
Abstract
Introduction
We evaluated intensive care medicine trainees’ practice of emergency intubations in the United Kingdom.
Methods
Retrospective analysis of 881 in-hospital emergency intubations over a three-year period using an online trainee logbook.
Results
Emergency intubations out-of-hours were less frequent than in-hours, both on weekdays and weekends. Complications occurred in 9% of cases, with no association with time of day/day of week (p = 0.860). Complications were associated with higher Cormack and Lehane grades (p=0.004) and number of intubation attempts (p < 0.001), but not American Society of Anesthesiologist grade. Capnography usage was ≥99% in all locations except in wards (85%; p = 0.001). Ward patients were the oldest (p < 0.001), had higher American Society of Anesthesiologist grades (p < 0.001) and lowest Glasgow Coma Scale (p < 0.001).
Conclusions
Complications of intubations are associated with higher Cormack and Lehane grades and number of attempts, but not time of day/day of week. The uptake of capnography is reassuring, although there is scope for improvement on the ward.
Introduction
In-hospital emergency intubations are often performed in patients with limited physiological reserve, with limited planning, and occasionally in suboptimal locations (e.g. general wards). Over 1 million (emergency and elective) intubations are performed annually within the National Health Service (NHS) alone. Recommendations on equipment availability, rapid sequence induction (RSI), use of induction agents and neuromuscular blockade, and confirmation of intubation are available to improve the safety of emergency intubations. 1
The 4th National Airway Project (NAP4) highlighted the inherent dangers of emergency intubations. 2 Poor planning of airway control was noted to correlate with poor outcomes and is particularly relevant in emergency intubations. This ability to plan is compromised by the inherent nature of emergency intubations, but should be mitigated as much as possible by availability of all necessary equipment for intubation regardless of location, with specific mention in multiple guidelines of capnography.2,3
Intensive care doctors are faced with increasingly complex patients “with deranged baseline physiology and complex conditions who are disproportionately likely to experience airway difficulty, presenting challenges to airway safety in the intensive care unit (ICU)”. 4 We undertook a retrospective, observational study of tracheal intubation performed by critical care trainees in United Kingdom to identify practice and complications. The primary objective was to ascertain factors associated with complications of intubations. The secondary objectives were to ascertain differences in intubation practice and complications in hours compared to out of hours and to describe the drugs commonly used. Findings should have implications on workforce planning and airway training for intensive care trainees.
Methods
An online logbook, “MedELogbook” (www.medelogbook.com) designed for ICU junior doctors to log their referrals, transfers, procedures, and resuscitation calls was created in September 2013. Individual users entered data prospectively. Three consecutive years of data (2014–2016) were extracted from the database on 10 January 2017. All user data were anonymised.
Inclusion criteria included patients aged 16 years or older who underwent emergency intubations. Exclusion criteria were logs from outside the UK and data logs from consultants. Variables used in the analyses included age, Cormack and Lehane classification of laryngeal view (CL grade), American Society of Anesthesiologist (ASA) classification, complications, drugs used, Glasgow Coma Scale (GCS), gender, location where intubation took place (accident and emergency (A&E), ICU, operating theatres (ORs), ward), patient category (medical or surgical), time of day of intubation, use of capnography, level of supervision (assisting other, directly supervised, independent, indirectly supervised, teaching a colleague, and “other”), number of attempts at intubation, and use of video laryngoscopy. Complications were selected from a dropdown menu of the following choices: airway trauma, aspiration of gastric contents, “can’t intubate can’t ventilate”, desaturation, failed intubation, oesophageal intubation, and “other”. It was possible to select more than one choice. Furthermore, it was possible to enter free text into the logbook to provide further detail.
Acknowledging that the precise working pattern may vary between ICUs, we divided each day into “daytime” (08:00–17:59) and nighttime (18:00–07:59 the next day) for both week days (Monday–Friday) and weekends (Saturday–Sunday).
