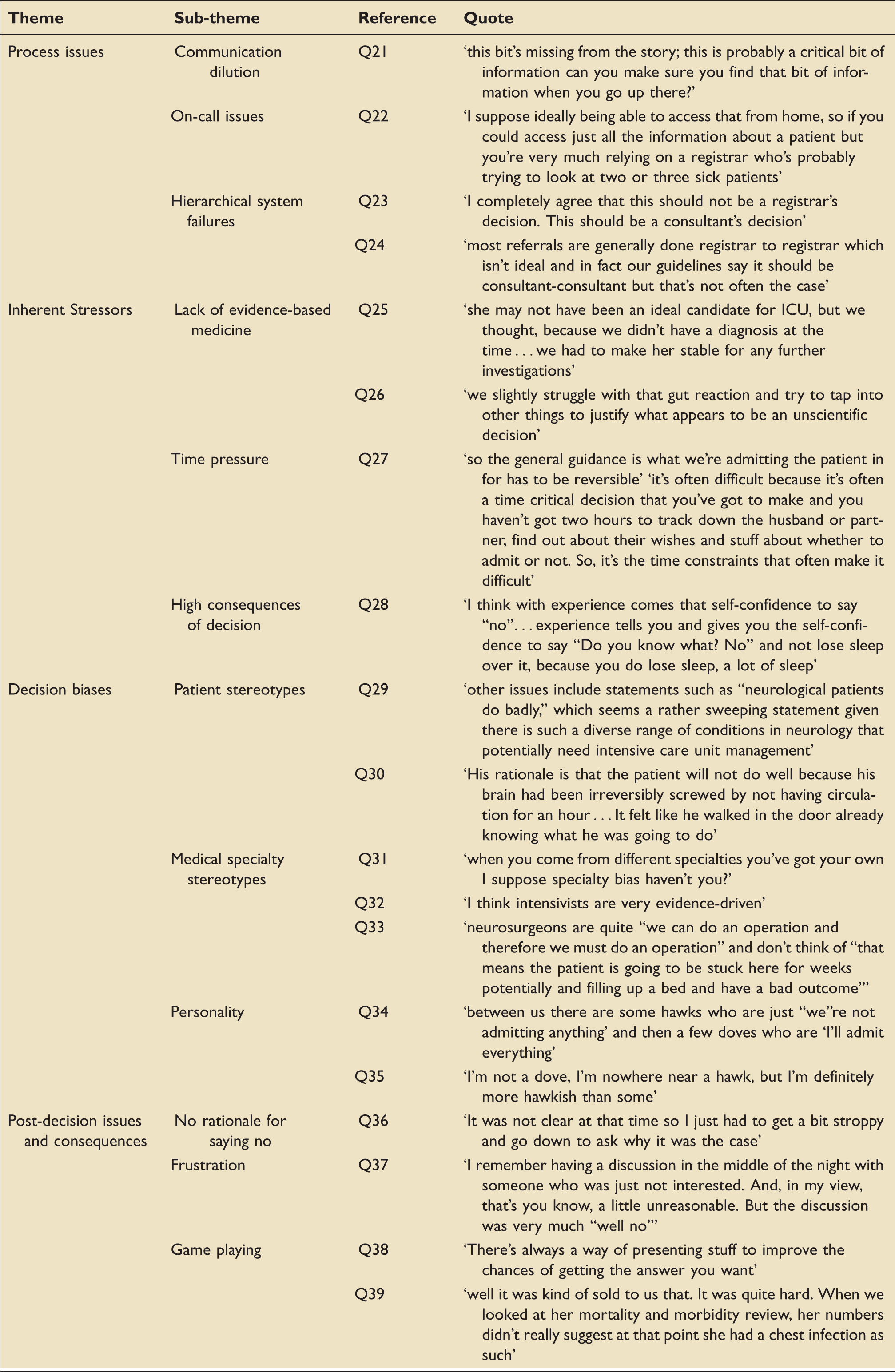
Referral process issues originated from three sources. First, communication dilution was identified as ICU consultants described how, at times, important information was missing that then had to be sought out first hand (Q21). Second, consultants described how human factors relating to the on-call system could derail decision-making, specifically in preventing physical interaction with the patient, instead relying on information from secondary sources (Q22). Third, it was identified that hierarchical system issues derailed the process. Specifically, it was identified across specialties that referrals should be at the consultant to consultant level (Q23); however, in practice this was often not possible and so reliance on more junior medical staff was common (Q24).
Inherent stressors
Three inherent stressors in the ICU environment made decision-making difficult. First, consultants described a lack of evidence-based information related to patient outcomes on ICU (Q25) and described conflict between perceived subjective estimates of benefit and a desire for evidence-based practice (Q26). Second, it was identified how time pressure was a core challenge as they had to make high-stakes choices rapidly and without full information (Q27). Third, consultants described the inherent emotional stressors linked to the potential negative consequences for making a wrong decision but acknowledged that experience was important for reducing this (Q28).