Missing data
It was mandatory for trainees to complete the following data fields; age, gender, location where intubation took place, patient category, time of day, complications, use of capnography, airway grade, ASA classification, supervision, and number of attempts. GCS prior to induction, drugs used, and time taken were optional data fields.
Ethics
All users accepted the terms and conditions on registering that “all data entered will be aggregated into a database for the purpose of research and audit. This may be published or presented in a public domain (e.g. conferences, journals, online). MedELogbook has the right to use any data entered for this purpose. This database will not be used to interrogate the data entered by individual users.” Under Section 251 of the NHS Act 2006, NHS Health Research Authority ethical approval is not required as no patient identifiable information is used. 5 The local Research Governance & Regulatory Assurance Manager at St George’s NHS Healthcare Trust, confirmed that no ethics approval was required.
Statistics
Analyses were performed using SPSS (Version 22, IBM). Differences in continuous variables between groups were compared using the Kruskal–Wallis test. Continuous variables are presented as median (interquartile range). Differences in categorical variables are compared using chi-squared test. Multivariate analysis using logistic regression was performed to assess variables associated with the incidence of complications. Factors included in the multivariate analysis included variables associated with complications on univariate analysis. A p-value of < 0.05 was taken as being statistically significant for all analyses.
Results
Details of patient demographics and intubation procedure.
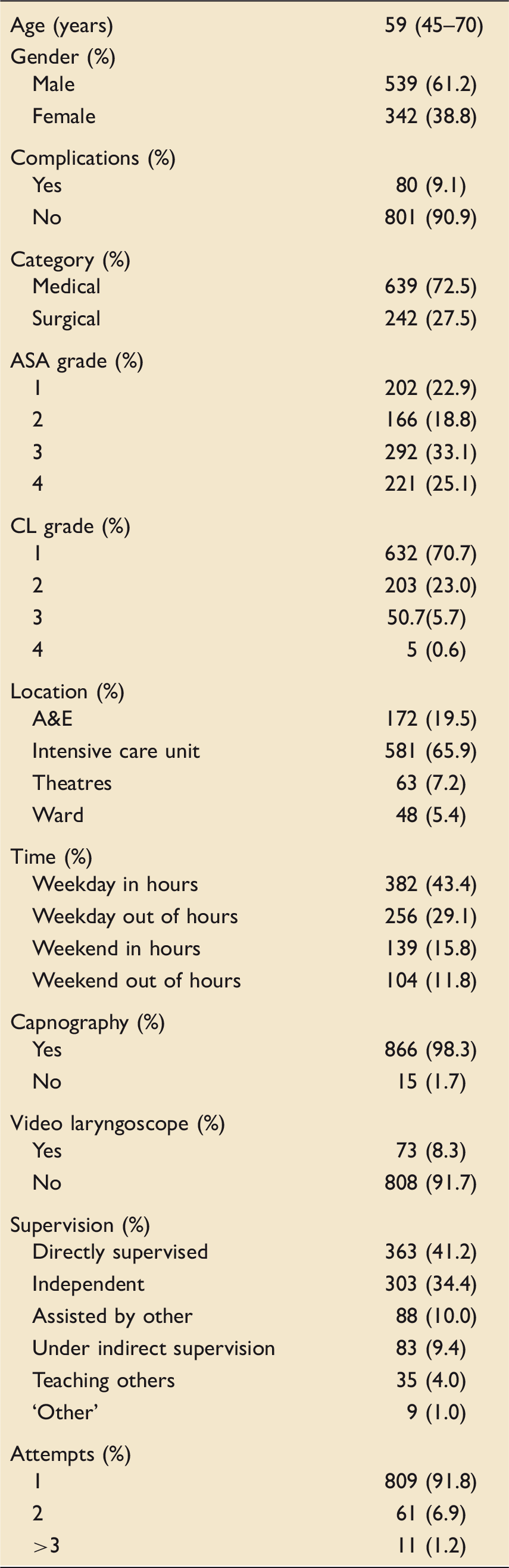
A&E: accident and emergency department; ASA: American Association of Anaesthesiologist; CL: Cormack and Lehane classification of laryngeal view.
Of the 881 intubations recorded, 500 (56.8%) were performed by trainees in ICM also sub-specialising in anaesthesia, 214 (24.3%) by trainees in ICM (without a second specialty), 153 (17.4%) by trainees in ICM with an internal medicine sub-specialty, and 14 (1.6%) by other (e.g. emergency medicine) trainees. Majority of entries were by specialist trainees in the first years of specialist training (ST1–ST3) (n = 383; 43.5%), and in the last years of specialist training (ST4–ST7) (n = 285; 32.3%). Doctors who were trainees but not on a formal training program accounted for 114 (12.9%) reported intubations.
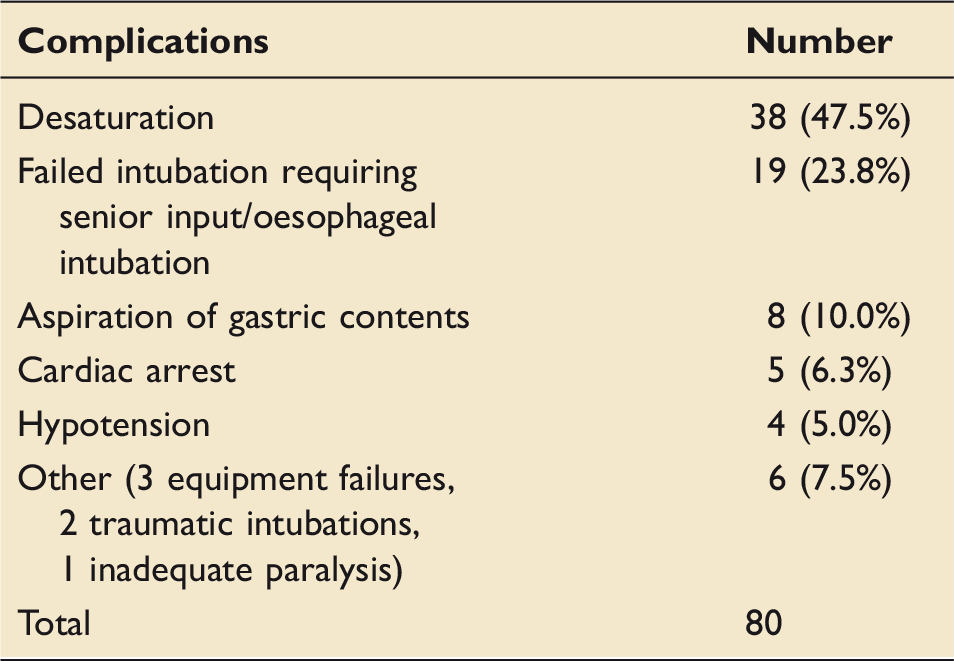
Complications associated with emergency tracheal intubation.
Complications
Complications were noted in 80 of the 881 (9.1%) intubations (Table 2). Most complications occurred under direct supervision (n = 37; 47.5%), followed by independent intubations (n = 25; 31.3%), assisting others (n = 12; 15%), and indirect supervision (n = 5; 6.2%). Similar number of complications were reported by specialist trainees in the first years of specialist training (ST1–ST3) (n = 31; 38.8%) and in the last years of specialist training (ST4–ST7) (n = 31; 38.8%). Doctors who were trainees but not on a formal training program accounted for 18 (22.4%) reported complications.
There were a disproportionate number of complications among higher CL grades (p < 0.001). Complications were reported in 6.6% of CL grade 1 (n = 623), 10.8% of grade 2 (n = 203), and 32.0% of grade 3 airways (n = 50, p ≤ 0.001). There was insufficient number (n = 5) of CL grade 4 intubations for statistical analysis. Patients with CL grade 3–4 views had a greater proportion of ≥3 intubation attempts than patient with CL grade 1–2 views (10% vs. 2.0%, p < 0.001). Patients with complications had a greater proportion of three or more attempts at intubation (7.5%) compared to patients without complications (0.6%) (p < 0.001). There was a significant association between video laryngoscopy use and complications, with a greater proportion of intubations with video laryngoscopy use (19.2%) having complications compared to direct laryngoscopy (8.6%) (p = 0.004). However, video laryngoscopy was used more often in patients requiring more than one attempt at intubation (17.8% vs. 7.1%. p < 0.001).