Decision biases
A number of cognitive biases were identified which could derail the decision-making process. A core bias identified by non-ICU consultants was the use of patient stereotypes used by ICU consultants when considering whether patients should be admitted to the ward (Q29). This was associated with frustration on behalf of the non-ICU consultant, who often felt that they were not being listened to when they tried to argue for the unique characteristics of the patient that deviated from stereotypes (Q30). Similar was the impact of medical practitioner stereotypes to reflect assumed decision-making styles of different specialties (Q31). This was described across specialties wherein participants described how different types of doctors approached medicine in different ways (Q32) and were biased by narrow thinking about their medical or surgical specialty rather than the bigger picture (Q33). A final bias that was discussed by ICU consultants related to stereotyped views about their own personality. Specifically, this referred to whether they were a ‘hawk’, deemed to use more stringent criteria for admission, or a ‘dove’, and more liberal in their criteria for admission (Q34). Consultants from ICU discussed this as a way of rationalising their decision process, by reflecting on their personal tendencies to admit patients or not (Q35).
Post-decision issues and consequences
Negative experiences that arise during a referral can have consequences on future events. Non-ICU consultants expressed frustration for not having a clear rationale for why patients they referred were not admitted (Q36). They described how this led to frustration at being ignored (Q37). Interestingly, they identified that, sometimes, this caused them to adapt their practice to ‘game play’ for admission. This might be when trying to get the same patient who had been refused admittance by using different language or presenting information in different ways or to different consultants (Q38). Indeed, this was something also identified by ICU consultants, who described how they sometimes felt that patients were being ‘sold’ for admission to ICU, largely by not being provided with a full picture of patient status and co-morbidities (Q39).
Potential solutions to facilitate the referral process
Quotes from the potential solutions to facilitate the referral process section.
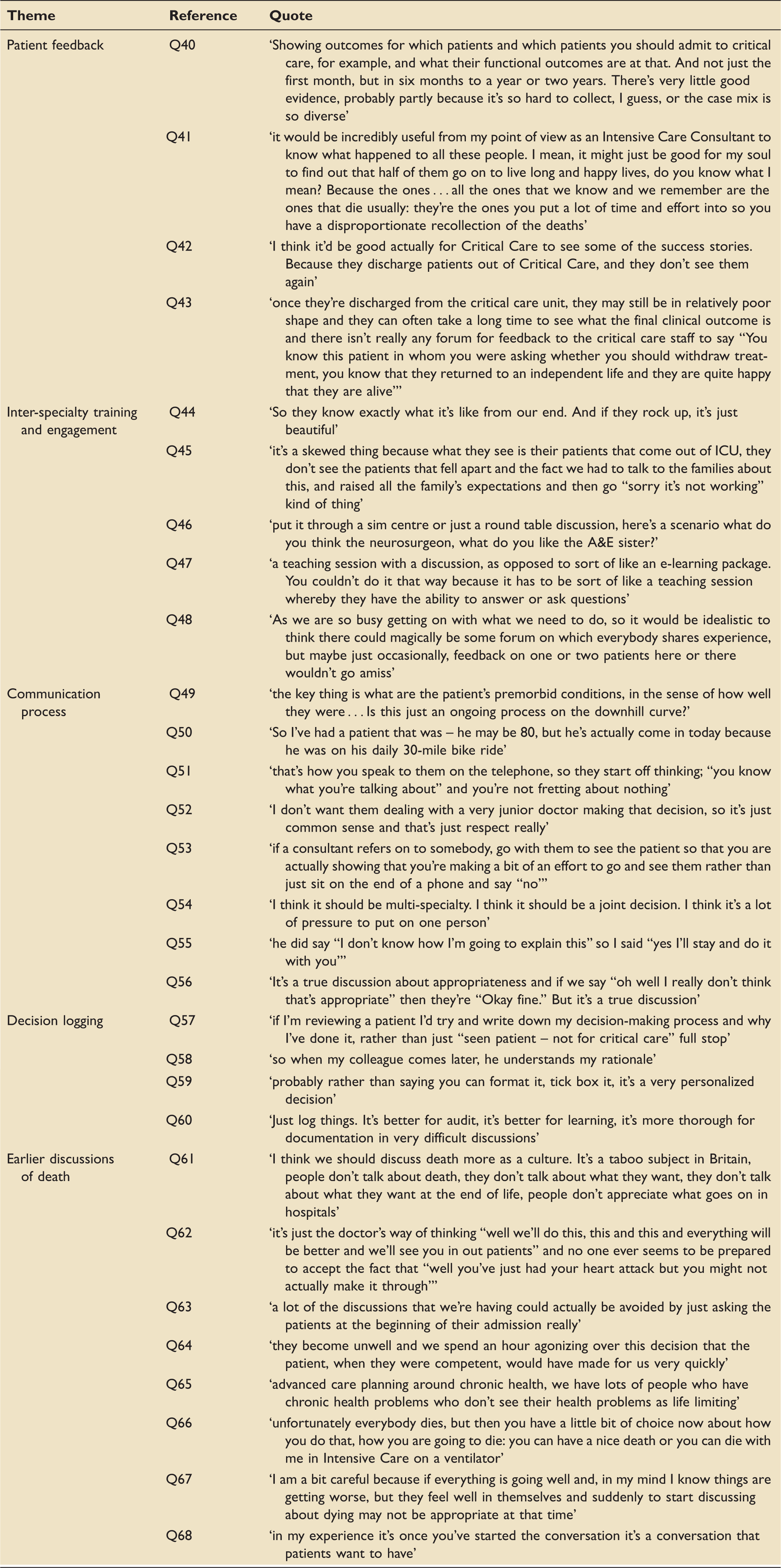
Patient feedback
As identified earlier, a lack of evidence-based information on patient outcomes post-ICU made decision-making challenging, and it was expressed that more information about patient outcomes in the short-, medium- and long-term might help to support decision process (Q40). Patient feedback was perceived as useful at an emotional-level by ICU consultants who felt they often tended to remember patients that die rather than those that survive (Q41). This was also acknowledged by non-ICU consultants who identified the biased exposure ICU consultants have to positive patient outcomes (Q42). Furthermore, non-ICU consultants also identified that feedback should be long-term (Q43).
Inter-specialty training and engagement
It was acknowledged across both groups of consultants that greater engagement between specialties would support the referral process. Having worked together before or being exposed to each other’s place of work was seen as beneficial for teamwork by enhancing role understanding (Q44). It was identified that training might help to educate non-ICU consultants on some of the reasons for non-admission (Q45). In terms of how such training could be delivered, it was suggested that simulations could be useful (Q46) and emphasized that training must crucially involve physical interaction and discussion between specialties (Q47). However, it was acknowledged that time limitations were problematic for ideal inter-specialty engagement (Q48).