A greater proportion of ASA grade 3 (40.1%) and grade 4 (50.2%) compared to grade 1 (35.1%) and grade 2 (36.7%) intubations took place out of hours (p = 0.007). However, there was no association between time of day and complications. Furthermore, a greater proportion of intubations in ASA 4 patients was independent (41.6%) compared to directly supervised (19.6%) (p = 0.024).
Emergency intubations on the ward were associated with greater complication rates (14.6%) compared to other locations (<10%), although this did not reach statistical significance (p = 0.065). Age of patient, time of day and day of week, ASA grade, pre-intubation GCS, medical/surgical patients, and use of capnography had no association with complication rates. The predictors of complications in multivariable logistic regression were number of attempts (OR = 5.95 (3.218–11.010); p < 0.001) and CL grade (OR = 1.729 (1.186–2.521); p = 0.004).
Time of day and day of week
Characteristics of emergency intubations by time of day.
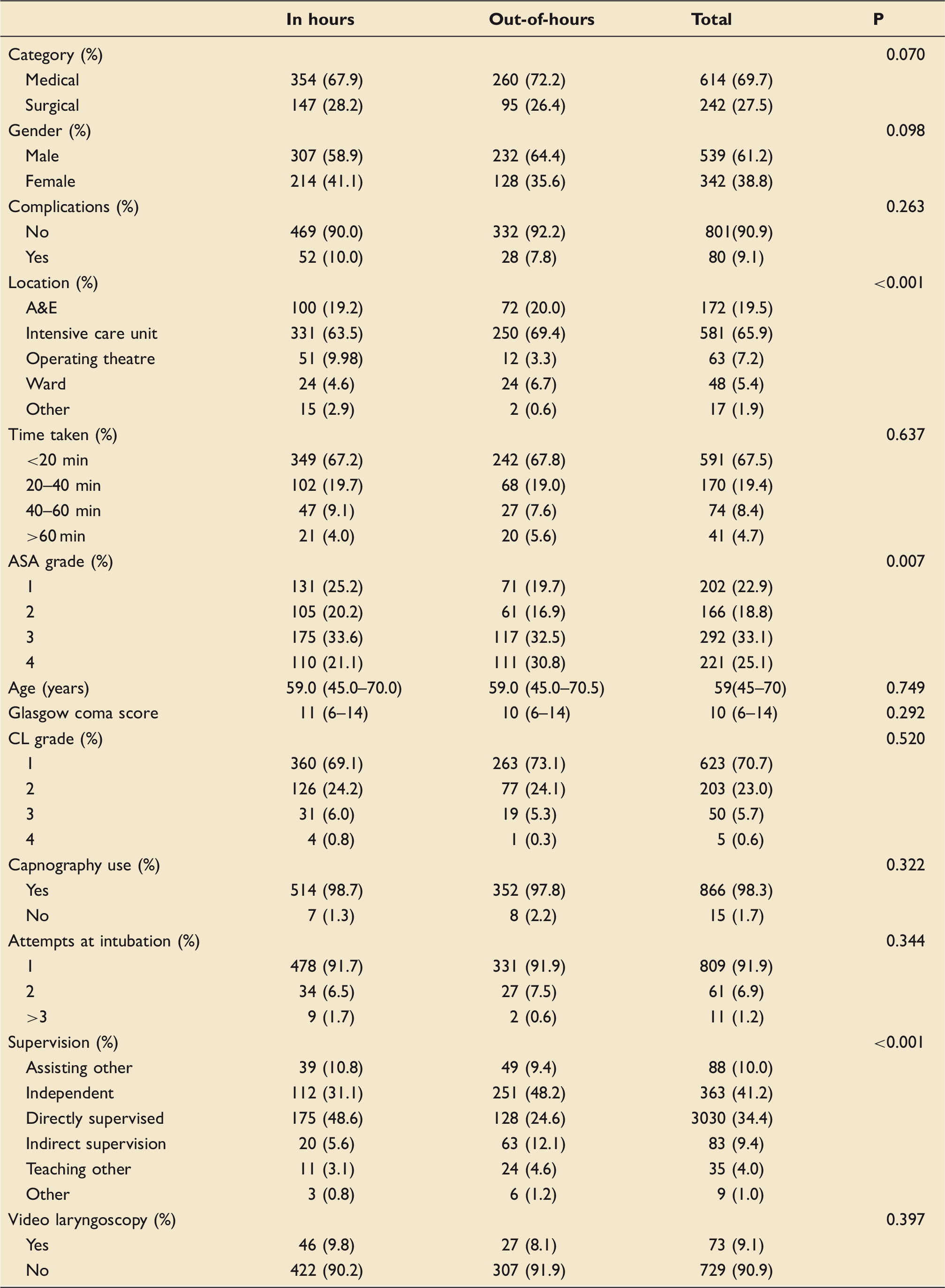
A&E: accident and emergency department; ASA: American Association of Anesthesiologist; CL: Cormack and Lehane classification of laryngeal view.
Note: p-values are for comparison of proportions between in- and out-of-hours.
A greater proportion of the intubations that took place overnight were independent compared to supervised (48.6% vs. 24.6%) in contrast to more intubations taking place during the day being directly supervised compared to independent (48.2% vs. 31.1%) (p < 0.001). There was also a significant association between out-of-hour intubations and higher ASA scores (p = 0.007). 35.1% of ASA 1 intubations were out of hours compared to 50.2% of ASA 4 intubations. Despite this, time of day was not associated with complication rates (p = 0.263) or number of intubation attempts (p = 0.344).
There were no differences between in-hours and out-of-hours intubations and other variables (Table 3). There was no positive association between day of week and any variables.
Capnography
Capnography was used in 866 (98.3%) intubations. Capnography was used in the operating room and A&E on every occasion, in contrast to the ward or the ICU (p < 0.001). Capnography was not used was on the ICU in 1.4% of intubations and in 14.6% of intubations on the ward. Patients on the ward were the oldest (p < 0.001) and had a disproportionately higher number of ASA 4 patients (41.7%) compared to other locations (p < 0.001), and patients on the ward and in A&E had the lowest pre-intubation GCS (p < 0.001) compared to other locations.
Use of drugs
The choice of sedatives was recorded in 728 (83%) intubations. Propofol is by far the most common induction agent used, in 550 (76%) intubations. Propofol alone was used in 253 (35%) intubations and was most commonly paired with fentanyl (n = 134, 18%). Fentanyl was the more popular opiate, being used in 261 (36%). Thiopentone was used in 119 (16%) cases; 58 (8%) of cases as the sole sedative agent.
Choice of neuromuscular blocking agent was recorded in all intubations. Rocuronium was the most commonly used neuromuscular blocking agent, and was used in 484 (55%) of cases. Suxamethonium was used in 269 (31%) cases, and atracurium was used in 96 (11%) cases. Nineteen (3%) of the intubations did not require neuromuscular blocking agents. The most popular combination of neuromuscular blocking agent and sedative is rocuronium with propofol (129, 18%) followed by rocuronium with propofol and fentanyl (109, 15%). The use of vasopressors was not recorded.