Communication process
Related to training, consultants reflected on lessons they had learnt through experience relating to communications between specialties. Non-ICU consultants identified the importance of providing a full picture of a patient. This might include information about other medical conditions not directly linked to the referral (Q49) and unique information about the patient as a whole that might deviate from normative assumptions (Q50). Consultants described how appropriate communications were essential for facilitating a sense of trust and professional respect between teams (Q51). Non-ICU consultants also reflected on how decisions not to admit should be at the consultant level to show professional respect (Q52). It was suggested that when a patient was being refused, that face-to-face discussions were important (Q53). Indeed, a suggested benefit of good communication and respect across specialties was to reduce the pressure associated with decision-making by making it a shared process (Q54). This was further identified as being helpful if a patient was not going to be admitted to ICU, where ICU consultants can support non-ICU consultants in explaining why a patient is not going to be admitted in difficult situations (Q55). Generating professional respect also facilitated communications by allowing for a more honest discussion, rather than considering ulterior motives (Q56).
Decision logging
Consultants suggested that one way to improve the referral process would be via decision logging, and that logging should go beyond merely listing actions and must include a clear rationale for why those decisions have been made (Q57), which can also facilitate patient handovers during shift changes (Q58). It was also suggested that this type of log should be free text rather than pro-forma (Q59). Logging was also perceived to help make decision-making more transparent during difficult decisions, thereby reducing some of the issues linked to lacking a rationale for ‘no’ decisions (Q60).
Earlier discussions of death
It was acknowledged across specialties that ICU referrals would be easier to manage if there were more open discussions of advanced care planning both with patients and between doctors (Q61). This was identified as an issue for the medical profession, wherein doctors tend not to think about death due to their desire to treat and cure (Q62). It was suggested that this could be part of the standard process during admission (Q63) as it could reduce the need to make referral decisions if the patient’s wishes regarding ICU are already known (Q64). It was highlighted that this is crucial when treating patients with chronic conditions (Q65) and that more discussions of death could help people make informed decisions about this inevitability (Q66). Although it was acknowledged that discussions of death must be carefully managed in line with the emotional wellbeing of the patient (Q67), it was recognized as the responsibility of the referring doctor to address the topic to allow this conversation to happen (Q68).
Discussion
We have taken an initial step in developing a deeper understanding of the processes and challenges faced by clinicians making and receiving referrals to intensive care. Specifically, we have identified how referrals can be derailed due to: (i) process issues, (ii) inherent stressors, (iii) decision biases and (iv) post-decision issues and consequences. Our research has also offered tentative suggestions as to how this process might be improved.