Discussion
We present a large contemporaneous dataset of emergency intubation practices among intensive care trainees in the UK. The case mix of patients is representative of UK ICU demographics; the age of patients and proportion of medical/surgical patients are similar to recently published data from the Intensive Care National Audit and Research Centre (ICNARC) case mix programme. 6 Furthermore, the incidence of complications is in keeping with the published literature.7–15
Our findings represent current practice following publication of findings and recommendations of the NAP4 audit. 2 A national survey conducted following the NAP4 audit found improvements in practice including “improved provision of difficult airway equipment and more widespread routine use of capnography”, 16 and that although ICU had significant improvements in practice, there was room for improvement. While surveys and clinical studies provide useful information, this dataset provides insight into “real life” practice. Shortfalls in airway management in the critically ill patient have a significant human and financial cost. 17
Complications
Among emergency intubations carried out by UK intensive care medicine trainees, there is an overall complication rate of 9.1%, with desaturation being the commonest complication (accounting for 47% of all complications). Complications were associated with increasing CL grade and number of attempts at intubation rather than ASA grade. Others have demonstrated the association between difficulty intubations and complications. 10 If the initial attempt at intubation fails, the chance of success declines with each subsequent attempt at laryngoscopy8,18 and the number of attempts at intubation is associated with increasing complications.12,13 Greater clinical experience and attending supervision of junior practitioners are associated with fewer complications.8,13
The proportion of complications was relatively high in intubations done as part of training (directly supervised). From the data available, it is not possible to comment on the severity or outcomes of these complications. Furthermore, we are unable to ascertain the clinical experience of individual doctors. It is inevitable that there will be a learning curve with airway management in the critically ill patients and adequate structured training should mitigate risk. 19 Training to include airway management in elective ASA 1 patients, scenario-based training with computerised patient simulator to improve mechanical skills of intubation and team leadership respectively, and cadaver-based training are effective tools in airway management training among critical care trainees.20,21
There are variations in reported complication rates which reflect heterogeneity in patient demographics and illness severity, level of training of doctors, and definitions of complications. For instance, the degree of desaturation or haemodynamic instability is not binary and is contextual. Therefore, the clinician may be best placed to judge the presence or absence of any complication. In fact, desaturation and hypotension may be considered a reflection of the patients’ limited physiological reserve rather than a complication associated with the intubation per se. The reported complication rate of emergency intubations is variable, ranging from 4.2% to 39%.7–15
Time of day of intubation
Although one may presume that patients are likely to be acutely unwell at any time of the day requiring emergency intubations, we found that the frequency of emergency intubations was significantly less during weekday and weekend out of hours compared to in hours. The frequency of intubations on weekdays and weekends, however, was similar. The distribution of emergency intubation timings is probably reflective of intensivist practice given the similarity with the reported literature.15,22 This may represent improved planning and anticipation of the deteriorating of patients requiring emergency intubation; as recommended by the NAP4 audit. 2
Emergency intubations occurring out of hours tended to be in patients who have a higher ASA grade (a surrogate of illness severity). These intubations were more likely to be done independently, although not associated with a greater number of complications. This remains reassuring and suggests that current workforce planning provides adequately airway-trained staffing levels round the clock. Consistent with this, emergency ICU admissions out of hours are not associated with an increased mortality. 6
Capnography
There were disproportionately more complications associated with emergency intubations on the wards compared to other locations, although this did not reach statistical significance (p = 0.065). This is likely to be secondary to the greater illness severity of ward patients (with ASA grade and pre-intubation GCS as surrogates of illness severity). However, almost all cases where capnography was not used were on the wards. This is of concern following NAP4 and ICS guidelines.2,3 Although it is reassuring to see high uptake in locations where intubations are a common occurrence, the reduction of uptake on wards should not be viewed as acceptable given ease of portability of the equipment. Conversely, it is reassuring to see a vast improvement in the uptake of capnography from the survey by Simpson et al. (54%). 15 Further investment of training and resource is required to ensure capnography is used following emergency intubations on the ward.
Use of drugs
Traditionally, suxamethonium and thiopentone were the favoured choices for rapid sequence intubations (RSIs). Historically, anaesthetists report preference for use of thiopentone (88%) compared to propofol (58%), and etomidate (54%) in RSIs. 23 A recent survey of current UK practice suggests a shift towards the use of propofol (with or without opiates) and rocuronium to achieve adequate sedation and paralysis, respectively. 24 This may represent greater familiarity with propofol. We confirm these findings with most intubations performed with propofol and only minority with thiopentone (alone or in conjunction with another induction agent). The concurrent use of opiates is common, with fentanyl proving the more popular option.
Our data suggest that rocuronium is now the most popular choice of NMB among intensivists being used in over half of intubations, with suxamethonium accounting for a third. A recent survey suggests that the use of rocuronium is growing, though suxamethonium is still commonly used. 24 We speculate that the increased use of rocuronium compared to suxamethonium may be in part related to the ability to reverse the effects of rocuronium with suggamadex and the perceived complications associated with suxamethonium. The use of suggamadex in a timely manner with adequate efficacy during a difficult emergency intubation has been described in case reports.25,26 However, clinical trials are lacking.
Limitations and strengths of our study
Potential sources of bias in our data arise primarily from the self-reported nature of our data, data may be entered retrospectively and may be prone to recall bias of events/techniques. Furthermore, we do not have data on what proportion of the total number intubations performed by intensive care medicine trainees nationally this represents. Acknowledging that we are reporting perhaps a minority of all intubations in critically ill patients, we do not feel these sources of bias are significant, especially given the similarity in patient demographics, complication rates, and airway difficulties, with the reported literature.6–15
It should also be noted that the database used to store this data is derived from intensive care trainees as opposed to anaesthetics trainees and as such will be missing out on cohorts of patients in hospitals where the anaesthetics teams provide out of hours airway cover, and not intensive care. We lack data on a number of strategies to improve the success rates of intubation including pre-oxygenation, maintenance of oxygenation, device selection, and human factors.27,28 We do not account for the level of variations in hospitals. The reasons for intubation, use of cricoid pressure, and use of rescue techniques are also relevant information that is beyond the scope of the database.
Despite these limitations, we capture useful information regarding differences in practice by time of day/day of week and location. Such data capture is important for workforce planning. Intubation practice performed by intensive care medicine trainees has not been previously described to this level of detail.
Conclusion
The incidence of clinically significant complications associated with emergency intubations is not insignificant. Our data confirm the association between the CL airway grade, the number of attempts at intubation and subsequently the incidence of complications. However, the lack of association between complications and time of day/day of week, or ASA grade is encouraging, suggesting that adequate trained staff is available throughout the working week. Individualisation of drug choices for emergency intubations may intuitively be safer, though clinical trials are needed to confirm this. With oldest and sickest patients on the wards, the significant reduction in usage of capnography needs to be addressed. Emergency/outreach staffing levels on weekends are crucial given the similar frequency of emergency intubations on weekday daytime and weekends.
Authors' contributions
NA and CSM contributed equally to this study. NA and KA created and maintained the online trainee logbook. NA and KA conceived the study idea and designed the study. KA extracted the data from the database. NA drafted the statistical analysis plan and performed the analyses. NA and CSM drafted the manuscript. All authors critically revised the manuscript for important intellectual content. All authors had full access to all of the data in the study, take responsibility for the integrity of the data and the accuracy of the data analysis. BJP and MC supervised the project, participated in the data analysis and interpretation, in writing and editing the manuscript. All authors read and approved the final version of the manuscript.
Availability of data and material
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: NA and KA have designed and created the online database. NA and KA own the database and have access to the data.
Ethics approval and consent to participate
All users accepted the terms and conditions on registering that “all data entered will be aggregated into a database for the purpose of research and audit. This may be published or presented in a public domain (e.g. conferences, journals, online). MedELogbook has the right to use any data entered for this purpose. This database will not be used to interrogate the data entered by individual users”. Under Section 251 of the NHS Act 2006, NHS Health Research Authority ethical approval is not required as no patient identifiable information is used. The local Research Governance & Regulatory Assurance Manager at St George’s NHS Healthcare Trust, confirmed that no ethics approval was required.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.