A major stumbling block identified with both ICU and non-ICU clinicians remains the lack of evidence base regarding the utility of intensive care services for patients referred in terms of functional outcomes. One study that sought to review long-term mortality for ICU patients concluded that inconsistent approaches to research (low quality, variation in case-mix, study design, case-mix adjustment differences) made it difficult to assess findings. 17 Without such an evidence base, we are unable to have frank discussions with referring teams, and where possible patients themselves, regarding the potential risks and benefits of admission to ICU. As a result, this continues to be a field where anecdote and experience trumps data-driven decision-making, allowing for the intrusion of cognitive biases and ‘game playing’ into the decision-making process. Such data would reduce the subjective component of these discussions, but would need to be acquired via large-scale national research and data-collection projects requiring significant backing from funders; for example, longitudinal data collection and analyses on the short-, medium- and long-term outcomes of patients discharged from ICU. 18
Other solutions might be appropriate to localized trials at trust or regional level; for example, developing pro-forma to standardize decision logging during patient referrals which would become easily available evidence in the case of future hospital admissions and referrals to intensive care, and allow audit of decision-making processes; or a trial wherein all patients are asked to identify their preferences regarding resuscitation and escalation in the case of deterioration during their admission to hospital.19,20 Studies have demonstrated disparities between patients’ wishes and decisions made by treating clinicians at the time of requiring life-sustaining interventions 21 leading to inappropriate intensive care interventions, 22 when ‘mandatory’ advance care planning would allow any conflict between the patient’s expectations and their likely clinical course to be discussed and recorded early in their stay. This would reduce the tendency to delay decision-making until brought about by the discussion with intensive care services regarding their suitability for escalation, shifting the burden for such decision-making from ICU clinicians and patients’ relatives back to the patient’s primary treating team and the patient themselves. 23
Teams might also benefit from external collaboration with researchers; for example, using immersive simulated training scenarios to test interventions related to communication processes and identifying its impact on collective team performance. Such research would further support the desire for greater multi-specialty engagement as a result of these activities, which might be further strengthened via structured debriefs to understand variation in clinical views. For example, preliminary evidence from a meta-analysis suggests that structured debriefs can have benefits of improving clinician knowledge and skill acquisition. 24 Ultimately ICU and non-ICU clinicians will have differing cognitive biases inherent to this decision-making process; ICU consultants will often perceive an intensive care admission in terms of the detrimental impact on patients’ wellbeing, whereas non-ICU consultants are biased by their involvement with intensive care patients being predominantly those who improve and are discharged back to their ward, or patients who were refused ICU, and so die in their care. By use of simulation and structured feedback, one could hope to allow each side of this, at times, adversarial approach a greater insight into the cognitive and emotional processes underpinning the others’ decision-making processes and help to avoid this subjective aspect being the dominant driver in inter-specialty discussions. In particular, this would avoid the game-playing highlighted above, which has the potential to not only detrimentally affect both the experience of the patient being referred but also weaken the professional relationship between specialties as well as impact the availability of intensive care services.
It was notable that both ICU and non-ICU consultants highlighted aspects of the hospital system external to intensive care as drivers on their decision-making process, which needs buy-in from the rest of the hospital system to be improved upon. In particular, patients were being escalated due to inadequate staffing of nursing on general wards, a factor directly correlated with inpatient mortality elsewhere.25,26 This has the potential to worsen in the current economic and political climate of the UK’s health system 27 and the ever-present issue of worsening bed pressures both in intensive care and in the wider hospital.5,28 Although both groups stated they make a conscious effort to avoid this impacting on patient care, it does place the firmest constraint on whether the intensive care resources are available for a particular patient, and on the wards preventing discharge back in to the hospital environment upon recovery from critical illness.
This final point combines with the concept of ‘mission creep’ within intensive care, wherein a patient admitted for one clinical reason remains in ICU for an extended period of time due to a combination of issues. ICU consultants highlighted bed pressures, perceived lack of input to their care from their referring team, and management of further pathological processes which were not apparent at the time of referral, which increase their length of stay and so further impact on ICU bed availability.29,30 It would be of interest to explore the causes of mission creep further as this has clinical, psychological and economic effects on patients, relatives and ICUs.
Conclusion
This qualitative paper not only highlights the challenges associated with ICU decision-making but offers a practical framework around which solutions to overcome challenges might be operationalized. It is recommended that this framework be used as a basis upon which to develop understanding on the challenges to ICU decision-making, and to guide future research and quality improvement projects that seek to facilitate the inter-specialty decision-making process. Specific areas of interest include the perceived lack of evidence base, consideration of how decisions are logged at local and national levels, the causes and ramifications of ‘mission creep’ and improving communication between teams.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Lancaster University’s Faculty of Science and Technology Research Grants fund.